Operative Removal of Ear Foreign Bodies: Analysis of Indications and Outcomes
In the head and neck, foreign bodies are most commonly lodged in the ears of young children. Adult cases are rare, but not unusual. Majority of the foreign bodies in the ear are removed with simple manoeuvres in an outpatient setup. Ear foreign bodies requiring surgical intervention under general anaesthesia are extremely rare. Our case series highlights the indications of such interventions and the outcomes encountered. A special emphasis is placed on the prognosis of facial nerve palsy after button battery induced injury.
Introduction
Of all the ENT emergencies, foreign bodies in the head and neck account for about 11% [1] of cases. Ear is the commonest site for lodgement of foreign bodies, especially in children [1]. It is not unusual to encounter foreign bodies in adults, which break while attempting to clean the ears. Majority of the foreign bodies present immediately and are removed by simple instrumentation on an outpatient basis. In some cases presenting late or in un-cooperative children, sedation might be required for safe removal. With availability of good clinical expertise and technology, a surgical intervention is very rarely indicated for removal of foreign bodies from the ear. Our series analyses the indications for which surgical intervention was required and also the complications encountered, with special emphasis on battery induced facial nerve palsy and its prognosis.
Case 1
A 6 year old girl presented with severe pain in the right ear, with a history of foreign body insertion 2 days back. Patient had underwent multiple attempts at removal by local practitioners prior to our review. On evaluation an oedematous proximal ear canal with tragal tenderness was noted. The foreign body was not visible due to the blood clot and oedema. The patient underwent foreign body removal under general anaesthesia as the oedema prevented any instrumentation beyond the foreign body. A limited endaural incision was made to deliver the foreign body and a small pearl was retrieved. A tear in the tympanic membrane was noted which healed progressively. The patient’s recovery was uneventful.
Case 2
A 3 year old male child had history of alkaline button battery insertion in the left ear, 1 month back. A local practitioner initially attempted removal of the battery, but failed. 12 hours post the failed attempt, patient developed left sided facial weakness. After 24 hours patient underwent battery removal under general anaesthesia in the local state college. He was then initiated on steroids for facial rehabilitation, but no benefit was appreciated. He was referred to our tertiary centre for further management. On examination he had purulent discharge with a macerated canal skin and left Otolaryngology Open Access Journal
sided grade 5 facial nerve palsy. Radiology (figure 1) was performed to evaluate the status of the air cell system. The patient underwent a trans-mastoid facial nerve decompression under general anaesthesia. Intra- operatively a large tympanic membrane perforation was identified with a bare promontory. The facial nerve canal was not dehiscent, but granulations were present over the bare canal bone. Decompression of the tympanic and partially the vertical segment of the facial nerve till just beyond the second genu were done. Patient was continued on IV antibiotics for osteitis and a trial of short course steroids was given. No significant improvement was noticed, excepting for cessation of discharge and pain. (figure2).
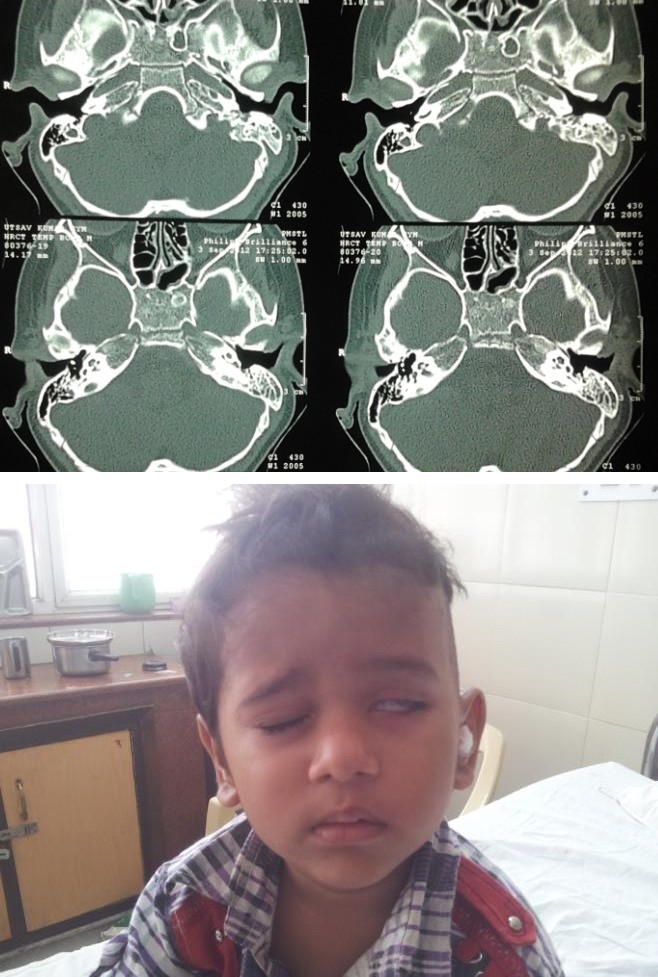
Figure 1
Figure 2
Case 3
An 8 year old male presented with complaints of blood tinged discharge and pain in left ear for 1 week. On evaluation active discharge with haemorrhagic clots were visible in the canal. A history of removal of a foreign body from the left ear 3 weeks back was present. As the child was not cooperative and was complaining of pain, removal was planned under general anaesthesia. Initial attempts with vasoconstrictors failed to create space for its retrieval. A rounded plastic piece of a toy was found embedded in the distal canal with a small perforation of the tympanic membrane. An end-aural incision was given to deliver the foreign body.
Case 4
A 6 year girl presented to our emergency with a history of alkaline button battery insertion into the right ear 2 hours back. Patient had a failed attempt at removal and was uncooperative. On evaluation a button battery was visualised in the deep meatus, with eroded proximal canal skin, probably due to the failed attempt. Patient was given general anaesthesia and removal tried with instrumentation. The oedema prevented atraumatic removal and so an end-aural incision was given to retrieve the battery without causing any trauma. The canal was then irrigated with saline and kept dry. The patient had an uneventful recovery.
Discussion
Removal of foreign bodies from the ear of children with or without sedation is a common occurrence in day to day ENT practice. Very rarely does the need for general anaesthesia with surgical intervention arise. The onus of evaluating the need for sedation or anaesthesia lies on the surgeon’s experience. One has to be very careful to prevent further iatrogenic injury due to failed attempts. In our cases the need for surgical intervention arose due to either a delayed presentation of the patient or in patients presenting with button batteries. The delayed presentation and failed attempts create a lot of oedema and trauma to the canal skin. The tympanic membrane perforation and discharge are sequel of such failed attempts. The usual practice of using vasoconstrictors and saline irrigation fails in cases presenting late and forceful instrumentation causes more injury and complications. Complications usually encountered are, tympanic membrane perforation, ossicular discontinuity, facial nerve injury and delayed canal stenosis [2]. A special mention is warranted for cases where a button battery is involved. Irrigation or forceful removal is contraindicated Otolaryngology Open Access Journal
as it can cause flow of residual current or leakage of chemicals, with severe tissue destruction. Our 2nd case developed facial nerve injury after manipulation of the battery under local anaesthesia, which could have been the trigger for the injury. The battery commonly encountered is an alkaline battery with an anode and cathode being separated by a strong alkaline solution. Sodium or potassium hydroxides are the commonly utilized electrolytes [3]. The proposed mechanisms of injury are electrical burns due to the residual charge, chemical burns due to the leaked alkali, pressure necrosis and rarely chemical toxicity due to the absorbed chemical [4]. The residual current in the battery causes injury and this conductivity is aided by the moist environment of exudates or even the cerumen [5] in the canal. The manipulation of the battery causes leakage of the alkali solution which causes severe tissue destruction. A liquefying necrosis [6] occurs with dissolution of proteins, saponification of lipids, and dehydration of tissue. The pressure caused by the battery along with the severe inflammatory reaction causes massive damage to the canal skin and precludes easy removal. Rarely the absorption of chemicals like mercury can cause mercury poisoning, sometimes warranting chelation therapy. In our case there was destruction of the canal skin, tympanic membrane and also current induced injury of the facial nerve. The facial nerve decompression and anti- inflammatory agents unfortunately failed in our case. The probable reason of nonimprovement could be due to the severe injury insult at the outset or the delayed intervention. The need for irrigation after removal of the battery is essential to clear the leaked chemicals and prevent further injury. The battery can also sometimes erode the medial wall and cause sensorineural hearing loss [3], but fortunately in our case no such complication was encountered. Conclusion A surgical intervention is rarely but surely required in select cases. A rounded foreign body with no grip to hinge the instrument carries a high risk of iatrogenic injury. The delayed presentation causes lot of oedema and tissue destruction, thus preventing easy removal. Special care should be taken while removing button batteries as they can cause very severe tissue destruction with a poor prognosis. Usual practices like irrigation, vasoconstrictor use and forceful or delayed removal should be avoided in cases with button batteries. Ultimately the surgeon has the onus for identifying such difficult patients and plan for a surgical intervention, to prevent further iatrogenic injury.
References
-
Figueiredo RR, de Azevedo AA, de Avila Kos AO, Tomita S (2008) Complications of ent foreign bodies: a retrospective study. Rev Bras Otorinolaringol. 74(1): 7-15.
-
Kavanagh K, Litovitz T (1986) Miniature battery foreign bodies in auditory and nasal cavities. Journal of the American Medical Association 255 (11): 1470- 1472.
-
McRae DJPD (1990) Severe tissue destruction in the ear caused by alkalinebutton batteries. Postgrad Med J 66(771): 52- 53.
-
Lin VYW, Daniel SJ, Papsin BC (2004) Button batteries in the ear, nose and upper aerodigestive tract. International Journal of Pediatric Otorhinolaryngology 68(4): 473-479.
-
Capo JM, Lucente FE (1986) Alkaline battery foreign bodies of the ear and nose. Arch Otolarvngol Head Neck Surg, 112(5): 562-563.
-
Houck JC, DeAngelo L, Jacob RA (1962) The dermal chemical response to alkali injury. Surgery 51: 503 - 507.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?