Review on Ovine Fasciolosis in Ethiopia
Fasciolosis is one of the major constraint factors for ovine production development in Ethiopia by inflecting direct and indirect loss at different parts of the country. Ovine fasciolosis is an economically important parasitic disease of sheep caused by trematodes species of the genus Fasciola, which migrate in the hepatic parenchyma and establish and develops in the bile ducts.In Ethiopia, both species co-exist at different altitudes. The snails of the genus lymnae are mainly involved as an intermediate host in the life cycle of fasciolosis. Ovine fascioliasis in Ethiopia were losses annually estimated at 48.4 million Ethiopian birr due to mortality, productivity (weight loss and reproductive wastage), and liver condemnation at slaughter. This fasciola disease has three phases of clinical sign acute, sub-acute and chronic forms. Acute fasciolosis occurs as disease outbreak following a massive, but relatively short-term, intake of metacercariae. Death usually results from blood loss due to hemorrhage and tissue destruction caused by the migratory juvenile flukes in the live resulting in traumatic hepatitis. Diagnosis of Fasciolosis is based on clinical sign, grazing history, and seasonal occurrence, examination of feces by laboratory tests and post mortem examination. Treatment of infected animals will largely depend on the correct use of appropriate and registered anthelmintic. Triclabendazole is the most effective anthelmintic drug which can be destroys or kills all stage of fasciola. Fasciolosis may be controlled by reducing the populations of the intermediate snail host, or by appropriate anthelminthic treatment and the population of snail should be destroyed by applying Molluscicide and destroying the environment that suit for snail’s reproduction.
Introduction
Ethiopia is believed to have the largest livestock population in Africa, with an estimated population of
7.8 million of equine, 1million of camels, 476.5 million cattle, 39.6 million chickens, 26.1 million sheep and 21.7 million goats [1]. Small ruminants play a significant role in maintaining household stability by providing meat, milk, skin and wool, generate cash income and play traditional social and religious role [2]. Among the small ruminant in Ethiopia, sheep are the dominant livestock, providing up to 63% of cash income and 23% of the food subsistence value obtained from livestock production productivity [3]. Despite the large size of the Open Access Journal of Veterinary Science & Research
sheep population, the productivity per animal and the contribution of this sub-sector to the national economy is relatively low. Endo-parasitic infections, malnutrition, and management problems are known to be the main factors that affect. The various species of gastro- intestinal and pulmonary nematodes, trematodes, and cestodes are known to be prevalent in Ethiopia, one of the helminthosis that causes immense direct and indirect losses especially in domestic ruminates is fasciolosis [4, 5, 6]. Fasciolosis is known by different local names in various parts of Ethiopia that vary according to the region and language. In Amharic, it is called “Kulkult”, “Wadomma”, “and yegubet tile”. In Afan Oromo, it is known as “Dadao”, “Losha”, and “RammoTiruu”. In Tigray language, it is termed as “Ifil [7]. The economic significant of fasciolosis in the highlands of Ethiopia has been reported by several workers. An estimate of the economic loss due to ovine fasciolosis in the Ethiopian high lands was made based on available data on mortality weight loss, reduced reproductive efficiency and liver condemnation at slaughter. The economic effects of fasciolosis were identified and models for estimating the financial loss presented. Ovine fasciolosis losses were estimated at 48.8million Ethiopian Birr per year of which 46.5%, 48.8% and 4.7% were due to mortality, productivity (weight loss and reproductive wastage) and liver condemnation, respectively [8, 9, 10]. Clinically, it is characterized by a progressive loss of condition and the development of anemia and hypoalbuminaemia which can result in emaciation, pallor mucous membranes, sub mandibular oedema and ascites [11]. Diagnosis is based primarily on clinical sign, seasonal occurrence, and privies history of fasciolosis on the farm or the identification of snail habitats, postmortem examination, hematological tests and examination of faeces for fluke eggs. Even though, it is difficult to detect Fasciola in live animals, liver condemnation at slaughter or necropsy was found to be the most direct, reliable, and cost efficient technique for the diagnosis of fasciolosis [11]. The objective of this review is to understand the general description of ovine fasciolosis and its clinical sign, diagnosis and prevention which concern with recently reported research.
Literature Review
General Description of Ovine Fasciolosis
Fascioliasis is a worldwide zoonosis caused by Fasciola spp. and is often neglected despite its common occurrence in endemic areas and It is caused by two species of parasitic flatworms or trematodes that mainly affect the liver [12, 13, 14].
Aetiology
Fasciolosis is caused by Digenean trematode of the Genus Fasciola consisting of two species usually implicated in causing the disease namely F. hepatica and F. gigantica [12, 15].
| Scientific Classification | |||
|---|---|---|---|
| Kingdom: | Animalia | ||
| Phylum: | Platyhelminthes | ||
| Class: | Trematoda | ||
| Subclass: | Digenea | ||
| Order: | Echinostomida | ||
| Suborder: | Distomata | ||
| Family: | Fasciolidae | ||
| Genus: | Fasciola | ||
| Species: | F. hepatica, F. gigantica |
Open Access Journal of Veterinary Science & Research
operculum with embryonic clear cells, and possess a small knob at their posterior ends [19]. A characteristic of Fasciola egg is yellow-brown in colour, large and oval in shape. It has an indistinct operculum (lid). It contains an unsegmented ovum surrounded by many yolk cells [20]. Recent molecular studies demonstrated that the two species can be properly distinguished by DNA sequencing of ITS1 and ITS2 and also mitochondrial genes of NDI and COI [21, 22].
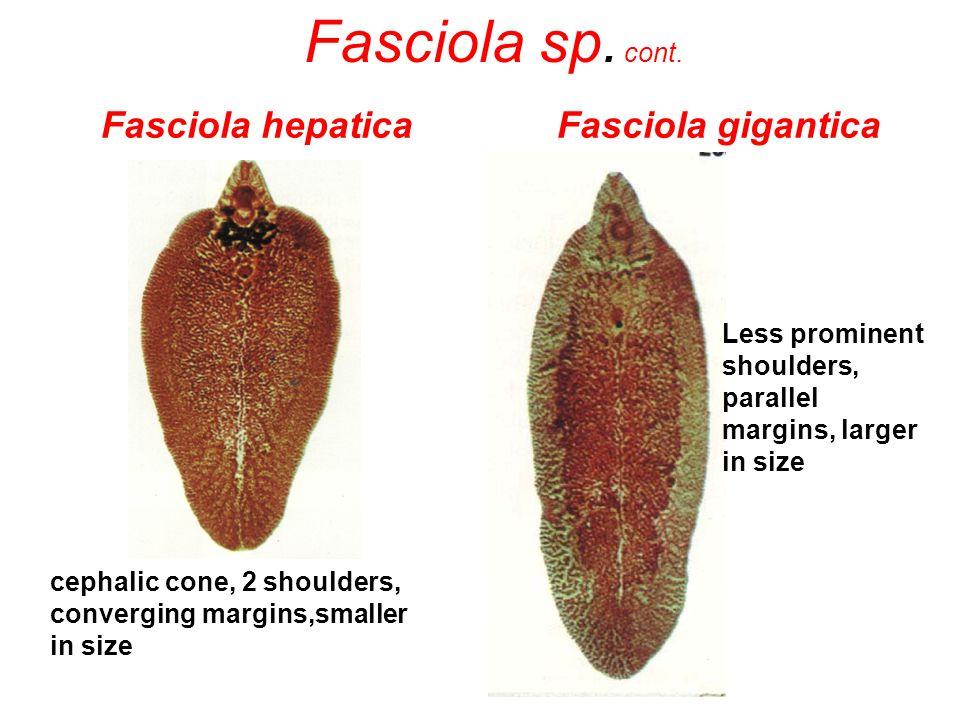
Figure1: Morphology of Fasciola spp.
Epidemiology
The geographical distribution of F. hepatica and F. gigantic is determined mainly by the distribution patterns of the snails that have a role as intermediate hosts [23, 19, 24]. In Ethiopia, both species coexist at different altitudes and transmitted by the snail called Lymnea truncutula and Lymnea natalenesis, respectively. F. hepatica is found in temperate areas and in cooler area of high altitude in the tropics and sub tropics, and F. gigantic is predominantly found in tropics and sub-tropics [15]. In Ethiopia both Fasciola hepatica and Fasciola gigantic have the greatest risk occurred in areas of extended high annual rainfall associated with high soil moisture and surplus water, with risk diminishing in areas of shorter wet season and or lower temperatures. Average annual mean temperature s of 23°C or above were found to correspond to areas below the 1200m elevation limit of Fasciola hepatica in Ethiopia [25].
The main factors determining the timing and severity of Fasciolosis depend on the number of metacercariae accumulating on herbage. Particularly, temperature and rainfall affect both the spatial and temporal abundance of snail hosts and the rate of development of fluke eggs and larvae, the three most important factors that influence the occurrence of Fasciolosis are availability of suitable snail habitat, temperature and moisture [26]. Host range: Intermediate host of Fasciolosis is determined by the number of infected lymnaeid snails in the grazing area, the most important IHs of F. gigantic is L. natalensis and L. auricular [27]. Some Lymnae snails have more aquatic habit than others but most are restricted to damp and Water, land and blocked drainage are hazardous for grazing stock [26, 28]. Snails burrow in to the soil to survive dry periods and release cercaria when free water is present [28]. Final host: Hosts of Fasciola hepatica are most mammals including man, sheep and cattle, cattle being Open Access Journal of Veterinary Science & Research
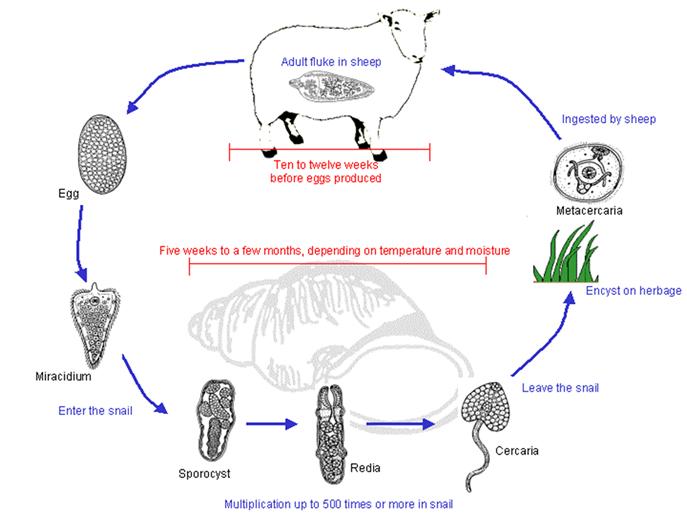
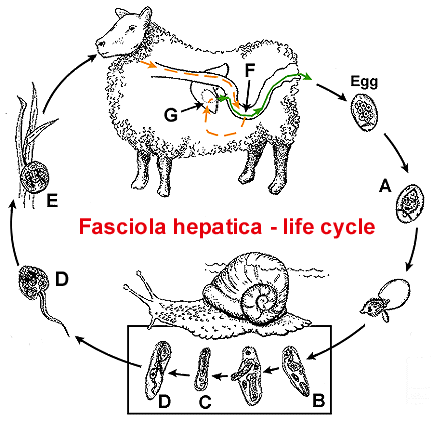
most important. F. gigantic affects a wide range of domestic animals and is found in low land areas replacing F. hepatica. Adult sheep and cattle may remain carriers for many years because of the longevity of the adult flukes [28]. Lifecycle: Infestation with Fasciolosis is usually associated with grazing wet land and drinking from the snail infesting watering places [29]. Adult flukes in the bile duct shed eggs into the bile, which enter to the intestine. Eggs reach the outside by passing down the common bile duct and being voided with feces. The eggs of flukes passed in the feces of mammalian host develop and hatch releasing motile, ciliated miracidium. These takes 9 days at optimum temperature of 22˚C - 26˚Cand little development occurs below 10˚C [30]. The liberated miracidium has a short life span and must locate a suitable snail within 3 hours if successful penetration of the tissue of snail occurs. In infected snails, development proceeds through the sporocyst and rediae stage to the final stage in the IH, the cercaria; these are shed from the snail as motile forms which attach themselves to frame surface, such as grass blades, and insisted there to form the infective metacercariae [15]. It takes a minimum of 6 - 7 weeks for completion of the development from miracidium to metacercariae. Infection of snail with one miracidium can produce over 600 metacercariae. Metacercaria infests the final host and encysted in the small intestine, migrate through the gut wall, cross the peritoneum and penetrate the liver capsule. The young flukes tunnel through the liver parenchyma for 6 - 8 weeks and then enter to the bile duct where they migrate to the large ducts and occasionally the gall bladder. The prepatent period is 10 - 12 weeks [31]. The metacercaria cyst is only moderately resistant, not being able to survive dry conditions. If, however they are maintained in conditions of high humidity and cool temperatures, they may survive for up to a year [7, 24]. Adult flukes can survive for many years in the livers of infected hosts and lay between 20,000 and 50,000 eggs/day. Animals grazing in wet marshy areas, favored the intermediate host, are more likely to become infected. Typically, long and wet seasons are associated with a higher rate of infection. However, sheep are more likely to ingest large numbers of cysts during dry periods following a wet season. This is due to a reduction in available pasture, forcing the animals to graze in swampy areas or in areas where the water has receded, thus exposing them to vegetation heavily infected with metacercaria [32].
Open Access Journal of Veterinary Science & Research
Pathogenesis
The development of fasciolosis infection in definitive host is divided into two phases: the parenchymal (migratory) phase and the biliary phase. The parenchymal phase occurs during migration of flukes in the liver parenchyma and is associated with liver damage and hemorrhage. During the parenchyma stage of the infection, liver damage caused by the migrating flukes compromise liver function, which in sheep is reflected in a decline in plasma albumin concentrations, attributed partly to reduced rate of synthesis and partly to an expansion of the plasma volume [33, 34]. Early infection, during fluke migration, there is hyper proteinemia, hyper globulinemia, and hypo- albuminemia. The hypo-albuminemia is associated with plasma volume expansion caused by liver damage and reduced albumin synthesis. When excysted juvenile flukes penetrate the intestinal wall then flukes migrate within the abdominal cavity and penetrate the liver or other organs. F. hepatica has a strong predilection for the tissues of the liver [33]. The biliary phase occurs when the parasite is in the bile ducts, and results from the hematophagic activity of the adult flukes and from the damage to the mucosa, by their cuticles spines and in biliary ducts, flukes mature, feed on blood, and produce eggs. Hypertrophy of biliary ducts associated with obstruction of the lumen occurs as a result of tissue damage [6]. Thus, a progressive loss of plasma albumin occurs in all infected host species, starting from around the time the fluke commences blood feeding.
Clinical Sign
The clinical features of Fasciolosis can have acute, sub-acute and chronic forms. Acute Fasciolosis occurs as disease outbreak following a massive, but relatively short-term, intake of metacercaria [36].Several clinical Open Access Journal of Veterinary Science & Research
syndromes are acute Fasciolosis in sheep most often occurs as sudden death without other apparent clinical abnormality. Animals suffering from acute Fasciolosis especially sheep and goat, may display no clinical signs prior to death; while some may display abdominal pain and discomfort and may develop jaundice. In some cases, the liver capsule may rupture and fluid may lick into the peritoneal cavity causing death due to peritonitis. More commonly, on ingestion of fewer metacerceriae, fever and eosinophilia is seen [24]. It is usually seen in the summer and autumn but may occur at any time when sheep have the opportunity to graze heavily contaminated herbage. If the disease is observed clinically in sheep it is manifested by dullness, weakness, lack of appetite, pallor and edema of mucosa and conjunctiva and pain when pressure is exerted over the area of the liver [28]. Death usually results from blood loss due to hemorrhage and tissue destruction caused by the migratory juvenile flukes in the liver resulting in traumatic hepatitis. This is more commonly seen in sheep than in other hosts. Sub-acute Fasciolosis is caused by ingestion of a moderate number of metacercariae and is characterized by anemia, jaundice and ill-thrift. The migrating fluke causes extensive tissue damage, hemorrhage and in particular liver damage. The result is severe damage, anemia, liver failure and death 8 - 10 weeks [35, 36]. Chronic Fasciolosis is the most common clinical syndrome in sheep. It occurs when the parasite reaches the hepatic bile duct. The principal effects are bile duct obstruction, destruction of10 liver tissue, hepatic fibrosis and anemia. The onset of clinical signs is slow. Animals become anemic and anorectic, as the adult fluke becomes active within the bile duct and signs may include dependent edema or swelling under the jaw (‘bottle jaw’). Affected animals are reluctant to travel. Death eventually occurs when anemia becomes severe. Additional stress upon anemic animals, such as droving, may lead to collapse and death. Cattle typically present with signs of weight loss, anemia and chronic diarrhea [37]. Chronic Fasciolosis does not become apparent until several weeks after the danger of acute disease has receded. It occurs when the parasite reaches the hepatic bile duct [38].
Diagnosis
Diagnosis of Fasciolosis is based on clinical sign, grazing history, and seasonal occurrence, examination of feces by laboratory tests and post mortem examination [30]. Diagnosis of Fasciolosis may consist of tentative and confirmatory Procedures. A tentative diagnosis of Fasciolosis may be established based on prior knowledge of the epidemiology of the disease in a given environment; observations of clinical signs, information on grazing history, seasonal occurrence and examinations of snails must be considered. Confirmatory diagnosis, however, is based on demonstration of Fasciola eggs through standard examination of feces in the laboratory. Postmortem examination of infected animals may demonstrate of immature and mature flukes in the liver. The latter is helpful in deciding the intensity of infection. Fecal examination as chronic Fasciolosis is diagnosed by finding eggs in the feces by using sedimentation technique. However, they must be distinguishing from the eggs of the other flukes especially the large eggs of paramphistomum. Examination employing sedimentation technique, Fasciola eggs have specific gravity and sedimentation is preferred to floatation [11]. The oval percolated golden eggs of F. hepatica appear in the feces ten weeks after infection, while F. gigantic eggs only appear 15 weeks after infection. Excretion of fluke eggs shows considerable day to day and within day variation and distribution of eggs in feces are irregular thus single fecal egg count assay may lead to in correct conclusion [27]. A Fasciola hepatica specific antibody is recognized using ELISA or Western blot since 2–4 weeks post- infection [39]. In vivo diagnosis of mild and prevalent infection is possible serologically. For example, detection of antibodies by ELISA in serum or milk is available and particularly useful for diagnosis of infection in sheep in an individual or herd basis. Arise in antibodies can be detected by two weeks after infection and keeps rises until week six [30]. The detection of adult flukes in the liver at necropsy is the most reliable method to confirm Fasciolosis. Prevalence studies should be based on abattoir survey other than coproscopic investigation [40]. Acute Fasciolosis which is common in sheep is manifested by severe anemia and sudden death. Confirmation is by post mortem examination when small fluke can be expressed from the liver parenchyma [13]. Whereas chronic Fasciolosis is confirmatory diagnosis could easily carried out by coproscopic examination employing sedimentation technique. Number of eggs in fecal sample is not an accurate indication of the number of the parasites neither in the liver nor of the amount of damage being done to the host [41]. Ultrasound can be used visualized the adult fluke in the bile duct and connecting tissue scan may reveal the burrow tract made by the worms and dilation of the bile duct [42].
Open Access Journal of Veterinary Science & Research
Treatment
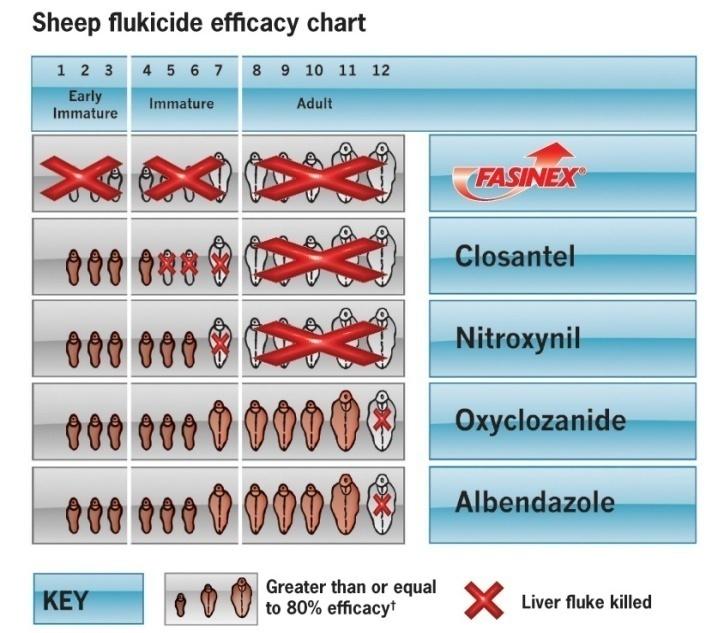
Not all compounds are equally effective against stages of development of F. hepatica in the body. For the treatment of acute Fasciolosis, it is essential to choose a product highly effective against the juveniles that damage the liver parenchyma. For chronic disease, a compound active against adult fluke is required [43]. Triclabendazole (Fasinex) is considered as the most common drug due to its high efficacy against adult as well juvenile flukes. It is effective against adult F. hepatica at a dose rate of 7.5 mg/kg in sheep. It is ovicidal and well kills any F. hepatica eggs present in the bile duct or the alimentary tract at the time of treatment. Clorsulon is supplied in combination with ivermectin for combined fluke and around warm control in cattle. Nitroxynil is given sub cutaneausly at 10 mg/kg and has good efficacy against the adult fluke but the dose has to be increase by up to 50% to obtain adequate control of acute disease [43].
Control and Prevention
Program charts for Fasciolosis control can be produced based on average rainfall and temperature records of any geographic regions [44]. Reduction of snail population before any scheme of snail control is under taken as a survey of the snail habitat should be made to determine whether they are localized or wide spread. When the snail habitat is limited simple method of control is to fence off these areas or treat annually with a molluscides. Currently cupper sulphate is most widely used and more efficient molluscides such as N- trityl morphine [45, 30]. Control of snail by chemical such as niclosamide, sodium pentachlorophenate, copper sulphate focally and seasonally possible, however, usually not practical due to labor, high cost, environmental consideration and rapid colonization of snail habitat [30]. It is true that seasonal strategic application of effective anthelmintics which is specific for trematode as well as timely prophylactic and curative treatment play an important role in the control of liver fluke infection [41]. The prophylactic used of anthelmintics aiming to reduce pasture contamination by fluke eggs at times most suitable for development of fluke, April to august and removing fluke population at times of heavy burdens or at periods nutritional stress to animal. Prophylactic treatment in sheep is therefore directed at reducing the fluke burdens in the winter at a time when the nutritional status of the animal is at its lowest level [30]. Other control methods include environmental sanitation and manipulation (draining, swamps, building sewage system and providing clean water supplies), rotational grazing and also avoiding mixed grazing of animals of different age groups (young animals are generally susceptible to helminthes infection [46]. Molluscicide is the most frequently used public health intervention is the application of molluscicides to decrease the population of Lymnaea snails, the intermediate hosts of Fasciola hepatica. Molluscicides have been particularly popular because they also decrease transmission of many other Trematode of importance, such as the various Schistosoma and Fasciola species [47]. Two methods for control of snail, they are biological and immunological methods. Biological control agents of snails have been studied and tested against the snail host, Free-ranging ducks or geese, which feed on snails, have also been proposed as a possible means for control of F. gigantic [48] Immunological method use of Glutathione S- transferase (GST) isolated from F. gigantic as a vaccine alone or in combination with either aluminum hydroxide or saponin in sheep against F. gigantica infection has also been evaluated. The highest fluke reduction was observed in the group vaccinated with GST-saponin (32 %), but the reduction was not statistically significant in comparison with the control group [49, 50].
Conclussion and Recommendation
In general, Fasciolosis is an important limiting factor for ovine production and causes several economic losses due to morbidity and mortality and also due to liver condemnation thereby contributing to loss hide and wool productivity of sheep industry in Ethiopia. The
Open Access Journal of Veterinary Science & Research
two species of the greatest veterinary importance are Fasciola hepatica and Fasciola gigantia and snails are their intermediate host with the recommendations of education of farmers, control rather than treatment, reduction in the number of snail by drainage, fencing, and use of molluscides. Strategic anthelmintics treatment with appropriate fluckicide drug should be practiced twice a year; before and after rainy seasons to eliminate fluke burden of the host of animal and minimize pasture contamination by fecal egg shedding thus interrupting the life cycle and cook water-grown vegetables thoroughly before eating. Disease of livestock have many additional direct and indirect impacts on human nutrition, community development and socio-cultural and also reduction in farm income, contributing to food insecurity and poor nutrition, therefore the control of the parasites based on the current finding the following points were Recommended; Control of intermediate host snails through drainage practicing zero grazing is important in the control of the disease. Improving of the veterinary service and infrastructure in prevalence area with provision of modern anthelmintic and treatment is giving based of the weight of the animal? Regular deworming of animals before and after the rainy season is important. Drainage of swampy area is also important in the reduction of the intermediate host. Applications of mulluscicide drugs are important in the control of the intermediate hot factors and its indirect economic loss.
Acknowledgement
- Above all, I would like to praise Almighty GOD, for his loving, supporting, and guiding me in all my life.
- Secondly, I would to acknowledge the Medwin Publisher site (Open Access Journal of Veterinary Science & Research) for they accept and help in preparing this review.
- Lastly, but not least, I would have great gratitude for ICT center of Jimma university college of veterinary medicine for they guide me by internet access
References
-
CSA (Central Statistical Agency) (2009) Agricultural survey. Report on livestock, poultry and bee hives population, private peasant holdings. Addis Ababa, Ethiopia pp: 2.
-
Alemayehu Z, Fletcher I (1995) Small ruminant productivity in the central Ethiopian mixed farming system. Institute of Agricultural Proceeding 4: 1941-1947.
-
Zelalem A, Fletcher I (1991) Small ruminant productivity in the central Ethiopian mixed farming systems. In: IAR, Addis Ababa, Ethiopia: 4 National Livestock Improvement Conference, 13-15 Novemberpp: 141-147.
-
Brook L, Fesha G, Shibiru T (1985) Studies on fascioliasis in four selected sites in Ethiopia. Vet Parasitol 18(1): 29-37.
-
Scott JM, Goll PH (1977) The epidemiology and anthelmintic control of ovine fascioliasis in the Ethiopian Highlands. Br Vet J 133(3): 273-280.
-
Tesfaheywet Z (2012) Helminthosis of Sheep and Goats in and around Haramaya, Southeastern Ethiopia. J. Anim. Hlth. Vet. Med 4(3): 48-55.
-
Yeneneh A, Kebede H, Fentahun T, Chanie M (2012) Prevalence of cattle Flukes infection at Andassa Livestock Research Center in north-west of Ethiopia Veterinary Research Forum 3(2): 85-89
-
Adem A (1994) Prevalence of Bovine and ovine fasciolosis a preliminary survey around zeiway region (Shewa Ethiopia) DVM Thesis Addis Ababa University, Faculty of veterinary Medicine, Debre Zeit Ethiopia pp: 1-15.
-
Ahmed EF, Markvichitr K, Tumwasorn S, Koonawootrittriron S, Choothesa A, et al. (2007) Prevalence of Fasciolaspp Infections of sheep in the Middle Awash River Basin, Ethiopia. Southeast Asian J Trop Med Public Health 38(1): 51-57.
-
Okewol EA, Ogundipe GAT, Adejinmi JO, Olaniyan AO (2000) Clinical evaluation of three Chemiophylatic Regines against ovine helminthosis in a Fasciola endemic area from in Ilbadan, Nigeria. Israel Journal of Veterinary Medecine 56(1): 15-28.
-
Wessie M (1995) Prevalence of bovine and ovine fasciolosis a preliminary survey in Nekemte and its surrounding areas, DVM Thesis, FVM, Addis Ababa University, Dedre Zeit, Ethiopia pp: 30
-
Urquhart GM, Amour JL, Duncan JL, Dunn AM, Jennings FW (2007) Veterinary Parasitology. 3rd (Edn.) Black Well Science, Hoboken 103-133.
-
Mas-Coma S, Bargues MD, Valero MA (2005) Fascioliasis and other plant-borne trematode Open Access Journal of Veterinary Science & Research zoonoses. International Journal of Parasitology 35(11-12): 1255-1278.
-
WHO (1995) Control of Food Borne Trematode Infections. Technical Report Series 849: 1-157.
-
World Health Organization (2009) Fascioliasis: Infection with the “Neglected” Neglected Worms.
-
Urquhart GM, Aremour J, Duncan JL, Dunn AM, Jennings FM (1996) Veterinary parasitology, 2edn. Blackwell Science, UK, pp: 102-120.
-
Valero MA, Darce NA, Panova M, Mas-Coma S (2001) Relationships between host species and morphometric patterns in Fasciola hepatica adults and eggs from the northern Bolivian Altiplano hyperendemic region. Veterinary Parasitology 102(1-2): 85-100.
-
Urquhart GM, Armour JD, Duncan JL, Dunn AM, Jennings FW (1989) Veterinary parasitology. 2nd Edition, Blackwell, 286.
-
Maximou UI (1982) A Series of Practical Studies of the Helminthes, Arthropods and Protozoa of Domestic Animals Use during Practical Classes in Parasitology. Veterinary Institute, DebreZeite.
-
Soulby JL (1982) Helminthes, Arthropods and Protozoa of Domestic Animals. 7th (Edn.), Ballier Tindal, London, 40-52.
-
Monica C (1987) District Laboratory Practice in Tropical Countries. 223-234.
-
Tamura K, Peterson D, Peterson N, Stecher G, Nei M, et al. (2011) “MEGA5: molecular evolutionary genetics analysis using maximum likelihood, evolutionary distance, and maximum parsimony methods,” Molecular Biology and Evolution 28 (10): 2731-2739.
-
Peng M, Ichinomiya M, Ohtori M, Ichikawa M, Shibahara T, et al. (2009) Molecular characterization of Fasciola hepatica, Fasciola gigantica, and aspermic Fasciola sp. in China based on nuclear and mitochondrial DNA. Parasitology Research 105(3): 809-815.
-
Hall MTB (1986) Disease and parasites of livestock in the tropics. 2ndIntermediate Tropical Agriculture Series. London: Longman 207.
-
Soulsby EJL (1982) Helminth, Arthropod and Protozoa of Domestic Animals. 7th (Edn.), Baillere Tindall, London, Uk, Pp: 809.
-
Malone JB, Gommes R, Hansen J, Yilma JM, Slingenberg J, et al. (1998) A geographic information system on the potential distribution and abundance of Fasciola hepatica and F. gigantic in east Africa based on Food and Agriculture Organization databases. Vet Parasitol 78: 87-101.
-
Maqbool A, Hayat CS, Tanveer A, Hashmi HA (2002) Epidemiology of Fasciolosis in Buffaloes under Different Management Conditions. Veterinarski Arhiv 72: 221-228.
-
Dalton JP, Spithil TW (1998) Progress in Development of Liver Fluke Vaccines. Parasitology Today 14: 224-228.
-
Radostits OM, Gay CC, Hinchclitt KW, Constable PD (2007) Veterinary Medicine, a Text Book of the Disease of Cattle, Horses, Sheep, Goats, and Pigs. 10th (Edn.), Elsevier, New York 1516-1579.
-
Terefe D, Wondimu A, Gachen DF (2012) Prevalence, gross pathological lesions and economic losses of bovine Fasciolosis at Jimma Municipal Abattoir, Ethiopia. Journal of Veterinary Medicine and Animal Health 4(1): 6-11.
-
Marquardt WC, Demaree RS, Grieve RB (2000) Parasitology and Vector Biology. 2nd Edition, Harcoart Academic Press, London, 273-279.
-
Scott JM, Goll PH (1997) The Epidemiology and Anthelmintic Control of Ovine Fasciolosis in Ethiopian Central Highlands. British Veterinary Journal 133: 273-280.
-
Richter J, Fraise S, Mull R, Millan JC (1999) Fasciolosis: son graphic abnormalities of the bilary tract and evolution after treatment with Triclabendazole. Tropical Medicine of International Heath 4 (11): 774-781.
-
Behm CA, Sangster NC (1999) Pathology, pathophysiology and clinical aspects. In: Dalton JP (Ed), Fasciolosis. CAB International Publishing, Wallingford 185-224.
-
Urquhart GM, Armour J, Duncan JL, Dunn AM, Jennings FW (1994) Veterinary parasitology. Oxford: Longman Scientific 98-109.
-
Michael A (2004) Infectious Prevalence of Ovine Fasciolosis in Irrigation Schemes along The Upper Awash River Basin and Effect of Strategic Anthelmintic Treatment in Selected up Stream Areas. M.Sc. Thesis, Department of Biology, School of Graduate Studies, Addis Ababa University, Addis Ababa. Open Access Journal of Veterinary Science & Research
-
Urquhart GM, Amour J, Duncan JL, Dunn AM, Jennings FW (1996) Veterinary Parasitology 2nd Edn, Oxford, Longman Scientific and Technical Press, UK. Pp: 100-109
-
Mitchell GBB (2003) Treatment and Control of liver fluke in sheep and cattle. Technical notes November, Sac 2003. West mains roads, Edinburgh.
-
Taylor MA, Cop RL, Wall RK (2007) Veterinary Parasitology. 3rd (Edn.), Blackwell Publishing, Oxford, 81.
-
Zimmerman GL, Jen LW, Cerro JE, Farnsworth KL, Wescott RB (1982) Diagnosis of Fasciola hepatica infection in sheep by immunosorbent Assay Amer J Vet Res 43(12): 2079-2100.
-
Kaufman J (1996) Parasitic Infection of Domestic Animals, a Diagnostic Manual. Verlag, Berlin 90-92.
-
Wakuma M (2009) Prevalence and Economic Significance of Bovine Fasciolosis at Bedele Municipal Abattoir. PhD Thesis, Faculty of Veterinary Medicine, Jimma University, Jimma.
-
Hansen J, perry B (1994) The Epidemiology, Diagnosis, and Control of Helminth Parasites of Ruminants. 4th (Edn.), International Laboratory for Research on Animal Diseases, Nairobi, 74.
-
Rai RB, Sinai S, Ahlawat SPS, Kumar BV (1996) Studies on the control of fasciolosis in Andaman and Nicobar Islands. Indian Veterinary Journal 73: 822 825.
-
Cornelissen BW, Gasenbeek PV, Borgsteede WG, Harnisen MM, Boerrsma WT (2000) Early Immune Diagnosis of Fasciolosis in Ruminants Using Recombinant _Fasciola hepatica_ Cathepsin-Like Protease. International Journal for Parasitology 31(7): 728-737.
-
Kassai T (1999) Veterinary Helmintology. Butler Worth Heinemann, Oxford, 9.
-
Mas-Coma S, Valero MA, Bargues MD (2014) Chapter 4: fascioliasis. In: Toledo R, Fried B, editors. Digenetic Trematodes. New York: Advances in Experimental Medicine and Biology Series, Springer Science + Business Media, 766: 77-114.
-
Malek Emile A (1980) Snail-Transmitted Parasitic Disease.
-
Pfukeny DM, Mukartirwa S, Willingham AL, Monrady (2006) Epidemiological studies of Fasciola gigantica infections in cattle in the high veld and low veld communal grazing areas of Zimbabwe. Journal of Veterinary Research 73: 37-51.
-
Parr SL, Gary JS (2000) A Strategic Dosing Scheme for the Control of Fasciolosis in Ireland. Veterinary Parasitology 88(3-4): 187-197.
- The Digital Stethoscope: Harnessing AI in Veterinary Medicine Without Losing Our Healing Touch
- Meningoencephalomyelitis of Unknown Etiology: Short-Term Effect of Two Treatment Protocols on Cerebrospinal Fluid
- Safety and Efficacy of the HomeoPet Cough in Domestic Pets –A Clinical and Correction Analysis Based Upon User Response Survey
- Non Human Animals Responses to Social Loss
- Owner Reported Clinical Outcomes of a Homeopathic Proprietary Preparation for the Treatment of Upper Respiratory and Nasal Disorders in Companion Animals
- Effects and Diagnostic Approach of Ultrasound in Veterinary Practice: A Systematic Review