Nasal and Laryngeal Non-Hodgkin’s Lymphoma: A Case Report
Among head and neck malignancies, lymphoma is the second most frequent cause. They can develop in the head and neck lymph nodes or as extranodal determinations. The onset of malignant lymphoma outside of lymph node registers increasingly frequent, currently over 30% of malignant lymphoma are diagnosed as taking place outside the lymph nodes. The aim of this paper is to describe a rare case of double location of non-Hodgkin's nasal and laryngeal lymphoma and the modalities of diagnosis and treatment even the lack of studies in the literature.
Introduction
The NHL larynx represents less than 1% of all laryngeal tumors. Less than 100 cases have been reported in the literature. Although they are in 2nd place in frequency in ENT, malignant lymphomas with sinonasal onset are still rare, accounting for about 5% of primary extranodal lymphomas. The presence of both nasal and laryngeal malignant lymphoma location at the same time is extremely rare. This is what we will describe in this study.
Case Report
It is about a 65 years old man consulting for nasal obstruction especially in the left side, answering local medical treatment with episodes of dyspnea and dysphonia is resolvent after medical treatment . In the neck palpation, there is some cervical lymph nodes, all operating in a conservation context of the general condition. Video laryngoscopy and shows a diffuse laryngeal edema, with mass of the left side wall of the naso pharynx. The vocal cords are movable (Figure1).
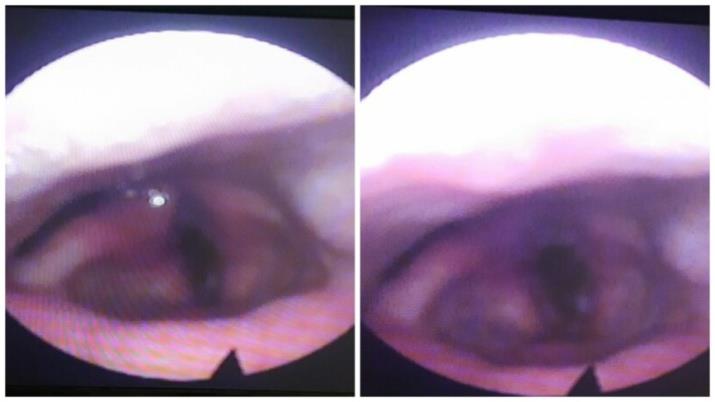
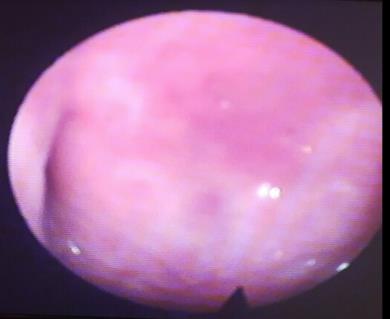
Figure1: Video laryngoscopy showing the diffuse edema of the throat. The patient carried out a panendoscopy showing edematous appearance throughout the extra glottal region with diffuse inflammation. A biopsy was done. In the nasal endoscopy, burgeoning mass of the right side wall of the nasopharynx bleeding on contact. A biopsy was done too (Figure 2).
Discussion
Malignant lymphomas, defined as neoplasm of lymphoid B- or T-cells, are one of the topical problems of modern medicine. Although Hodgkin’s lymphoma records stagnation or even a decrease in incidence in recent years, non-Hodgkin’s malignant lymphoma is lately growing by at least 5% per year ranking the 3rd place in terms of growth rate after lung cancer and malignant melanoma [1]. Improving biology and molecular genetics techniques, the contribution of immune histochemistry and immune phenotyping and the development of new high performance imaging methods have enabled special clarifications regarding the diagnostic accuracy of this pathological entity, allowing the use of the most appropriate course of treatment [2]. Among head and neck malignancies, lymphoma is the second most frequent cause. Although most malignant lymphoma arises in the lymph nodes, the onset of malignant lymphoma outside of lymph nodes is registered increasingly frequent, currently a significant proportion of over 30% of cases having extranodal origin and presenting special pathogenic features, both clinical and therapeutical. This has led this group of lymphoproliferative transformations to be given increased attention in recent years [3, 4]. There are numerous subtypes of lymphoma, the main two being HL and NHL [5]. NHLs constitute a heterogeneous group of malignancies characterized by abnormal clonal proliferation of T cells, B cells, or both. Approximately 90% of lymphomas are NHLs [6]. The risk factors for common types of NHL include autoimmune diseases, HIV/AIDS, infection with human T-lymphotropic virus, consuming large amounts of meat and fat, immunosuppressive medications and certain pesticides [7]. The symptoms of lymphoma may include enlarged lymph nodes, fever, cold sweats, weight loss, pruritus and fatigue [8, 9]. The diagnosis is usually confirmed by lymph node biopsy. In this case, Lymphoma was suspected just after double biopsy nasal ant laryngeal. Imaging may then be performed to determine whether the cancer has spread and to which location. Spread most commonly occurs to the lungs, liver and/or brain [9]. The head and neck is the second most common region for extranodal lymphoma, the first being the gastrointestinal tract [10]. Extranodal NHLs occurring primarily in the epiglottis are extremely rare, accounting for merely 0.7% of all NHLs and 1% of malignant laryngeal tumours [7]. Supraglottic cancer is almost exclusively squamous cell carcinoma In literature, malignant lymphoma of the head and neck frequently include ENT (ear, nose & throat) lymphomas. Otorhinolaryngology lymphomas represent an important group of lymphomas with extranodal onset, being 2nd in frequency after digestive lymphomas. Their percentage is 5-10% of non-Hodgkin’s malignant lymphomas, including lymphoproliferation that arise in the Waldeyer’s lymphatic ring, in the nose and paranasal sinuses and in the larynx, the pharynx, the thyroid and the salivary glands. The starting point is the mucosa associated lymphoid tissue (MALT) that is already recognized as being particularly rich in this area [11, 12]. In the pathogenesis of ENT lymphomas, there are many factors involved with the role of antigenic stimulation at this level (especially chronic inflammation), an important role in this aspect being held by viral infectious agents: Epstein– Barr virus, human T-cell leukemia virus type 1 (HTLV-1), human herpesvirus-8 (HHV-8) [13, 14]. Natural killer/T (NK/T)-cell lymphoma in the larynx is extremely rare, as only 29 cases have been previously reported in the English-language, Japanese-language, and Chinese- language literature. Its characteristics have never been systematically illustrated. A recent study was done about throat lymphoma [15] it is about 2 new cases of laryngeal NK/T-cell lymphoma. In our case, NH lymphoma type T is described. The NHL larynx represents less than 1% of all laryngeal tumours. Our patient doesn’t have cervical lymph nodes clinically palpable, and making the diagnosis of lymphoma was slowly because of the clinical signs and the need for nasal and laryngeal biopsy with two immune histochemical studies. The clinical and progressive histological heterogeneity onset of sinonasal malignant lymphomas brings into question many aspects of the diagnostic and therapeutic point of view. An essential role for proper management of these lymphoproliferative modifications is in the histopathological and immune histochemical examinations in detail of the part excised. Although they are in 2nd place in frequency in ENT, malignant lymphomas with sinonasal onset are still rare, accounting for about 5% of primary extranodal lymphomas. The maxillary sinus is the most common. It represents about 6% of sinonasal tumours [16, 17]. The NK/T-cell nasal lymphoma is extremely aggressive, with a tendency to important local extension (especially the orbit, palate and soft parts) and to central nervous system. The B- phenotype is more common in sinus localizations, while T-phenotype is more common in the nasal cavity, like our case report. Lymphomas developed by T-lymphocyte proliferation frequently evolves with obstructive lesions and with nasal septum perforation [18, 19]. In terms of diagnosis, these entities bring important concerns in terms of distinguishing from non-neoplasic diseases of destructive nature (such as Wegener’s granulomatosis) or other neoplasms development at this level, due to the association of inflammatory infiltrates with non specific neoplastic tissue. It is thus mandatory to collect multiple biopsy fragments from suspicious areas and the size of these fragments must be large enough. In terms of therapeutic attitude, therapeutic means used were: multi-agent chemotherapy, surgical treatment, radiation therapy and monoclonal antibodies treatment. Although malignant lymphoma is par excellence a blood disease, we found an increasing role of surgical procedures as part of complex multimodal therapy in malignant lymphoma with sinonasal localization. The contribution of surgery was complex: diagnostic, curative ablation, solving complications (video-assisted orbital decompression), drainage for the control of associated septic phenomena, hemostasis in the remaining area after tumor ablation (using argon plasma coagulation) [20]. Given the high degree of malignancy of the sinonasal malignant lymphomas, their destructive, invasive and locally extensive and frequent determinations in the central nervous system, most of these cases received radiationtherapy treatment more than other localizations, associated with surgery, polychemotherapy and treatment with monoclonal antibodies (mostly Rituximab), which is consistent with data presented in literature [21, 22].
Conclusion
Malignant lymphoma of the head and neck frequently include ENT (ear, nose & throat) lymphomas. Otorhinolaryngology lymphomas represent an important group of lymphomas with extranodal onset, being 2nd infrequency after digestive lymphomas. The simultaneous presence of nasal and laryngeal lymphoma and very rare and it is not described in the literature, so that this work is interesting and still to be discussed and need for another study to explain this phenomenon.
References
-
Greer JP, Foerster J, Rodgers GM, Paraskevas F, Glader B, et al. (2009) Means RT Jr (Eds.) Wintrobe’s clinical hematology (12th edn), Lippincott Williams & Wilkins, Philadelphia, 2071-2130.
-
Isaacson PG (2000) The current status of lymphoma classification. Br J Haematol 109(2): 258-266.
-
Vlădăreanu AM (2002) Actualităţi în limfoamele maligne nonhodgkiniene (edn) Medicală Amaltea, Bucureşti, pp. 13-16.
-
Oltean G (2010) Limfoamele maligne cu debut extraganglionar (edn) Veritas, Târgu-Mureş, pp. 112- 133.
-
Bardia A (2010) Johns Hopkins Patients Guide to Lymphoma (1st edn) Jones and Bartlett Publishers, USA, pp. 6.
-
(2014) Leukemia and Lymphoma Society: The Lymphoma Guide Information for Patients and Caregivers.
-
King AD, Yuen EH, Lei KI, Ahuja AT, Van Hasselt A (2004) Non-Hodgkin lymphoma of the larynx: CT and MR imaging findings. AJNR Am J Neuroradiol 25(1): 12-15.
-
National Cancer Institute (2014) General Information about Adult Hodgkin Lymphoma.
-
National Cancer Institute (2014) General Information about Adult Non-Hodgkin Lymphoma.
-
Jacobs C, Weiss L, Hoppe RT (1986) The management of extranodal head and neck lymphomas. Arch Otolaryngol Head Neck Surg 112: 654-658.
-
Behrbohm H, Kaschke O, Nawka T, Swift A (2009) Ear, nose, and throat diseases with head and neck surgery (3rd edn) Georg Thieme Verlag, Stuttgart, pp. 398-402.
-
Catovsky D, Ralfkiaer E, Müller-Hermelink HK (2001) T-cell prolymphocytic leukaemia. In: Jaffe ES, et al. (eds.) Pathology and genetics of tumours of haematopoietic and lymphoid tissues. World Health Organization (WHO) Classification of Tumours, International Agency for Research on Cancer (IARC) Press, Lyon: 195-196.
-
Heslop HE (2005) Biology and treatment of Epstein- Barr virus associated non-Hodgkin lymphomas; Oral presentation at 47th Annual Meeting of the American Society of Hematology, Atlanta, Georgia. Hematology Am Soc Hematol Educ Program 260-266.
-
Vlădăreanu AM (2007) Limfoamele în corelaţie cu virusurile limfotrope (edn) Medicală Amaltea, Bucureşti, 159-205.
-
Zhu SY, Yuan Y, Liu K, Zeng L, Zhou JM, et al. (2016) Primary NK/T-cell lymphoma of the larynx: Report of 2 cases and review of the English, Japanese, and Chinese language literature. Ear Nose Throat J 95(4- 5): E1-8.
-
Han X, Kilfoy B, Zheng T, Holford TR, Zhu C, et al. (2008) Lymphoma survival patterns by WHO subtype in the United States, 1973–2003. Cancer Cause Control 19(8): 841-858.
-
Laskin JJ, Savage KJ, Voss N, Gascoyne RD, Connors JM (2005) Primary paranasal sinus lymphoma: natural history and improved outcome with central nervous system chemoprophylaxis. Leuk Lymphoma 46(12): 1721-1727.
-
Hochberg J, Waxman IM, Kelly KM, Morris E, Cairo MS (2009) Adolescent non-Hodgkin lymphoma and Hodgkin lymphoma: state of the science. Br J Haemato 144(1): 22-40.
-
Cheson BD (2008) Staging and evaluation of the patient with lymphoma. Hematol Oncol Clin North Am 22(5): 825-837.
-
Tuşaliu M, Zainea V (2014) Indications and surgical techniques in malignant sinonasal lymphomas. Arch Balkan Med Union 49(1): 87-93.
-
Soutar R, Lucraft H, Jackson G, Reece A, Bird J, et al. (2004) Guidelines Working Group of the UK Myeloma Forum; British Committee for Standards in Haematology; British Society for Haematology. Guidelines on the diagnosis and management of solitary plasmacytoma of bone and solitary extramedullary plasmacytoma. Br J Haematol 124(6): 717-726.
-
Tuşaliu M, Mogoantă CA, Dobrea CM, Zainea V (2015) Clinical and histological aspects with therapeutic implications in head and neck lymphomas. Rom J Morphol Embryol 56(2): 499-504.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?