Pattern and Clinical Characteristics of Cystic Kidney Disease Patients in a Tertiary Centre, South-West Nigeria: A Retrospective Study
Background: Cystic kidney disease is a group of disorders that are characterized by the formation of cysts in the kidneys.It is a major cause of end-stage renal disease (ESRD) worldwide. Objectives: This study aimed to determine the pattern and clinical characteristics of patients with cystic kidney disease who presented at a tertiary hospital in South-West Nigeria. Methods and Materials: We reviewed the records of patients admitted with cystic kidney disease over an 8-year period at Ekiti State University Teaching Hospital. Data extracted included patients’ demographics, clinical presentations, and treatment outcomes. We compared the data between patients with ADPKD and other types of kidney cysts and summarised the treatment outcomes among the patients. Result: The prevalence of cystic kidney disease was 9.2% and the mean age of the patients was 52.87 years with a male predominance. The most common type of kidney cyst was simple renal cysts (53.2%), followed by ADPKD (40.4%). Incidental findings with no symptoms were the most common mode of presentation (61.7%), followed by abdominal pain (38.3%) and palpable abdominal swelling (36.2%). Nephrolithiasis was documented in 4.3% while the frequency of hypertension, haematuria and urinary tract infection was 55.3%, 14.9% and 8.5 %respectively. More than one in five ADPKD patients (21.1%) developed end-stage renal disease. Overall, the majority 41(87.2%) were managed conservatively. Conclusion: This study contributes valuable insights into the pattern and clinical features of cystic kidney disease in South- West Nigeria, further enriching the existing data on this condition within the region.
Introduction
Cystic kidney disease is a group of disorders characterised by the formation of fluid-filled sacs, or cysts, within the kidneys. As these cysts expand, they can impair kidney function, ultimately leading to chronic kidney disease, kidney failure, and various complications [1]. The reported prevalence of ADPKD in the United States ranges from 2.34 to 4.3 per 10,000 people [1, 2]. In Africa, the epidemiology of kidney cysts has received less attention in the global literature. However, the African continent presents a unique set of circumstances, such as differences in genetic predisposition, environmental factors, and healthcare infrastructure, which may influence the prevalence and characteristics of kidney cysts. As Africa faces unique challenges in healthcare delivery and resource allocation, understanding the epidemiology of kidney cysts in this context is crucial for tailoring appropriate diagnostic and treatment approaches to meet the specific needs of the population [3]. Unfortunately, there is currently no cure for cystic kidney disease, and available treatments mainly focus on managing its symptoms. The study is aimed to determine the pattern and clinical characteristics of patients with cystic kidney disease that present at Ekiti State University Teaching Hospital, South-West Nigeria over 8 years.
Materials and Methods
This was an observational, descriptive and retrospective study. We reviewed the records of patients admitted with cystic kidney disease from 1st October 2015 to 30th September 2022 at Ekiti State University Teaching Hospital, Ado-Ekiti, Nigeria. Data extracted include patients’ demography, clinical presentation and treatment outcome. Patients with unconfirmed diagnoses and /or incomplete data were excluded. Ethical clearance for the conduct of the research was obtained from the ethics and research committee of the hospital.
| Variables | ADPKD n=19 | Other Types n=28 | P-value |
|---|---|---|---|
| Age (years) | 55.85±17.55 | 50.86±16.06 | 0.322 |
| Gender (male/female) | 12/7 | 13/15 | 0.259 |
| Systolic BP (mmHg) | 145.11±22.71 | 128.64±15.30 | 0.005 |
| Diastolic BP (mmHg) | 88.42±15.30 | 79.43±10.62 | 0.337 |
| Right kidney size (cm) | 15.87±2.64 | 13.33±2.81 | 0.01 |
| Left kidney size (cm ) | 15.17±2.95 | 12.90±2.17 | 0.009 |
| Sodium (mmol/L) | 136.19±4.69 | 136.52±3.83 | 0.001 |
| PCV(%) | 33.47±9.37 | 38.79±5.56 | 0.217 |
| BMI (Kg/m2) | 25.65±2.64 | 25.99±2.14 | 0.785 |
| Creatinine (µmol/L)# | 111.00(67-1200) | 74.40(56-202) | 0.01 |
| eGFR(mL/min/1.73m2) | 54.26±37.36 | 89.37±30.84 | 0.001 |
Table 1: Comparison of Patients with ADPKD and Other Cyst Types.
#=median (IQR) Table 1: Comparison of Patients with ADPKD and Other Cyst Types.
Statistical Analysis
Data analysis was done using Statistical Package for Social Sciences (SPSS) version 25. Using Pearson’s Chi- Square and Student’s t-test respectively, we compared the frequencies of categorical and means of continuous variables between patients with ADPKD and other types of kidney cysts and summarised the treatment outcome among the patients. Tables and chat were used to present the data. A p-value of ≤0.05 was taken as statistically significant.
Results
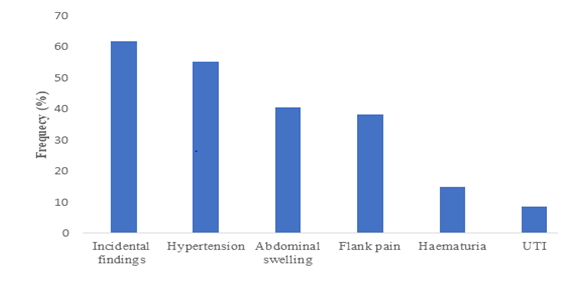
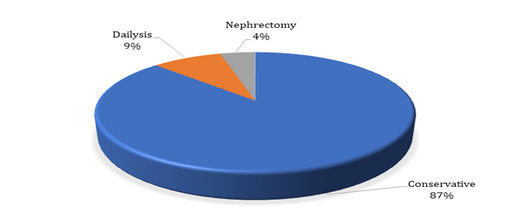
Forty-seven out of 512 patients with renal diseases managed during the period under consideration had cystic kidney disease accounting for 9.2%. The age range of the patients was 16-87 years with a mean age of 52.9 ±16.8 years and a male-to-female ratio of 1.1:1.0. The majority of patients 25(53.2%) had simple renal cysts (Table 1). Polycystic kidney disease (PKD), suspected to be autosomal dominant polycystic kidney disease (ADPKD), and complex cysts were seen in 40.4% and 6.4% of patients, respectively. Among the patients diagnosed with multicystic kidney disease, one patient (2.1%) had cystic renal carcinoma. The frequency of haematuria and urinary tract infection (UTI) was low among the patients (14.9% and 8.5%). Among all the patients, hypertension was diagnosed in 26(55.3%), of which 17(89.5%) were ADPKD patients. Four (21.1%) ADPKD patients developed ESRD and were started on dialysis. Among the four ADPKD patients who underwent brain CT scans, only one (25.0%) showed abnormal features suggestive of a berry aneurysm. This patient also had chamber dilation and valve incompetence on echocardiography. Nephrolithiasis was diagnosed in 2 (4.3%) patients, one of whom had a complication of pyelonephritis. Incidental findings with no symptoms were the most common mode of presentation in about 29(61.7%), closely followed by abdominal pain and palpable abdominal swelling in 18(38.3%) and 17(36.2%) respectively. The mode of treatment was conservative management in the majority 41(87.2%) of the patients while 4(8.5%) were placed on dialysis and 2(4.3%) had nephrectomy (Figures 1,2).
Discussion
Cystic kidney disease is a common cause of morbidity and mortality worldwide. The present study describes the pattern and clinical characteristics of cystic kidney disease patients in a tertiary hospital in South-West Nigeria. The findings of this local study are similar to other studies conducted in Nigeria and some other parts of the world. Our observed prevalence (9.2%) was higher than a similar local report in Lagos, Nigeria [4] and the report of Mosharafa in the Middle East [5] but lower than the findings from Ilorin, Nigeria [6]. Mensel, et al. in their work on the assessment of prevalence and size and associated risk factors for renal cysts among the general population of Pomerania in central Europe , showed that the prevalence of renal cysts was 27% with a male predominance [7]. The observed differences in the reported prevalence may be due to the timing and method of diagnosis, as well as access to specialists capable of recognizing early signs of cystic kidney disease. In addition, estimating the prevalence of kidney cysts in the population may be particularly challenging, since early-stage disease can remain asymptomatic and undiagnosed for many years.
The mean age of the patients in our study falls within the middle age group, consistent with the finding of Awoonidanla, et al. [4] Cystic kidney disease can occur in any age group depending on the specific type and causative genes. In agreement with previous studies, we found that the disease is more common in males and that the prevalence increases with age [4, 6, 7]. However, this contrasts with a previous study by Willey, et al. [1], which found that young women were diagnosed with autosomal dominant polycystic kidney disease (ADPKD) at nearly twice the rate of young men. This difference was attributed to the increased use of ultrasound in women during their childbearing years.
Most of our patients had simple renal cysts, followed by ADPKD. Complex cysts were less common. However, one patient with multicystic kidney disease was found to have cystic renal carcinoma. This finding highlights the importance of careful clinical evaluation and diagnostic imaging in patients with cystic kidney disease, even if they have a benign-appearing cyst [8].
While we found simple renal cysts as the most common, it has previously been documented that ADPKD was the most common [4]. There are however racial and methodological differences in the study population. Cystic kidney disease has been recognized through the advancement in sequencing techniques as a complex genetic disease with over 100 genes involved [9]. Despite these complex genetic links, most of the protein products of the identified genes are linked to the generation and function of the primary cilia, hence, cystic kidney disease complex is defined as ciliopathy [9]. The latter underscores the crucial role of genetic testing in the evaluation of cystic kidney disease.
In terms of clinical presentation, incidental finding with no apparent symptoms was the most common in this study. This underscores the importance of routine health check-ups and diagnostic imaging in detecting cystic kidney disease in asymptomatic individuals. Other common modes of presentation included abdominal pain, hypertension, and palpable abdominal masses. These symptoms are in line with typical manifestations of cystic kidney disease, emphasizing the need for early diagnosis and intervention [1, 4, 7, 10, 11].
Systemic hypertension and end-stage renal disease (ESRD) are common complications of ADPKD, regardless of the genetic mutation variant. Patients with PKD1 genotype tend to develop these complications at a younger age than those with PKD2 mutation [3, 8, 12, 13].
For simple renal cysts, the presentation is mostly asymptomatic [11]. majority of our patients in this study had simple renal cysts which explains why the commonest mode of presentation in this index study is incidental finding since they were asymptomatic. Simple renal cysts can also present with systemic hypertension and haematuria consistent with the observation in this study [10]. Other modes of clinical presentation for simple renal cysts include flank pain and urinary obstruction [10]. A rare presentation of small bowel obstruction has also been reported [14].
Although relatively few patients in our study had complex renal cysts, the detection of such cysts has increased dramatically in recent decades due to the increased use of high-resolution imaging facilities [15]. Complex renal cysts can present with haemorrhage (painful or painless haematuria), infection, or malignancy [16]. It is important to differentiate between benign and malignant complex renal cysts. Beyond computed tomography (CT), which is the gold standard for diagnosis, other promising modalities include contrast-enhanced ultrasonography and percutaneous biopsy [16].
Differentiating between benign and malignant complex renal cysts is crucial for determining the best management approach. However, the expertise and facilities required for this costly diagnostic modality are not available in most hospitals in Nigeria. Therefore, it is important to have a high index of suspicion for complex renal cysts and to refer patients to tertiary facilities whenever cystic kidney disease is detected, either incidentally in asymptomatic patients or in those who present with symptoms.
Renal and extra-renal complications are common in cystic kidney disease [12, 17]. This study found that some patients had pyelonephritis and nephrolithiasis, and one patient had valvular heart disease. The management of cystic kidney disease depends on the presentation and complications and can include symptomatic (conservative) treatment, renal replacement therapy, or nephrectomy. Lifestyle modifications, such as weight reduction, smoking cessation, maintaining a normal BMI, reducing sodium intake, regular physical exercise and blood pressure control have been shown to slow cyst growth and decline in kidney function including reduction in cardiovascular risk [18].
Tolvaptan is an oral vasopressin antagonist that can be used in patients with ADPKD to reduce the risk of progression to ESRD [19]. It has been shown to reduce the decline in eGFR by about 1ml/min/1.73m²/year [19]. Renal replacement therapy is indicated for patients who progress to ESRD, and this can be dialysis or kidney transplantation. Two of our patients had nephrectomy; native nephrectomy can be indicated in ADPKD if symptoms are related to the size of the native kidneys (pressure symptoms), if there is a need to create space for kidney transplantation, recurrent cyst infection, intractable haematuria, pain, weight loss or suspicion of malignancy [20].
The prognosis of cystic kidney disease is dependent on the specific type, the underlying genetic mutation, extra- renal and renal complications. Cystic kidney disease can cause a range of potential complications, the nature and severity of which depend on the specific type of kidney cyst involved. Simple renal cysts, though generally benign can cause haematuria, abdominal mass and pain due to cystic rupture and infections in addition to hypertension [3]. There has also been a report of massive renal cysts displacing intra-abdominal structures [21]. Cystic renal carcinoma can sometimes be misdiagnosed as a benign renal cyst; however, it has an excellent prognosis regardless of tumour size [8, 12]. In ADPKD, there is a progressive decline in renal function leading to end-stage renal disease [12].
Conclusion
Our study indicates that cystic kidney disease is not an uncommon disease condition in our population and the incidence is on the increase. Efforts should be geared toward early diagnosis and family screening of affected patients.
Study Limitations
The limitations of this study include the use of retrospective data from medical records which may introduce bias and limitations in data accuracy and completeness. Similarly, the study was conducted at a single tertiary centre in South-West Nigeria, which might not fully represent the broader population’s diversity and may limit the generalizability of the findings to other regions or healthcare settings. The small sample size could impact the precision and statistical power of the results.
References
-
Willey C, Kamat S, Stellhorn R, Blais J (2019) Analysis of Nationwide Data to Determine the Incidence and Diagnosed Prevalence of Autosomal Dominant Polycystic Kidney Disease in the USA: 2013-2015. Kidney Dis (Basel) 5(2): 107-117.
-
Willey C, Gauthier-Loiselle M, Cloutier M, Shi S, Maitland J, et al. (2021) Regional variations in prevalence and severity of autosomal dominant polycystic kidney disease in the United States. Current medical research and opinion 37(7): 1155-1162.
-
Arogundade FA, Akinbodewa AA, Sanusi AA, Okunola O, Hassan MO, et al. (2018) Clinical presentation and outcome of autosomal dominant polycystic kidney disease in Nigeria. Afr Health Sci 18(3): 671-680.
-
Awoonidanla O, Amisu M, Awobusuyi J, Umeizudike T, Onyido O, et al. (2014) Prevalence and clinical presentation of cystic kidney diseases at lagos state university teaching hospital. Tropical journal of nephrology 9(1&2): 31-34.
-
Mosharafa AA (2008) Prevalence of renal cysts in a Middle-Eastern population: an evaluation of characteristics and risk factors. BJU international 101(6): 736-738.
-
Chijioke A, Aderibigbe A, Olarenwaju TO, Makusidi AM, Oguntoyinbo AE, et al. (2010) Prevalence and pattern of cystic kidney diseases in Ilorin, Nigeria. Saudi journal of kidney diseases and Transplantation 21(6): 1172-1178.
-
Mensel B, Kühn JP, Kracht F, Völzke H, Lieb W, et al. (2018) Prevalence of renal cysts and association with risk factors in a general population: an MRI-based study. Abdominal radiology (New York) 43(11): 3068-3074.
-
Chebib FT, Torres VE (2016) Autosomal Dominant Polycystic Kidney Disease: Core Curriculum 2016. American journal of kidney diseases: the official journal of the National Kidney Foundation 67(5): 792-810.
-
Braun DA, Hildebrandt F (2017) Ciliopathies. Cold Spring Harbor perspectives in biology 9(3): a028191.
-
Bas O, Nalbant I, Sener NC, Firat H, Yeşil S, et al. (2015) Management of renal cysts. JSLS 19(1): e2014.00097.
-
Koh C, Cserni T, Hawkes R, Dickson A, Hennayake S, et al. (2018) The management of symptomatic simple renal cysts in children. Journal of Pediatric Surgery Case Reports 28: 21-29.
-
Chapman AB, Devuyst O, Eckardt KU, Gansevoort RT, Harris T, et al. (2015) Autosomal-dominant polycystic kidney disease (ADPKD): executive summary from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 88(1): 17-27.
-
Wilson PD (2004) Polycystic kidney disease. The New England journal of medicine 350(2): 151-164.
-
Sadeghi A, Shahrbaf MA, Asadzadeh Aghdaei H, Esmaeilinejad K, et al. (2018) A rare presentation of simple renal cyst: gastrointestinal obstruction. Gastroenterology and hepatology from bed to bench 11(4): 359-362.
-
McGuire BB, Fitzpatrick JM (2010) The diagnosis and management of complex renal cysts. Current opinion in urology 20(5): 349-354
-
Bisceglia M, Galliani CA, Senger C, Stallone C (2006) Renal cystic diseases: a review. Advances in anatomic pathology 13(1): 26-56.
-
Keith DS, Torres VE, King BF, Zincki H (1994) Renal cell carcinoma in autosomal dominant polycystic kidney disease. Journal of the American Society of Nephrology 4(9): 1661-1669.
-
Rangan GK, Alexander SI, Campbell KL, Dexter MA, Lee VW, et al. (2016) KHA-CARI guideline recommendations for the diagnosis and management of autosomal dominant polycystic kidney disease. Nephrology 21(8): 705-716.
-
Torres VE, Gansevoort RT, Czerwiec FS (2018) Tolvaptan in Later-Stage Polycystic Kidney Disease. The New England Journal of Medicine 378(5): 489-490.
-
Patel P, Horsfield C, Compton F, Taylor J, Koffman G (2011) Native nephrectomy in transplant patients with autosomal dominant polycystic kidney disease. Annals of the Royal College of Surgeons of England 93(5): 391- 395.
-
Khalid MG, Zarm MA, Velez JQ, Mohamed MMB (2023) Massive renal cyst displacing intra-abdominal structures. Ochsner Journal 23(3): 262-265.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report