Correlation of Clinical and Hematological Findings with the Bony Erosion in Patients of Allergic Fungal Sinusitis
Variation in the clinical, hematological parameters in patients of AFRS has well been documented in the past literatures. Few studies have also reported erosion of bony sinus and skull base in patients associated with AFRS. However we have focused the correlation of clinical, hematological and microbiological findings with that of the CT findings in 80 patients of AFRS, diagnosed by Bent and Kuhn's criteria. Material and Method: This was a prospective study conducted in the department in otorhinolaryngology in a tertiary care referral hospital from July 2013 to January 2015.Total 80 patients (50 primary cases and 30 revision cases) of AFRS with nasal polyposis were included in the study. Clinical (Sino-Nasal Outcome Test [SNOT-20], hematological tests (absolute eosinophil count, Serum IgE) and microbiological findings were correlated with the CT scan. Result: Characteristic heterogeneous density in CT scan finding was present in 60(75%) patients and combined skull base and orbital erosion was found in 18 cases. Average pretreatment AEC level in the primary and revision cases were 532 microg/L and 592microg/L respectively and whenbone erosion was taken in to account, these values were 570 microg/L and 510 microg/L respectively (P=0.093). The mean serum IgE level in primary and revision patients were 850.20IU/ml and 790 IU/mlrespectively and the respective values were 855 IU/ml and 827 IU/mlon correlation with the bone erosion(p=0.062). Similarly the mean SNOT score was 52.5(51 for primary and 66 for revision cases) and on considering the bony erosion it was found to be 68.4(59 for primary cases and 62.75 for revision cases) (p=0.148). Conclusion: Characteristics CT finding is an important parameter for the clinical diagnosis of AFRS. Although clinical and hematological parameters are closely related to each other, there was no direct relationship between patients with and without erosion of the bone.
Introduction
Allergic fungal rhino sinusitis (AFRS) has always been remained a topic of discussion despite of the availability of adequate literature for the diagnosis and its treatment protocol even after decades of research. AFRS is an inflammatory response (type I and type III) to a host when later is exposed to the environmental fungi which later produce mucosal edema and obstruction of the sinus ostium. Again stasis of the mucous in the sinuses creates an ideal environment for the proliferation of the fungus. At some point, the cycle becomes self-perpetuating, resulting in the eventual product of this process i.e. allergic mucin, the material that fills the involved sinuses of patients with allergic fungal sinusitis. The production of this allergic mucin and its clinical, histologic, and radiographic characteristics are unique to AFRS and serve as a hallmark of the disease. Although most of the time patients are diagnosed by Bent- Kuhn’s criteria yet radiological findings contribute an important role for the diagnosis of AFRS in the outpatient department. Subtotal or total heterogeneous opacity in the sinus cavity with expansion or destruction of the adjacent bone are often considered pathognomonic for the diagnosis for AFRS. There have been various past literatures demonstrating the variation in the hematological (serum IgE, absolute eosinophil count) and clinical parameter (Sino-Nasal Outcome Test [SNOT-20] associated with AFRS. Few studies have reported the erosion of bone including the skull base in patients with AFRS, however we have focused the correlation of clinical, hematological and microbiological findings with that of the CT findings in patients of AFRS as diagnosed by Bent- Kuhn’s criteria.
Materials and Methods
This is a prospective study was conducted in the department in otorhinolaryngology in a tertiary care referral hospital from July 2013 to January 2015. Total 80 patients (50 primary cases and 30 revision cases) with allergic fungal sinusitis with nasal polyposis were considered for the study. Patients in the age group of 5-60 years, diagnosed as Allergic Fungal Rhinosinusitis according to Bent and Kuhn’s criteria were included in the study. Patients with chronic systemic illness were not included in the study. After clinical examination of the patients, hematological evaluation (complete blood count, absolute eosinophil count [AEC]) immunological (Serum IgE) and intradermal skin test for fungus (Aspergillus species) were carried out. Pre-operative non contrast computed a tomography nose and paranasal sinus (CT scan with 3mm axial and coronal cuts) was performed for each patient to see the involvement of sinus and to look for the heterogeneous opacity along with the bony erosion. Diagnostic nasal endoscopy (DNE) was done in each patient for the assessment of nasal mass, nasal polyp, allergic mucin, and nasal discharge preoperatively before undergoing CT scan. Clinical assessment using Sino-Nasal Outcome Test [SNOT-20] scoring was performed for each patient before undergoing surgery and in each follow up periods. Patients were given a course of antibiotics, antihistaminic and systemic steroid for one week prior to surgery. Each patient underwent functional endoscopic sinus surgery (FESS) by single surgeon. Intra-operatively nasal swabs were taken for cytological evaluation of charcotlayden crystals, fungal hyphae, allergic mucin, mast cells, eosinophils and basophil. The specimen (allergic mucin, debris, polyp) were sent for fungal microscopy, fungal culture and sensitivity and histopathological evaluation. Preoperative clinical, hematological parameters are compared with the radiological findings for each patient.
(Table 1) Of 80 patients 52 were males and 28 were female. Majority of patients in our study population were in the age group of 21-30 years i.e. 68(85%) and 12 (15%) patients were in the age group of 11-20 years. Of 80 cases, 50 cases were primary cases and 30 cases were revision cases. 50 (62.5%) patients were suffering from disease for 1-2 years, 18(22.5%) and 12(15%) had a duration of symptoms for <1 year and 3-5 years respectively. Nasal obstruction, nasal discharge and headache were found in 46(%), 18(%) and 16(%) of patients respectively. Considering the Kuperberg endoscopic grading all 60 patients was endoscopic grade 4 preoperatively. Characteristic heterogeneous density in CT scan finding was present in 60(75%) patients and combined skull base and orbital erosion was found in 18 cases (11 patients in primary cases and 7 in revision cases)and were mostly seen in the males (72.22%c cases). Isolated sphenoid sinus was affected in 2(2.5%) patients. One patient (1.2%) in the revision group had decreased vision (visual acuity 6/36 in right eyein the preoperative period due to the erosion of the sphenoid roof which had regained its visual acuity in the immediate postoperative period. Nasal discharge and allergic mucin were present in 56(70.0%) and 53(66.7%) patients respectively. 63.3% (50cases) were found positive for intra dermal skin test for Aspergillus species. Histopathological evaluation was found to be consistent with nasal polyp with inflammation and PAS stain for fungal pathology was positive in 16(88.88%) cases and the most common isolate was Aspergillus flavus as shown in (Figure 1).
| Clinical | Primary | Revision | ||||||
|---|---|---|---|---|---|---|---|---|
| characteristic | cases | cases | ||||||
| No of patients | 50 | 30 | ||||||
| Male | 50 | 3 | ||||||
| Female | 22 | 5 | ||||||
| No of patients with raised AEC | 8 | 4 | ||||||
| Mean preoperative AEC | 532microg/L | 592microg/L | ||||||
| Mean AEC (When bone erosion was considered) | 570microg/L | 510microg/L | ||||||
| No of patients with raised IgE | 39 IU/ml | 23 IU/ml | ||||||
| Mean preoperative IgE | 850.20IU/ml | 790 IU/ml | ||||||
| Mean IgE (When bone erosion was considered) | 855 | 827 | ||||||
| Mean preoperative SNOT score | 51 | 66 | ||||||
| Mean SNOT score(When bone erosion was considered) | 59.4 | 62.75 | ||||||
| Isolation of Aspergillus | 29 | 15 | ||||||
| When correlated with bone erosion | 22 | 17 |
Table 1: Evaluation of Prospective study.
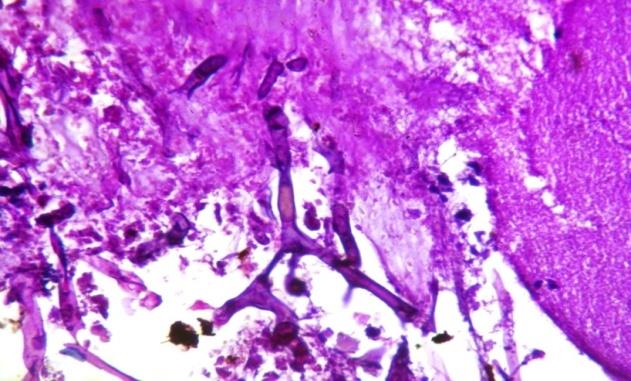
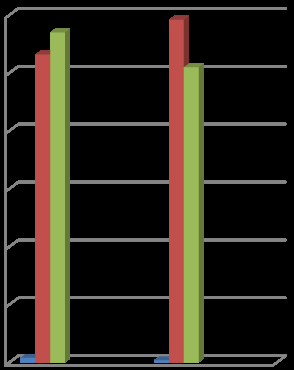
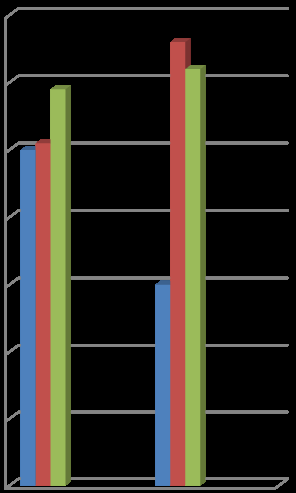
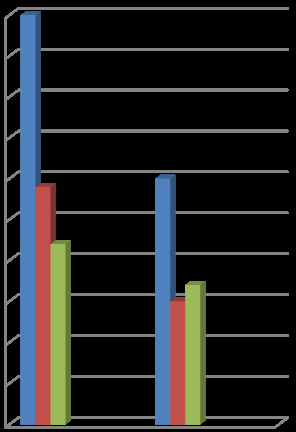
Figure 1: HE section showing pauci septate hyphae suggestive of Aspergillus Flavus (400x). 12 cases (8 from primary cases and 4 from revision cases) had presented with elevated AEC in the preoperative period. Average pretreatment AEC level in the primary and revision cases were 532microg/L and 592microg/L respectively and the difference was not considered significant (0.182). When AEC was correlated for the patients with bone erosion, it has been found that, the mean AEC for primary and revision cases were 570 microg/L and 510 microg/L respectively (P=0.093) as shown in the (Figure 2). In 62 (77.50%) cases (39 primary cases and 23 revision cases), serum IgE was elevated in the preoperative period. The mean pre- operative serum IgE level in primary and revision patients were 850.20IU/ml and 790 IU/ml respectively and the difference was significant (p=0.062) as shown in (Figure 3). On correlating the radiological findings, it has been seen that the mean IgE level in primary patients was 855 IU/ml and for the revision case it was 827 IU/ml although there was no direct correlation between the serum IgE values to that of bony involvement in patients with AFRS. Surgical management with endoscopic techniques was successful for all patients. Aspergillus was isolated in 44(56%) patients (29 primary cases and 15 revision cases) and was the most common etiological agent. When it was correlated with the erosion of bone, 39(88.63%) cases (22 cases primary and 17 cases revision) found positive for Aspergillus (p=0.52) as shown in (Figure 4). The mean SNOT score was 52.5 (for primary cases it was 51 and for the revision cases it was 66) in the preoperative period and when considered patients with bony erosion it was found to be 68.4(59 for primary cases and 62.75 for revision cases) and the difference was found insignificant (p=0.148) as shown (Figure 5). No statistical co-relation was found between KOH mount and serum total IgE and wit the preoperative CT scan findings. There was no significant intraoperative complications encountered in the current study except 1 patient who had periorbital swelling and 3 patients had postoperative nasal bleeding which were managed conservatively in the postoperative period.
Non contrast CT scan of nose and paranasal sinus is the mainstay for the diagnosis of the AFRS in the outpatient rhinology clinics and often considered as the road map to guide in the intraoperative period. Not only it focuses the involvement of the paranasal sinuses but also it provides the important information in detecting the fungal debris and the erosion of the bony wall of the sinuses with adjacent vital structures. Radiological changes are thought to be the characteristics of AFRS [1] and have been identified as an important criteria for its diagnosis [2]. Although heterogeneous opacification is seen in majority of cases, significant proportion of patient doesn’t exhibit the typical features of CT scan. In spite of great variation in the involvement of the paranasal sinuses in patients with AFRS, the most frequent site being affected is the anterior ethmoid cells followed by maxillary sinus and frontal sinus being the least common sinus affected as was demonstrated in the current study. Irrespective of all radiological changes, hyper attenuation in the CT scan is found in 100% of cases of in patients of AFRS as described by Dhiwakar, et al. [3]. But variable results are found in the past literature and in the current study it was found to be 60(75%) which was further supported by Li Y, et al. [4] where 78% of cases had calcified dots in the soft tissue window. Again, bony erosion in patients with AFRS varies significantly and in the current study it was detected to be 22.5%. Similar study conducted by Nussenbaum B, et al. [5] where around 20% of the patients of AFRS had radiological bone erosion and it was as high as (56%) as described by Ghegan MD, et al. [6]. Again in the present study, one case had decreased vision in the preoperative period due to the erosion of the lateral wall of the sphenoid sinus which was improved after surgery in the immediate postoperative period. In the current study 75% of the cases had presented with increased IgE as supported by similar studies conducted by Goh BS, et al. [7] & Ravi Kumar, et al. [8] where 56.7% and 60% patients had increased serum IgE levels respectively. Of 62 cases with raised IgE, 16 patients had radiological features of erosion of bone and rest 2 patients had only heterogeneous opacity without bone erosion. Although there was no direct correlation between the IgE level and the bone erosion, yet 88.88% of cases of patient having destruction had raised level of IgE. But when it was compared between the primary and revision cases it was found insignificant (p> 0.05). Similarly 15% (12) of cases presented with raised AEC, of which 5(41.66%) had presented with radiological destruction of the bone although there was no significant difference noted between them (p > 0.05). Although there was no direct correlation between AEC and serum IgE with the radiological bony destruction in patients of AFRS, still IgE level can be considered as a better indicator than AEC for the severity of bony involvement in AFRS. On correlating the symptomology, it has been found that there was no significant difference in the mean SNOT score with or without erosion of the bone in patients with AFRS as described by White LC, et al. [9]. Again there was no direct correlation between the endoscopic grading and the bone destruction in AFRS. Allergic mucin was detected found in 100% of cases of AFRS in the intraoperative period and Aspergillus flavus was isolated in 90% (16) of cases in patients with radiological bony erosion. There were no significant difference in the intraoperative complications encountered in the patients with bone destruction and those who did not have.
Conclusion
Bony erosion can be detected in significant no of patients with AFRS. Although clinical and hematological parameters are closely related to each other, there was no direct relationship of these parameters in relation to the severity of the bony involvement. A thorough anatomical knowledge in an expert hand can overcome the complications attributed to the bony erosion with similar success rate to that of the patients without bony destruction.
References
-
Manning SC, Merkel M, Kriesel K, Vuitch F, Marple B (1997) Computed tomography and magnetic resonance diagnosis of allergic fungal sinusitis. Laryngoscope 107(2): 170-176.
-
Bent JP III, Kuhn FA (1994) Diagnosis of Allergic fungal sinusitis. Otolaryngol Head Neck Surg 111(5): 580-588.
-
Dhiwakar M, Thakar A, Bahadur S, Sarkar C, Banerji U, et al. (2003)Preoperative diagnosis of allergic fungal sinusitis. Laryngoscope 113(4): 688-694.
-
Li Y, Li Y, Zhang G, Liu X, Ye J (2004) Computer tomography characteristics of chronic invasive fungal rhinosinusitis in early stage. Lin Chuang Er Bi Yan Hou Ke Za Zhi 18(5): 282-284.
-
Nussenbaum B, Marple BF, Schwade ND (2001) Characteristics of bony erosion in allergic fungal rhinosinusitis. Otolaryngol Head Neck Surg 124(2): 150-154.
-
Ghegan MD, Lee FS, Schlosser RJ (2006) Incidence of skull base and orbital erosion in allergic fungal rhinosinusitis (AFRS) and non-AFRS. Otolaryngol Head Neck Surg 134(4): 592-595.
-
Goh BS, Gendeh BS, Rose IN, Pit S, Samad SA (2005) Prevalence of allergic fungal sinusitis in refractory chronic rhinosinisitis in adult Malaysians. Otolaryngol Head Neck Surg 133(1): 27-31.
-
Ravikumar A, Mohanthy S, Vatsanath RP, Raghunandan S (2004) Allergic Fungal Sinusitis-a clinicopathological study. Ind J Otolaryngol Head Neck Surg 56(4): 317-320.
-
White LC, Jang DW, Yelvertan JC, Kountakis SE (2015) Bony erosion patterns in patients with allergic fungal sinusitis. Am J Rhinol Allergy 29(4): 243-245.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?