Comparison of the Tibial Anatomical-Mechanical Axis Angle and Patellar Positions between Labrador Retrievers and Golden Retrievers with and without Cranial Cruciate Ligament Rupture
This study investigated proximodistal and craniocaudal patellar positions and assessed these positions with the tibial anatomical-mechanical axis angle (AMA-angle), tibial plateau angle (TPA), relative tibial tuberosity width (rTTW), and Z-angle in Labrador Retrievers (LR) and Golden Retrievers (GR) with and without cranial cruciate ligament rupture (CCLR). Mediolateral radiographs were obtained from 2 groups. The affected group had a normal contralateral stifle measured at the time of unilateral surgically confirmed CCLR, which developed a subsequent contralateral CCLR (SC-CCLR; 40 dogs), and the control group (60 dogs aged >11 years) had normal stifles. In the SC-CCLR group, 95% of the tibial anatomical axes (AAs) were cranial (CR) to the patella, with a median (range) AMA-angle of 2.92° (1.65°-4.92°), while in the control group, 93% of the stifles had AAs caudal (CA) to or in the middle (M) of the patella, with a median (range) AMA-angle of 1.03° (0°-3.52°). The craniocaudal position of the patella was correlated statistically with the AMA-angles (median (range), 0.86° (0-1.61°), 1.87° (1.22-2.7°), and 2.97° (1.72-4.92°) in the CA, M, and CR positions, respectively, but not with other tibial measurements (p
Introduction
Cranial cruciate ligament rupture (CCLR) is a major cause of disability in the stifle joints of dogs and is reportedly caused by abnormal biological and biomechanical components leading to the development of progressive osteoarthritis (OA) and ‘organ joint failure’ [1, 2, 3, 4]. Concerning the biomechanics, most CCLRs are believed to be secondary to repetitive microtrauma and chronic strain that weakens the CCL and appears to result in the overuse and fatigue failure of the CCL [2, 3, 4, 5]. The altered biomechanics involved in the pathogenesis of the deficient-stifle joint could be secondary to conformational abnormalities in the proximal tibia or distal femur [6, 7, 8, 9, 10, 11]. Although several variations in stifle morphology can result in significant microinjury to the CCL, these variables have not been recognized as strong predictive factors of CCLR [12, 13, 14, 15, 16, 17, 18].
A recent study comparing dogs at low risk of developing CCLR and a consecutive series of predisposed dogs with surgically confirmed CCLR showed a caudal shift in the tibial weightbearing mechanical axis (MA) from the tibial anatomical axis (AA), which was quantified by the magnitude of the angle between these two axes (AMA-angle); thus, the AMA-angle may be a clinically relevant predisposing factor for the development of CCLR [10]. In this study, an AMA-angle higher than 1.9° had a sensitivity of 0.94 and a specificity of 0.97 in predicting CCLR in dogs [10]. This caudal shift of the functional axis, which is a reflection of the caudal angulation of the entire tibia (10), could alter the relationship between the patella and the anatomic structures of the stifle and, therefore, could affect the patellofemoral joint (PF) biomechanics. In two recent studies, OA of the PF has been identified to occur in all stifle joints in dogs with naturally occurring CCL-insufficiency, even in stable stifles with partial CCL tears [19, 20]. This finding could suggest that cartilage damage in the PF could be consecutive to alterations in the mechanical loading of PF and not subsequent to CCLR as previously speculated [19]. Limited information is available regarding the potential clinical conditions associated with the proximodistal and craniocaudal positions of the patella in CCL-deficient dogs because assessing patella positions is negatively impacted by the secondary caudal subluxation of the femur relative to the tibia [21, 22, 23].
The proximodistal patellar position has been previously assessed by using the Insall-Salvati index (ISI), the modified Insall-Salvati index (mISI) and the Caton-Deschamps index (CDI) [23, 24, 25, 26, 27]. The recognized drawbacks of these indices include inaccuracy when used in practice when anatomic landmarks are modified by OA [22, 26, 27]. To assess the proximodistal patellar position even in the presence of OA, a similar index to the CDI has been used, i.e., the Guenego- Verwaerde index (GVI), with intraarticular tibial bony landmarks that are less altered by osteophytosis [28].
The aim of the present study was to compare the proximodistal and craniocaudal positions of the patella between a group of stifles not showing clinical or radiographic signs, measured at the time of an unilateral CCLR (U-CCLR) that developed a subsequent contralateral CCLR (SC-CCLR) during the study, and a control group of healthy normal stifles of Labrador retrievers (LR) and Golden retrievers (GR) >11 years of age. The study herein assesses the possible relationship between these positions and tibial measurements, such as the TPA [29, 30], Z-angle [10, 31, 32, 33], Rttw [6, 10, 31, 32, 33, 34], and AMA-angle [10]. We hypothesized that if the craniocaudal angulation of the proximal tibia could influence the development of CCLR, the AMA-angle and the craniocaudal position of the patella could differ between stifle joints that developed SC-CCLR and healthy stifle joints.
Materials and Methods
Inclusion Criteria
This prospective study was performed at our referral centre from January 2012 to December 2017. The CCLR- affected dogs included in this study were LR and GR; all dogs underwent a clinical examination, and the mediolateral radiographic views of both tibiae were obtained under general anaesthesia before surgery.
The experimental group consisted of the contralateral healthy stifle, radiographed and measured at the time that the U-CCLR was surgically confirmed (at the clinic) as SC- CCLR (group SC-CCLR) and censored at a minimum of 3 years of follow-up from the initial diagnosis as proposed by Fuller, et al. [18]; no evidence of any other concurrent stifle pathology was observed during the physical and radiographic examinations.
The control group included LR and GR that were anesthetized for medical reasons unrelated to this study. During this anaesthesia, all owners agreed to have their animal radiographed at no cost and provided written informed consent.
To be included in the study, dogs of the control group were older than the oldest CCLR-deficient dog in the study (>11 years) with no history or clinical signs of stifle joint disease, and their physical, orthopaedic and radiographic examinations of the stifle joints revealed no abnormalities. All medical data of the dogs are shown in Table 1.
| Median: min-max | Control group | SC-CCLR group |
|---|---|---|
| Number of dogs | 60 | 40 |
| Age (years) | 11.8 (11.1 – 16) | 5.05 (1.2 – 9.6) * |
| Weight (kg) | 37 (27 – 57) | 34 (27 – 46) |
| Gender (M/F) | 31/29 | 28-Dec |
| Breed and number of dogs included in the groups (number of tibiae measured) | ||
| Labrador Retriever (LR) | 32 (64) | 28 (28) |
| Golden Retriever (GR) | 28 (56) | 12 (12) |
Table 1: Studied population characteristics. *p<0.05 using a Mann-Whitney non-parametric comparison SC-CCLR: subsequent contralat
Radiographic Procedure
Mediolateral radiographs of the stifle were obtained until the flexion angle of the stifle were at 90° using the method described by Mostafa et al. [22]. Briefly, the angle of the stifle joint was defined as the angle formed between the long axis of the distal femur and the proximal aspect of the tibia (Figure 1A and C) [22]. The anatomic landmarks described to obtain the stifle joint angle at 90° without the use of the talus and proximal femur have been used as references for ex vivo biomechanical studies and recently for screening dogs for CCLR in clinical studies [7, 9, 11, 22]. Then, once the flexion angle was equal to 90°, the radiographs were digitally duplicated, and lines drawn to determine the long axis of the distal femur and proximal aspect of the tibia were retrieved. On this duplicated radiograph, the tibial measurements and reference lines used to determine the proximodistal patellar position were drawn (Figures 1B and 2D). The radiographs were stored digitally as DICOM files.
![Figure 1: Measurements of the stifle joint angle at 90° (A and C) and AMA-angle with the craniocaudal position of the patella relative to the AA (B and D) on mediolateral radiographs of a contralateral healthy stifle of a LR at the time of a U-CCLR (A and B), and of a healthy old LR (C and D). PTW, proximal tibial width; DTW, distal tibial width; A, cranial extent of the medial tibial plateau; B, midpoint of the DTW; AB = 2X PTW; FCL, femoral condylar length; X, proximal extend of the femoral trochlea; FW, femoral width, which is measured at the distance equal to the FCL; D, segment parallel and proximal to the FW at 20 mm from the FW; Stifle joint angle is the angle formed between the long axis of the distal femur (line connecting the midpoints of FW and D) and the long axis of the proximal tibia (line connecting A and B), according to Mostafa, et al. [22]; AA, anatomical axis; MA, mechanical axis; AMA-angle, angle between AA and MA according to Guénégo, et al. [10].](/fulltextimages/6042/fig_1.jpeg)
Figure 1: Measurements of the stifle joint angle at 90° (A and C) and AMA-angle with the craniocaudal position of the patella relative to the AA (B and D) on mediolateral radiographs of a contralateral healthy stifle of a LR at the time of a U-CCLR (A and B), and of a healthy old LR (C and D). PTW, proximal tibial width; DTW, distal tibial width; A, cranial extent of the medial tibial plateau; B, midpoint of the DTW; AB = 2X PTW; FCL, femoral condylar length; X, proximal extend of the femoral trochlea; FW, femoral width, which is measured at the distance equal to the FCL; D, segment parallel and proximal to the FW at 20 mm from the FW; Stifle joint angle is the angle formed between the long axis of the distal femur (line connecting the midpoints of FW and D) and the long axis of the proximal tibia (line connecting A and B), according to Mostafa, et al. [22]; AA, anatomical axis; MA, mechanical axis; AMA-angle, angle between AA and MA according to Guénégo, et al. [10].
Radiographic Measurements of the Tibia
The AMA-angle was determined as the angle formed by the tibial AA and the tibial MA as previously defined (Figure 1B and D) [10]. The TPA was measured using landmarks as previously described [29, 30, 35, 36]. The Z-angle and rTTW were measured as previously reported [6, 10, 31, 32, 33, 34].
Evaluation of the Patellar Position
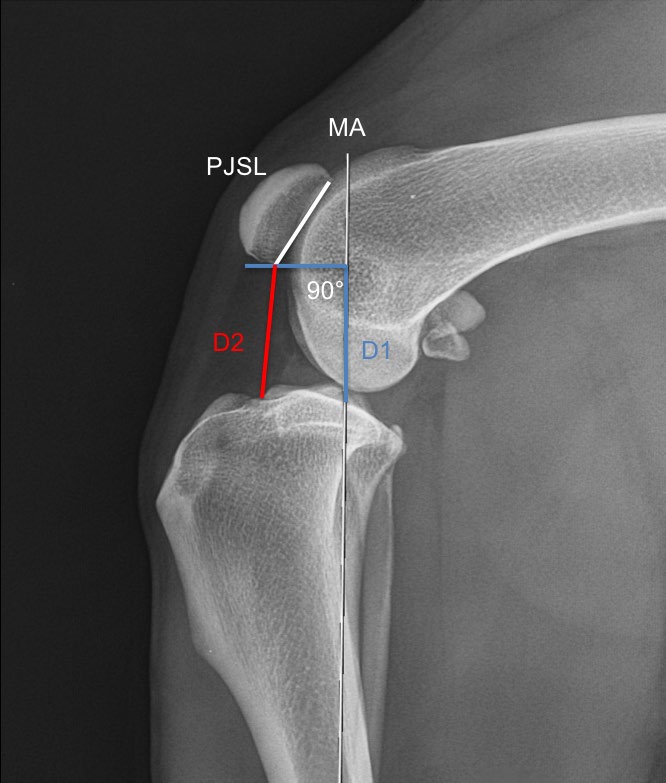
The vertical patellar position was assessed using the Insall-Salvati (ISI), modified Insall-Salvati (mISI), Caton- Deschamps (CDI), and Guénégo-Verwaerde (GVI) indices. The ISI is obtained by dividing the patellar ligament length (PLL) by the greatest diagonal length of the patella (PL), as previously described by Mostafa, et al. [22]. The mISI is the ratio between the PLL and the patellar joint surface length (PJSL), as defined by Miles, et al. [23]. The CDI is defined as the ratio of the length of the distance between the distal points of the patellar articular surface to the closest tibial cortex (D1) divided by the PJSL (Figure 2) [23, 25].
The GVI is determined by the ratio of the distance from the point intersecting the tibial plateau (TP) and the MA of the tibia and a point at the intersection between a line drawn perpendicular to the MA to the distal point of the patellar articular surface (D2) and the PJSL [28] (Figure 2).
The craniocaudal position of the patella was defined by the position of the AA relative to the patella. The patella was divided into five equal parts on its greatest diagonal length. The middle of the patella was defined by the part (1/5 of the length of the patella) centred strictly in the middle. The AA was recorded as caudal (CA) if the AA was caudal to the middle part of the patella (Figure 1D), middle (M) if the AA crossed the middle of the patella and cranial (CR) if the AA was cranial to the middle part of the patella (Figure 1B). To measure the intra- and inter-observer variability, any identifying information was removed from the digital radiographs, and three observers blindly evaluated two distinct series of measurements concerning the patella positions on a randomized sample of 30 radiographs of the studied groups [10, 36, 37]. The intra-and inter-observer variability of the AMA-angle, TPA, rTTW and Z-angle have been recorded in a previous study [10]. The measurements were repeated at least 14 days after the initial evaluation.
PJSL, patella joint surface length; D1, measurements of the length of the distance between the distal point of the PJSL to the closest tibial cortex, according to Miles, et al. [23]. The measurements are used to calculate the Caton-Deschamps Index (CDI=D1/PJSL). D2, measurements of the length of the distance from the point intersecting the tibial plateau and the mechanical axis (MA) of the tibia (and a point at the intersection between a line drawn perpendicular to the MA to the distal point of the PJSL). The measurements are used to determine the Guénégo-Verwaerde Index (GVI=D2/PJSL) [28].
Statistical Analysis
Normality was determined by the Shapiro-Wilk test. In cases in which a normal distribution was not identified in the data, the results are reported as the median and range with interquartile distance [Q1 – Q3]. The statistical analysis was performed using a non-parametric approach. All statistical analyses were performed on one limb within each dog of the control group but verified for both sides to accommodate the lack of independent samples. The statistical comparisons of the tibial measurements were performed using bilateral Mann-Whitney rank tests. Kruskal-Wallis tests and Dunn’s test followed by a post hoc test with Bonferroni adjustment were performed for the multiple comparisons of the tibial measurements and patellar positions. Spearman’s rank correlation coefficients were used to estimate the correlations between the tibial measurements. To examine the inter- and intra-observer variability, Kendall’s Coefficient of Concordance (KCC) among and within the observers were calculated for the PLL, PL, D1 and D2 measurements. A receiver operating characteristic (ROC) analysis was conducted to define the threshold values for the tibial measurements that could predict CCLR in dogs.
All statistical analyses were performed using XLSTAT software (Addinsoft). Statistical significance was considered at a p-value<0.05.
Results
Eighty-four dogs were enrolled in the U-CCLR group, and 60 dogs were enrolled in the control group. In the U-CCLR group, 40 dogs were observed to have an SC-CCLR and were enrolled in the experimental group. The breed, weight, gender and age of the dogs in the two groups are reported in Table 1.
The radiographic measurements of the AMA-angle, TPA, rTTW, Z-angle, PLL, PL, PJSL, D1, D2, ISI, mISI, CDI, and GVI and the craniocaudal patellar positions in the control group and the SC-CCLR group are reported in Table 2.
| Measurements | Control group | SC-CCLR group | |
|---|---|---|---|
| Number of dogs (Number of tibiae and patellar positions measured) | 60 (60) | 40 (40) | |
| AMA angle (°) [0.75 – 1.63] | 1 (0 – 3.52) | 2.92 (1.65 – 4.92)* | |
| [2.66 – 3.24] | |||
| TPA (°) [24 – 27.9] | 26 (20.1 – 30.9) | 28 (22.5 – 35) | |
| [27.5 – 30.2] | |||
| rTTW [0.61 – 0.7] | 0.65 (0.57 -0.86) | 0.71 (0.57 – 0.86) | |
| [0.69 – 0.75] | |||
| Z-angle (°) [60 – 64] | 61.7 (52.2 – 68.5) | 65.5 (50.3 – 76.2) | |
| [62.2 – 69] | |||
| PLL (mm) [46.2 – 52.5] | 49.5 (42.2 – 66.1) | 49 (42.2 – 57.1) | |
| [47.1 – 51.9] | |||
| PL (mm) [20.1 – 22.4] | 21.3 (19.4 – 23.6) | 21.5 (19.4 – 23.6) | |
| [20.5 – 22.4] | |||
| ISI=PLL:PL [2.27 – 2.41] | 2.32 (2 – 2.6) | 2.3 (2.1 – 2.57) | |
| [2.27 – 2.33] | |||
| PJSL (mm) [17.5 – 19.1] | 18.3 (15 – 24.4) | 18.1 (16.6 – 20) | |
| [17.4 – 18.8] | |||
| mISI=PLL:PJSL [2.59 – 2.8] | 2.7 (2.27 – 3.19) | 2.72 (2.5– 3.05) | |
| [2.63 – 2.8] | |||
| D1 (mm) [25 – 28.5] | 26.6 (20.6 – 37.5) | 27.5 (24.2 – 37.1) | |
| [25.8 – 29] | |||
| CDI=D1:PJSL [1.4 – 1.53] | 1.46 (1.23 – 1.79) | 1.53 (1.3 – 1.94) | |
| [1.49 – 1.58] | |||
| D2 (mm) [25.2 – 28.8] | 26.8 (20.7 – 37.6) | 28 (24.3 – 37.8) | |
| [26 – 29] | |||
| GVI=D2:PJSL [1.41 – 1.53] | 1.47 (1.25 – 1.87) | 1.54 (1.29 – 1.9) | |
| [1.5 – 1.59] | |||
| Position of the patella/AA (number of stifles, %) | F (front) | 84 – 70% | 0 – 0% |
| M (middle) | 28 – 24% | 2 – 5% | |
| B (back) | 8 – 6% | 38 – 95% |
Table 2: Values of the radiographic tibial measurements and proximodistal and craniocaudal patellar positions relative to the ana
Table 2: Values of the radiographic tibial measurements and proximodistal and craniocaudal patellar positions relative to the anatomical axis (AA). All measurements were performed by the same observer (observer 1). The data are expressed as the medians (min – max) and interquartile distance [Q1 – Q3]. AMA angle: anatomical-mechanical axis angle; TPA: tibial plateau angle; Z-angle: angle between the mechanical axis of the tibia and a line joining the tibial tuberosity and the intercondylar eminence; rTTW: relative tibial tuberosity width; PLL: patellar ligament length; PL: patella length; ISI=PLL:PL: Insall-Salvati index; D1: length of the distance between the distal point of the patellar articular surface and the closest tibial cortex; CDI=D1:PJSL: Caton-Deschamps index; D2: distance from the point intersecting the tibial plateau (TP) and the mechanical axis (MA) of the tibia and a point at the intersection between a line drawn perpendicular to the MA to the distal point on the patellar articular surface; GVI=D2:PJSL: Guénégo-Verwaerde index. *p-values were determined using a Mann-Whitney non-parametric comparison.
The KCCs are shown in Table 3 and indicated a good-to- strong correlation in the values of all parameters of interest measured by the distinct observers and the same observer. We found no differences between the groups in all parameters tested, except for the AMA-angle (p<0.0001). The AMA-angle values significantly differed in all groups concerning the craniocaudal position of the AA relative to the patella median (range) AMA-angle as follows: 0.86° (0°-1.61°), 1.83° (1.22°- 2.27°), and 2.97° (1.72°-4.92°) in the CA, M, and CR positions, respectively (p<0.0001). In the control group, 93% of the stifles had an AA caudal or in the middle of the patella with a median (range) AMA-angle of 1.03° (0°-3.52°), while in the SC-CCLR group, 95% of the AA were cranial to the patella with a median (range) AMA-angle of 2.92° (1.65°-4.92°). All the dogs with an AMA-angle above 3° had an AA cranial to the patella. The CDI and GVI were strongly correlated in the control group (r=0.961; p<0.0001).
| Intra-observer variability | Inter-observer variability | ||||
|---|---|---|---|---|---|
| Median (min – max) PLL | Obs 1 | Obs 2 | Obs 3 | ||
| Obs 1 | 48.65 (42.5-57.1) | 0.876 | - | 0.720 | 0.822 |
| Obs 2 | 48.2 (41.2-57.6) | 0.889 | - | 0.783 | |
| Obs 3 | 48.05 (41.4-57.4) | 0.937 | - | ||
| Median (min – max) PL | |||||
| Obs 1 | 21.05 (19.1-23.8) | 0.667 | - | 0.478 | 0,659 |
| Obs 2 | 22.45 (19.4-25.8 | 0.875 | - | 0,625 | |
| Obs 3 | 21.3 (19-24.7) | 0.864 | - | ||
| Median (min – max) PJSL | |||||
| Obs 1 | 17.7 (16.3-20.5 | 0.776 | - | 0.511 | 0.535 |
| Obs 2 | 17.8 (15.6-20.3) | 0.765 | - | 0.625 | |
| Obs 3 | 17.65 (15.8-20.6) | 0.775 | - | ||
| Median (min – max) D1 | |||||
| Obs 1 | 27.2 (22.7-37.1) | 0.894 | - | 0.781 | 0.766 |
| Obs 2 | 27.1 (23.1-35.6) | 0.901 | - | 0.733 | |
| Obs 3 | 27.5 (23.1-35.8) | 0.900 | |||
| Median (min – max) D2 | |||||
| Obs 1 | 27.35 (24-38.3) | 0.924 | 0.756 | 0.736 | |
| Obs 2 | 26.95 (34.2-35.9) | 0.842 | 0.705 | ||
| Obs 3 | 27.95 (7.4-39.2) | 0.789 | - |
Table 3: Intra- and inter-observer variability in the measurements of the PLL, PL, PJSL, D1, and D2. Kendall’s Coefficient of Con
In this study, the ROC curve analysis showed that an AMA-angle value equal to or higher than 2.42° was predictive of CCLR with a sensitivity of 0.95 (95% confidence interval [CI]: 0.83 – 0.99) and a specificity of 0.95 (95% CI: 0.89 – 0.98). In contrast, a TPA value equal to or higher than 27.5° was predictive of CCLR, with a sensitivity of 0.77 (95% CI: 0.62 – 0.88) and a specificity of 0.71 (95% CI: 0.62 – 0.78); a rTTW value equal to or less than 0.69 was predictive of CCLR, with a sensitivity of 0.8 (95% CI: 0.65 – 0.9) and a specificity of 0.66 (95% CI: 0.58 – 0.74); and a Z-angle equal to or higher than 67° was predictive of CCLR, with a sensitivity of 0.47 (95% CI: 0.33 – 0.62) and a specificity of 0.96 (95% CI: 0.91 – 0.98).
Based on these results, the AMA-angle and craniocaudal patellar position relative to the AA appear to be significantly more accurate parameters than the TPA, Z-angle, rTTW, ISI, mISI, CDI, and GVI to predict CCLR in dogs (p<0.0001).
Discussion
Our study supports the hypothesis that the AMA-angle and the craniocaudal position of the patella differ between stifle joints of a population of two breeds of dogs affected by CCLR that developed SC-CCLR and healthy stifle joints of a population of the same breeds of dogs, suggesting that the craniocaudal angulation of the tibia could influence the development of CCLR. Although the proximodistal position of the patella has been found to have a potential clinical influence on patella luxation [21, 22], the present study shows that the proximodistal position of the patella as measured by the ISI, mISI, CDI and GVI has no influence on the incidence of the occurrence of CCLR. However, the data obtained in the present study indicated that the craniocaudal position of the AA relative to the patella differs between groups, with the AA caudal to the patella in the control group and cranial to the patella in SC-CCLR group.
The CDI has been reported to be an accurate index in human patients and dogs in the assessment of the patellar height as the CDI reflects the distance between the distal pole of the patella and the tibial plateau (TP), whereas the ISI and mISI reflect the length of the patellar tendon and the patellar length [23, 24, 25, 26, 27]. However, the CDI is difficult to use in CCL- deficient stifles with osteophytosis on the cranial aspect of the tibia [23] as observed in all dogs with CCLR in our study. To palliate this potential issue, a similar index to the CDI, i.e., the GVI, was assessed by using the intraarticular bony landmark as the point of the intersection between the tibial plateau and the MA, which is less affected by OA [28]. Three observers were used to assess the intra- and inter-observer variability, as reported in previous studies [10, 33, 37]. In the current report, good inter- and intra-observer accordance was observed in the measurements of the PLL, PL, PJSL, D1 and D2 among all three observers, confirming the referenced findings.
The data obtained indicated a strong correlation between the CDI and GVI in the control group, confirming that the GVI assesses a similar patellar height in normal stifles. Furthermore, in this study, low inter- and intra- observer variability in the measurements of the patellar joint surface length and the distance from the distal pole of the patella to the TP were recorded. These levels of inter- and intra-variation indicate that these landmarks are acceptable for clinical use to assess the patellar height, even in the presence of OA. In the present study, a receiver operating curve (ROC) analysis was used to assess the discriminating properties of the tibial measurements and patellar positions studied; this analysis shows that the sensitivity and specificity of an AMA-angle higher than 2.42° in predicting the development of CCLR reached 95% and 95%, respectively, suggesting that this angle could be implemented with a previously published scoring system proposed by Cunningham, et al. [11] in a large-scale screening programme but warrants further investigations as a prerequisite before its use. The craniocaudal patellar position was strongly associated with the AMA-angle but not with other tibial measurements.
Although it remains to be determined how the magnitude of the AMA-angle and the consecutive craniocaudal position of the patella may play a role in the initiation or progression of CCL disease, considering these specific tibial measurements may help us decide which of all existing TPS alteration procedures could be the best surgical procedure on a case- by-case basis for each patient.
Recently, a CORA-based levelling osteotomy (CBLO), which is a curvilinear TPS alteration procedure in which the osteotomy is centred at the centre of the rotation of angulation (CORA) resulting in the desired post-operative TPA through the alignment of the proximal and distal anatomic axes, has been described [38]. Similarly, cranial closing wedge osteotomy based on the AMA-angle (AMA- based-CCWO) have been recently documented [28, 39] and revealed to accurately place the wedge by planning the precise alignment of the AA with the MA during the TPS alteration osteotomy. Similar to the CBLO, the AMA-based- CCWO through the alignment of these two axes during the TPA change is thought to limit the secondary translation of the tibia and caudal tibial thrust during weight bearing [38, 39]. Furthermore, with a post-operative reduced AMA- angle, the AA shifts from a cranial position relative to the patella to a caudal position, which is more consistent with unaffected stifles based on our data [28, 39].
Conclusion
The findings of the current study support the hypothesis that the AMA-angle and craniocaudal position of the patella differ between CCL-deficient stifles in LR and GR and stifles in normal healthy old LR and GR. This finding suggests that the craniocaudal angulation of the proximal tibia could influence the development of CCLR and deserves consideration in further studies.
References
-
Kim S, Acvs A, Kowaleski M, Lewis D (2008) Tibial osteotomies for cranial cruciate ligament insufficiency in dogs. Vet Surg 37(2): 111-125.
-
Cook JL (2010) Cranial cruciate ligament disease in dogs: biology versus biomechanics. Vet Surg 39(3): 270-277.
-
Griffon D (2010) A review of the pathogenesis of canine cranial cruciate ligament disease as a basis for future preventive strategies. Vet Surg 39(4): 399-409.
-
Comerford E, Smith K, Hayashi K (2011) Update on the aetiopathogenesis of canine cranial cruciate ligament disease. Vet Comp Orthop Traumatol 24(2): 91-98.
-
Hayashi K, Frank JD, Dubinsky C, Hao Z, Markel MD, et al. (2003) Histologic changes in ruptured canine cranial cruciate ligament. Vet Surg 32(3): 269-277.
-
Inauen N, Koch D, Bass M, Hässig M (2009) Tibial tuberosity conformation as a risk factor for cranial cruciate ligament rupture in the dog. Vet Comp Orthop Traumatol 22(1): 16-20.
-
Mostafa A, Griffon D, Thomas M, Constable P (2009) Morphometric characteristics of the pelvic limb of Labrador Retrievers with and without cranial cruciate ligament deficiency. Am J Vet Res 70(4): 498-507.
-
Osmond C, Marcellin-Little D, Harrysson O, Kidd L (2006) Morphometric assessment of the proximal portion of the tibia in dogs with and without cranial cruciate ligament rupture. Vet Radiol Uultrasound 47(2): 136-141.
-
Guerrero TG, Geyer H, Hassig M, Montavon PM (2007) Effect of conformation of the distal portion of the femur and proximal portion of the tibia on the pathogenesis of cranial cruciate ligament disease in dogs. Am J Vet Res 68(12): 1332-1337.
-
Guénégo L, Payot M, Charru P, Verwaerde P (2017) Comparison of tibial anatomical-mechanical axis angle between predisposed dogs and dogs at low risk for cranial cruciate ligament rupture. Vet J 225: 35-41.
-
Cunningham D, Ayman M, Gordan-Evans W, Boudrieau R, Griffon D (2017) Factors contributing to the variability of a predictive score for cranial cruciate ligament deficiency in Labrador Retrievers. BMC Vet Res 13: 235-241.
-
Duval JM, Budsberg SC, Flo GL, Sammarco JL (1999) Breed, sex, and body weight as risk factors for rupture of the cranial cruciate ligament in young dogs. J Am Vet Med Assoc 215(6): 811-814.
-
Morris E, Lipowitz AJ (2001) Comparison of tibial plateau angles in dogs with and without cranial cruciate ligament injuries. J Am Vet Med Assoc 218(3): 363-366.
-
Warzee CC, Dejardin LM, Arnoczky SP, Perry RL (2001) Effect of tibial plateau leveling on cranial and caudal tibial thrusts in canine cranial cruciate–deficient stifles: an in vitro experimental study. Vet Surg 30(3): 278-286.
-
Wilke V, Conzemius M, Besancon M, Evans R, Ritter M (2002) Comparison of tibial plateau angle between clinically normal Greyhounds and Labrador Retrievers with and without rupture of the cranial cruciate ligament. J Am Vet Med Assoc 221(10): 1426-1429.
-
Reif U, Probst C (2003) Comparison of tibial plateau angles in normal and cranial cruciate deficient stifles of labrador retrievers. Vet Surg 32(4): 385-389.
-
Venzin C, Howard J, Rytz U, Spreng D, Schawalder P, et al. (2004) Tibial plateau angles with and without cranial cruciate ligament rupture - comparison between different dog populations and a wolf population. Vet Comp Orthop Traumatol 17(4): 232-236.
-
Fuller M, Kapatkin A, Bruecker K, Holsworth I, Kass P, et al. (2014) Comparison of the tibial mechanical joint orientation angles in dogs with cranial cruciate ligament rupture. Can Vet J 55(8): 757-764.
-
Agnello KA, Holsworth IG, Caceres AV, Brown DC, Runge JJ, et al. (2014) Articular cartilage lesions of the patellofemoral joint in dogs with naturally occurring cranial cruciate ligament disease. Vet Surg 43(3): 308- 315.
-
Voss K, Damur D, Guerrero T, Hässig M, Montavon P (2011) Force plate gait analysis to assess limb function after tibial tuberosity advancement in dogs with cranial cruciate ligament disease. Vet Comp Orthop Traumatol 21(3): 243-249.
-
Johnson A, Broaddus K, Hauptman J, Marsh S, Monsere J, et al. (2006) Vertical patellar position in large-breed dogs with clinically normal stifles and large-breed dogs with medial patellar luxation. Vet Surg 35(1): 78-81.
-
Mostafa A, Griffon D, Thomas M, Constable P (2008) Proximodistal alignment of the canine patella: Radiographic evaluation and association with medial and lateral patellar luxation. Vet Surg 37(3): 201-211.
-
Miles J, Dickow M, Nielsen D, Jensen B, Kirpensteijn J, et al. (2012) Five patellar proximodistal positioning indices compared in clinically normal Greenland sled dogs. Vet J 193(2): 529-534.
-
Insall J, Salvati E (1971) Patella position in the normal knee joint. Radiology 101(1): 101-104.
-
Caton J, Deschamps G, Chambat P, Lerat J, Dejour H (1982) Patella infera. Apropos of 128 cases. Rev Chir Orthop Reparatrice appar Mot 68(5): 317-325.
-
Aparicio G, Abril JC, Albiñana J, Vanés FRS (1999) Patellar height ratios in children. J Pediatr Orthop B 8(1): 29-32.
-
Anagnostakos K, Lorbach O, Reiter S, Kohn D (2011) Comparison of five patellar height measurement methods in 90° knee flexion. Int Orthop 35(12): 1791- 1797.
-
Guénégo L, Serri P, Charru P, Verwaerde P (2018) Craniocaudal position and height decrease of the patella after modified Cranial Closing Wedge Osteotomy (AMA- based-CCWO) for treatment of cranial cruciate ligament disease. In: Proceedings of the 5th world veterinary orthopaedic congress ESVOT-VOS, Barcelona, Spain, pp: 296-297.
-
Slocum B, Slocum TD (1993) Tibial plateau leveling osteotomy for repair of cranial cruciate ligament rupture in the canine. Vet Clin N Am: Small Anim Pract 23(4): 777-795.
-
Dejardin L (2003) Tibial plateau levelling osteotomy. In: Slatter D, (Eds.), Textbook of small animal surgery. WB Saunders Company, Philadelphia, PA, pp: 2133-2143.
-
Vedrine B, Guillemot A, Fontaine D, Ragetly G, Etchepareborde S (2013) Comparative anatomy of the proximal tibia in healthy Labrador Retrievers and Yorkshire Terriers. Vet Comp Orthop Traumatol 26(4): 266-270.
-
Witte P (2015) Tibial anatomy in normal small breed dogs including anisometry of various extracapsular stabilizing suture attachment sites. Vet Comp Orthop Traumatol 28(5): 331-338.
-
Aertsens A, Alvarez JR, Poncet CM, Beaufrère H, Ragetly GR (2015) Comparison of the tibia plateau angle between small and large dogs with cranial cruciate ligament disease. Vet Comp Orthop Traumatol 28(6): 385-390.
-
Renwick A, McKee W, Emmerson T, House A (2009) Preliminary experiences of the triple tibial osteotomy procedure: tibial morphology and complications. J Small Anim Pract 50(5): 212-221.
-
Dismukes DI, Tomlinson JL, Fox DB, Cook JL, Witsberger TH (2008) Radiographic measurement of canine tibial angles in the sagittal plane. Vet Surg 37(3): 300-305.
-
Glassman M, Hofmeister E, Weh M, Roach W, Torres B, et al. (2011) Radiographic quantitative assessment of caudal proximal tibial angulation in 100 dogs with cranial cruciate ligament rupture. Vet Surg 40(7): 830- 838.
-
Caylor KB, Zumpano CA, Evans LM, Moore RW (2001) Intra- and interobserver measurement variability of tibial plateau slope from lateral radiographs in dogs. J Am Anim Hosp Assoc 37(3): 263-268.
-
Raske M, Hulse D, Beale B, Saunders W, Kishi E, et al. (2013) Stabilization of the CORA based leveling osteotomy for treatment of cranial cruciate ligament injury using a bone plate augmented with a headless compression screw. Vet Surg 42(6): 759-764.
-
Guénégo L, Payot M, Charru P, Verwaerde P (2016) Alignment of the anatomical and mechanical axes during cranial closing wedge osteotomy (AMA-based-CCWO) for treatment of CCL disease in 182 dogs. Results and complications. In: Proceedings of the European society of veterinary orthopaedic and traumatology congress, pp: 383-384.
- The Digital Stethoscope: Harnessing AI in Veterinary Medicine Without Losing Our Healing Touch
- Meningoencephalomyelitis of Unknown Etiology: Short-Term Effect of Two Treatment Protocols on Cerebrospinal Fluid
- Safety and Efficacy of the HomeoPet Cough in Domestic Pets –A Clinical and Correction Analysis Based Upon User Response Survey
- Non Human Animals Responses to Social Loss
- Owner Reported Clinical Outcomes of a Homeopathic Proprietary Preparation for the Treatment of Upper Respiratory and Nasal Disorders in Companion Animals
- Effects and Diagnostic Approach of Ultrasound in Veterinary Practice: A Systematic Review