Case Report - Parvovirus B19 Pure Red Cells Aplasia after Kidney Transplantation
Parvovirus B19, a member of the Parvoviridae family, is known for causing various clinical manifestations, including erythema infectiosum and arthropathy. However, its association with pure red cell aplasia (PRCA) following solid organ transplantation remains relatively uncommon. We present a case report detailing the occurrence of Parvovirus B19-induced PRCA in a patient who underwent kidney transplantation – a 48 years old man who had history of hypertension and gout who received a kidney from living donor. The patient presented in the clinic with severe anemia, dizziness, headache and swollen lymph nodes which later on was proved to be result from the viral infection. This case underscores the importance of considering Parvovirus B19 as a potential etiological factor in the development of PRCA post-kidney transplantation. Clinicians should maintain a high index of suspicion for viral-induced complications in immunocompromised transplant recipients, as timely diagnosis and appropriate management are crucial for optimal patient outcomes. This case report contributes to the limited existing literature on Parvovirus B19-associated PRCA in the context of solid organ transplantation, emphasizing the need for heightened awareness and vigilance in post-transplant care.
Introduction
One of the predisposing factors for anemia after kidney transplantation are the immunosuppression regimens [1]. The recipient humoral response inhibition provides an ideal environment for the activation of opportunistic viral pathogens. Abnormalities from pure red cell aplasia (PRCA) are limited to the red cell lineage. PRCA is a syndrome defined by a normocytic normochromic anemia with severe reticulocytopenia and marked reduction or absence of erythroid precursors from the bone marrow. Acquired PRCA may be either a primary disorder or secondary to some other disorder or agent.
Primary acquired PRCA is an autoimmune disorder that is frequently antibody-mediated. Secondary acquired PRCA may be associated with collagen vascular/autoimmune disorders such as systemic lupus erythematosus, lymphoproliferative disorders such as chronic lymphocytic leukemia or large granular lymphocyte leukemia, infections particularly B19 parvovirus [2], cytomegalovirus, thymoma and other solid tumors or a variety of other disorders, drugs, or toxic agents. The bone marrow aspiration biopsy demonstrated normocellularity, normal myeloid and megakaryocyte maturation and decreased erythroid lineage - <5% erythroblasts on the marrow differential count [2, 3].
Parvovirus B19 (PVB19) is a DNA virus which causes clinically relevant infection in renal transplant recipients leading to significant morbidity PVB19 infection is quite likely the cause of refractory normocytic anemia after kidney transplantation (KT). PVB19 affects rapidly dividing cells such as bone marrow erythrocyte progenitors causing normochromic normocytic anemia with a low reticulocyte percentage, normal leucocyte and platelets and absence of erythrocyte progenitors and that can be found when bone marrow biopsy is done. The diagnosis is based on positive PVB19 DNA polymerase chain reaction (PCR) [4]. The major challenge in managing and preventing the infection after KT involves management of the decreased level of immunosuppression and controlling the risk of rejection of the allograft. Number of papers have proved the importance of PVB19 infection after KT and the need of adequate immunosuppressive treatment in KT patients especially for those with anemia [5, 6], because infections with parvovirus PVB19 can cause significant morbidity in transplant recipients [7].
It is important to point out that treatment of Parvovirus B19-associated PRCA after kidney transplantation should be considered in accordance with the individual patient’s condition and decisions should be made in collaboration with a transplant specialist and an infectious disease expert. Early detection and intervention are crucial for better prognosis.
Case Report
A 48-old man with history of gout and hypertension received a kidney from living donor in July 2020. Renal biopsy was not performed, because of contraindications – the patient had low platelet count or prolonged clotting time. From point of view of the family history the patient had son with hyperuricemia with proven mutation in UMOD (uromodulin) gene. He had no other comorbidities and no other operative treatment in the past. After the transplantation was performed the postoperative period was smooth and the patient had no complications. Induction with Antithymocyte globulin (ATG) was used. For the first 24 hours the urine output was good with no complications. The induced immunosuppression therapy was: Tacrolimus (drug monitored value 9.0 ng/ml), Mycophenolate mofetil (MMF) as second immunosuppressant (2000mg/daily dosage) and also Prednisolone 10 mg was prescribed. After the kidney transplantation serum creatinine decreased to 150 µmol/l and the calculated eGFR (CKD-EPI 2021) was 50ml/min and kept in this range for the rest of the stay in the hospital.
Three months after KT the laboratory test demonstrated normochromic, normocytic anemia with hemoglobin concentration decreased to 48 g/L. The patient complained for weakness, fatigue and shortness of breath during physical activity. He had several blood transfusions which proceeded normally and without complications. Virology tests were performed and the results for CMV, EBV, BKV tests came out negative. Negative results were received from the test for HBV, HCV, HEV markers.
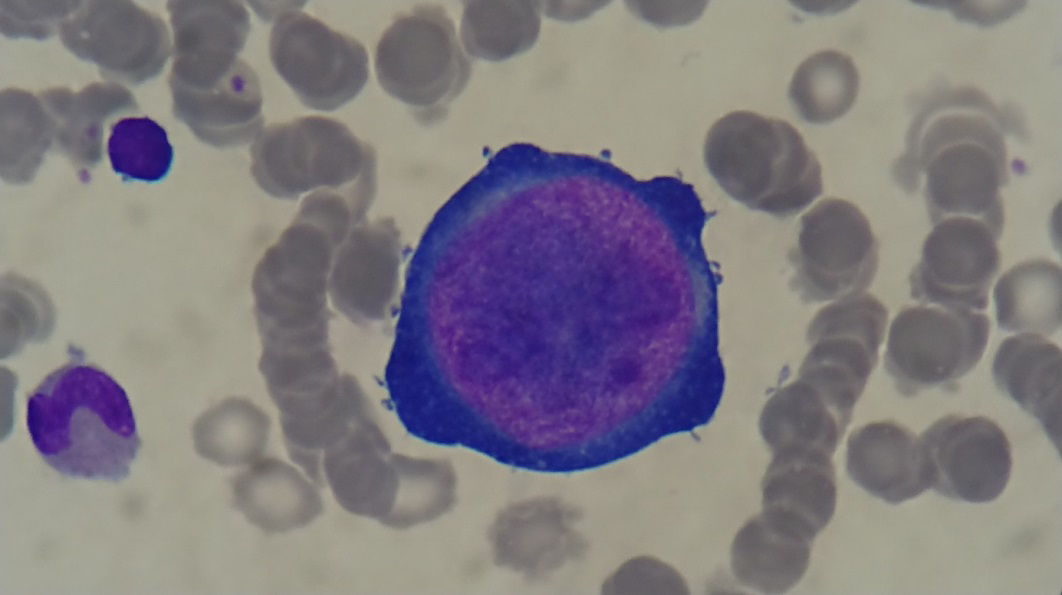
After a consilium, it was assessed that the therapy with MMF must be stopped and was decided that a conversion from Tacrolimus (TAC) to Cyclosporine A (CsA) must be done, but no improvement was found. In the hematology ward a bone marrow biopsy was performed and the result demonstrated pure red cell aplasia with typical giant pro-erythroblasts with nuclear viral inclusions. This result suggested that the patient has PVB19 infection (Figure 1).
Based on bone marrow findings test from the blood serum for PV19 was performed. IgG and IgM antibodies came out negative. The diagnose was confirmed with positive PCR DNA Parvovirus B 19 (more than 20 000 000 UI/ml) in December 2020. After receiving the results it was decided that a course of intravenous immunoglobulin (IVIG) will be administered and the used in dosage was 2 g/kg and was divided for 5 days. Four days after the end of the course of IVIG treatment, after a manual blood smear was performed and was reported an increase in reticulocytes count. Later on a slow increase in hemoglobin, hematocrit, erythrocytes was reported. Table 1 from nephrological point of view there was temporary decreased GFR level after IVIG infusion.
Three months after IVIG the patient was in stable condition with no complaints. Hemoglobin was 123 g/l with improved renal function - eGRF (CKD-EPI 2021) was 53ml/min. Six months after the recovery a PCR-test for DNA Parvovirus B19 was performed and the result was negative and treatment with Tacrolimus, MMF and peroral corticosteroid was restored. At the end of the first year after IVIG therapy Hb (g/L), Hct (%), reticulocytes count were normal and the renal function was stable with results similar to the ones that the patient had after transplantation. Nowadays PCR test for PVB19 remains negative (Table 2).
| Hb g/l | Ht % | Er x1012/l | Leu x 109/l | Pl x109/l | Ret x109/l | Creat μmol/l | Urea mmol/l | |
|---|---|---|---|---|---|---|---|---|
| Oct-20 | 47 | 18 | 1.7 | 10.9 | 322 | 179 | 9.8 | |
| After transfusion | 64 | 20 | 2.3 | 9.9 | 277 | 5 | ||
| Nov-20 | 56 | 17 | 2 | 10.5 | 415 | 159 | 9.4 | |
| Nov-20 | 71 | 22 | 2.5 | 9.3 | 394 | |||
| Dec-20 | 52 | 16 | 1.9 | 17.7 | 356 | 204 | ||
| After bood transfusion | 70 | 22 | 2.6 | 16.6 | 244 | 148 | 15.8 | |
| Before IVIG | 69 | 21 | 2.4 | 8.9 | 193 | 4 | 141 | 6.1 |
| transfusion | 69 | 21 | 2.4 | 8.9 | 193 | 4 | 141 | 6.1 |
| Course of IVIG from 10.01.21-14.01.21 | ||||||||
| 18.01.21 | 83 | 26 | 2.9 | 11.7 | 205 | 142 | 161 | 6.5 |
| 18.01.21 | 98 | 31 | 3.3 | 7.9 | 202 | 6.40% | 151 | 8.2 |
| Feb-21 | 123 | 40 | 4.3 | 15.4 | 301 | 138 | 7.2 | |
| Mar-22 | 145 | 42 | 4.8 | 12 | 143 | 7,4% | 143 | 6.9 |
Table 1: Laboratory date during the following period.
| Date | Reticulocyte |
| 09.01.2021 before IVIG | 4.10 x10^9/l |
| 20.01.2021 | 142.60 x10^9/l |
| 21.01.2021 | 177.00 x10^9/l |
| 20.03.2021 | 185.00 x10^9/l |
Table 2: Reticulocytes during the examined period.
Discussion
PV B19 infection is a rare, but severe complication after KT. The total incidence of PVB19 DNA positive test in KT patients is estimated at 10.3% and PVB19-PCR occurred in only 3% [8]. The viral infection should be excluded with PVB19 PCR in patient with normochromic normocytic anemia after transplantation or in immunosuppressive treatment [9, 10]. If serology or PCR tests are negative, but the clinical suspicion is high, examination of bone marrow specimen is helpful in establishing the diagnosis [8, 11]. The bone marrow biopsy is a required procedure with high informative value for the diagnosis. The typical giant pro- erythroblasts with nuclear viral inclusions in bone marrow biopsy suggests PVB19 infection.
There is no specific antiviral therapy available to treat PVB19 infection. Options in KT patients include: IVIG only, IVGI and decreased immunosuppression, reduction and/ or changes in immunosuppressive therapy and conservative approach, including haemotransfusions [12]. Other papers pointed out that in KT patients PVB19 PRCA had been corrected after a first course of intravenous immunoglobulin in 93% of patients, but approximately one-third relapsed. The calculated mean values from metanalysis were 4.3 months [1, 2, 3, 5, 8].
This case is the first described in Bulgaria. The patient showed excellent response after IVIG therapy with normalization of Hb level, reticulocyte count, with stable renal function and negative viral DNA. The results are stable since 2020 till nowadays. For the observed period no recurrence of infection was reported, allowing the patient to have baseline immunosuppression. IVIG has been widely used and appears to be beneficial in a substantial number of kidney recipients with PRCA related PVB19 infection [12, 13].
Although parvovirus B19 infection can cause various complications in adults, including haematological disorders. In cases of suspected complications associated with Parvovirus B19 we ordered a range of laboratory tests to aid diagnosis and differential diagnosis. The tests included total and direct bilirubin, LDH, iron, and ferritin. They came in the normal range.
However, the optimal duration and dosing regimen of IVIG therapy for PV B19 infection have yet to be established. The effective rate of IVIG reached 93-95%, but the recurrence rate is between 22-33% [14]. A decrease in immunosuppression load is reasonable, but only under control for rejection symptoms. Modalities used in immunosuppression regimen in PVB19 related PRCA should depend on the patient’s transplantation history [15], on their results from the blood count and the scheme that is chosen for the treatment [16, 17, 18, 19, 20, 21].
Conclusion
PVB19 is serious, but treatable cause of anemia in renal transplanted patients. A high index of suspicion should be maintained in patients with anemia in the posttransplant phase, especially those who have received higher doses of immunosuppressants. It may be relevant to perform a screening for selected donors for asymptomatic PVB19 infection and be closely monitored for anemia if the donor has the infection. Further studies on a larger group of patients are required to determine whether recommendations for routine donor screening need to be made. Early diagnosis and appropriate intervention can minimize the negative impacts of the viral infection.
References
-
Vanrenterghem Y (2009) Anemia after kidney transplantation. Transplantation 87(9): 1265-1267.
-
Sawada K, Fujishima N, Hirokawa M (2008) Acquired pure red cell aplasia: updated review of treatment. Br J Haematol 142(4): 505-514.
-
Means RT (2016) Pure red cell aplasia. Blood 128(21): 2504-2509.
-
Servant-Delmas A, Morinet F (2016) Update of the human parvovirus B19 biology. Transfus Clin Biol 23(1): 5-12.
-
Thongprayoon C, Khoury NJ, Bathini T, Aeddula NR, Boonpheng B, et al. (2020) Epidemiology of parvovirus B19 and anemia among kidney transplant recipients: a meta-analysis. Urol Ann 12(3): 241-247.
-
An HPH, Diem HT, Cuong NT (2019) Parvovirus B19- associated anemia in kidney transplant recipients: a single-center experience. Transplant Proc 51(8): 2693- 2696.
-
Eid AJ, Brown RA, Patel R, Razonable RR (2006) Parvovirus B19 infection after transplantation: a review of 98 cases. Clin Infect Dis 43(1): 40-48.
-
Srinivas P, Kenneth F, Bal K, Camellia E, Sundaram H (2000) Human parvovirus B19 infection presenting as persistent anemia in renal transplant recipients. Transplantation 69(12): 2666-2669.
-
Xiao C, Wang CX, Liu LS, Fu Q (2013) Clinical investigation of human parvovirus B19 infection after renal transplantation in China. Transplant Proc 45(4): 1593-1599.
-
Waldman M, Kopp JB (2007) Parvovirus-B19-associated complications in renal transplant recipients. Nat Clin Pract Nephrol 3(10): 540-550.
-
Crabol Y, Terrier B, Rozenberg F, Pestre V, Legendre C, et al. (2013) Intravenous immunoglobulin therapy for pure red cell aplasia related to human parvovirus b19 infection: a retrospective study of 10 patients and review of the literature. Clin Infect Dis 56(7): 968-977.
-
Mouthon L, Michel M, Gandre C, Montagnier-Petrissans C, Chevreul K (2015) Costs of intravenous immunoglobulin therapy in patients with unconfirmed Parvovirus B19 pure red cell aplasia. Clin Infect Dis 60(3): 488.
-
Gosset C, Viglietti D, Hue K, Antoine C, Goltz D (2012) How many times can parvovirus B19-related anemia recur in solid organ transplant recipients? Transpl Infect Dis 14(5): E64-E70.
-
Rerolle JP, Morelon E, Helal I, Perald MN, Mamzer- bruneel MF, et al. (2004) Parvovirus B19-related anemia after renal transplantation. Scand J Infect Dis 36(6-7): 513-516.
-
Gregoor PS, Weimar W (2005) Tacrolimus and pure red- cell aplasia. Am J Transplant 5(1): 195-196.
-
Liefeldt L, Buhl M, Schweickert B, Engelmann E, Sezer O, et al. (2002) Eradication of parvovirus B19 infection after renal transplantation requires reduction of immunosuppression and high-dose immunoglobulin therapy. Nephrol Dial Transplant 17(10): 1840-1842.
-
Rocha PT, Gomes CL, Finni P, Andrade JA, Filgueiras R, et al. (2004) Pure red cell aplasia and diabetes mellitus following parvovirus B19 infection in renal transplant recipient. Transplantation 78(2): 491.
-
Gallinella G, Manaresi E, Venturoli S, Grazi GL, Musiani M, et al. (1999) Occurrence and clinical role of A sternal biopsy with typical giant pro-erythroblasts with nuclear viral inclusions points to PV B19 infection active parvovirus B19 infection in transplant recipients. Eur J Clin Microbiol Infect Dis 18(11): 811-813.
-
Landry ML, Hayden RT, Wolk DM, Carroll KC, Tang YW (2016) Parvovirus B19. Microbiol Spectr 4(3).
-
Eid AJ, Chen SF (2013) Human parvovirus B19 in solid organ transplantation. Am J Transplant 13(Suppl 4): 201-205.
-
Pabisiak K, Stepniewska J, Ciechanowski K (2019) Pure Red Cell after Aplasia after kidney transplantation: Parvovirus B19 Culprit or Coincidence? Ann Transplant 24: 123-131.
- Results of 6-Month Follow-Up of Patients After B-Turp and Thulep
- The Effect of Drinking Water with a High Content of Antimony and Arsenic on the Dynamics of their Distribution in the Kidneys and the Renal Excretory Function in Rats
- Effectiveness and Safety of Tansurethral Thulium Laser Enucleation of the Prostate in the Treatment of BPH: Review
- A Systematic Review on Molecular Pathophysiology Involved in Chronic Kidney Disease and the Role of Animal Models in Drug Discovery to Manage in Chronic Kidney Disease - An Update
- Functional Development of Kidneys in Human Ontogenesis
- Testicular Metastasis: Uncommon Prostate Cancer Case Report