Management of Tracheoesophageal Fistula Secondary to Button Battery Ingestion
Introduction: Foreign body ingestion in children is a common problem encountered and treated by both pediatricians and otolaryngologists. The increased use of electronic devices has paralleled the increasing incidence of battery ingestions. Ingestion of the disc batteries can be fatal by causing burns in the trachea and the esophagus, resulting in an acquired tracheoesophageal fistula. We report on a child with tracheoesophageal fistula secondary to disc battery ingestion in which primary repair was performed successfully. There are several options of closure of a tracheoesophageal fistula. In our case, it was repaired using an inferiorly based sternocleidomastoid flap which gave excellent result.Conclusion: Increased public and health personnel awareness is necessary to diminish the incidence of battery ingestion and its related sequelae. Though exceedingly rare, physicians who treat battery ingestion injuries in children should be aware of the possible serious and fatal adverse outcomes, and facilitate prompt medical and surgical therapy.
Introduction
Foreign body ingestion in children is a common problem encountered and treated by both pediatricians and otolaryngologists. While coins are still the most common foreign bodies swallowed in children, ingestion of batteries became more frequent in recent years among children, due to the increasing accessibility to electronic toys and devices by children [1]. Ingestion of the disc batteries can be fatal by causing burns in the trachea and the esophagus, resulting in an acquired tracheoesophageal fistula [2, 3, 4]. The mechanisms include absorption of toxic substances, electrical injury, pressure necrosis, and caustic injury from leaking battery contents. The size of the battery impacts the risk of esophageal entrapment. Lithium batteries generate twice the voltage (3 V) of alkaline batteries, and are more than twice as likely to cause major injury. The increased use of electronic devices has paralleled the increasing incidence of battery ingestions. Timely and prompt removal is critical. We report on a child with tracheoesophageal fistula secondary to disc battery ingestion in which primary repair was performed successfully.
Case Report
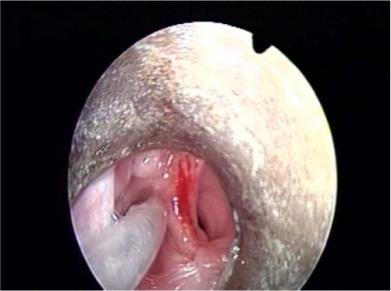
A 2 yr old female child presented to ENT emergency with symptoms of sudden onset of cough and difficulty in swallowing since three days. Patient was apparently normal three days back when she was playing in house and developed sudden cough and vomiting. She was taken to local doctor and managed for URI. Symptoms of cough and difficulty in swallowing persisted. X-ray chest was taken after two days which showed radiopaque foreign body, so patient was referred to Govt. medical college and hospital Chandigarh. Patient was admitted and a repeat X- ray showed foreign body at the level of cricopharynx. Oesophagoscopy under general anesthesia was done in emergency and metallic foreign body approx. 2 x1 cm was seen lying just below cricopharynx, covered with slough. Foreign body was removed and it was found to be a button cell. Patient was extubated and shifted to ENT ward. On 4th post op day oral trial was given, patient developed severe cough possibly due to aspiration. A chest x-ray was done which showed aspiration pneumonitis. The respiratory system examination showed bilateral air entry equal but rhonchi was present over bilateral lower lobes. A diagnosis of tracheoesophageal fistula secondary to foreign body (button cell) was kept. Repeat rigid esophagoscopy was done after one day which showed defect between esophagus and trachea. A defect measuring approx. 2.5cm craniocaudally and 1.5cm transverse was visualized. The endotracheal tube could be seen through the defect. After one week, patient was taken up for primary tracheoesophageal repair under general anesthesia. Using collar incision, the margins of tracheoesophageal fistula was exposed superiorly and inferiorly. A primary repair of esophageal mucosa was undertaken with vicryl 3-0 followed by primary repair of trachea with ethilon 3-0. An inferiorly based sternocleidomastoid muscle flap was inserted in between trachea and esophagus and was sutured. Post-operative recovery was good; patient started taking orally after two weeks and there was no identifiable leak. The patient followed up in our opd after 3 and 6 months respectively and a barium swallow was done which was essentially normal (Figure 1 & 2).
Discussion
Disc battery ingestion has become an increasingly common occurrence in the pediatric population. According to the American association of poison control centers, 10,213 cases of battery exposures were documented across the US in 2007 [5]. Unlike traditional foreign bodies in children such as coins, ingestion of the disc batteries can be fatal by causing burns in the trachea and the esophagus, resulting in tracheoesophageal fistula [2]. One major problem confronted in these cases is delayed presentation. The most common signs and symptoms of battery ingestion include, in a decreasing order, vomiting, abdominal pain, discolored stools, fever, diarrhea, rashes, respiratory distress, irritability, food refusal, and dysphagia [5]. The affected children may present with various symptoms including dysphagia, dyspnea, choking, and pneumonia with considerable delay ranging from 4 hours to 4 weeks [3]. It has been reported that esophageal perforation can occur as soon as 6 hours after battery ingestion if it is impacted in the esophagus [6]. Therefore, it is generally agreed that the immediate removal of the impacted battery should have the highest priority. Standard radiologic workup for suspected battery ingestion is chest film, in AP and lateral views. X-ray films have high availability, low costs and high accuracy in outlining radiopaque objects. However, there is no consensus on how to treat the tracheoesophageal fistula if present. Surgical treatment is the mainstay of therapy traditionally, but recently there has been a trend toward more conservative medical management [7]. Nevertheless, conservative management carries high risk of respiratory distress because of aspiration and pneumonia, especially in cases of large fistula. In the current case, total rest of esophageal mucosa by total parenteral nutrition failed to relieve difficulty in swallowing and respiratory symptoms. Early surgical intervention should be considered in patients with serious respiratory symptoms. Most reported therapeutic strategies involve surgical intervention in multiple stages. Repair of an acquired corrosive tracheoesophageal fistula by simple 1-staged closure is unsuitable if the adjacent tissue also is affected. As reported in literature a case in which failure of primary repair of the tracheoesohageal fistula resulted in 2 episodes of recurrence [8]. In literature, also reported is a case of multiple staged surgical interventions, which consisted of cervical esophagostomy and colon interposition [9]. As we showed in this case, the anterior cervical approach via lower collar incision provides an excellent access to the fistula even if severe inflammation around the fistula is present. Moreover, attaching the sternocleidomastoid muscle between trachea and esophagus is thought to be useful to avoid any recurrence of the fistula. The cosmetic result in this case also is excellent.
Conclusion
Increased public and health personnel awareness is necessary to diminish the incidence of battery ingestion and its related sequelae. Though exceedingly rare, physicians who treat battery ingestion injuries in children should be aware of the possible serious and fatal adverse outcomes, and facilitate prompt medical and surgical therapy.
References
-
Gregori D, Salerni L, Scarinzi C, Morra B, Berchialla P, et al. (2008) ESFBI Study Group, Foreign bodies in the upper airways causing complications and requiring hospitalization in children aged 0-14 years: results from the ESFBI study, Eur Arch Otorhinolaryngol 265(8): 971-978.
-
Peralta M, Fadda D, Contreras L (1991) Tracheoesophageal fistula secondary to ingestion of a button battery. Rev Child Pediatr 62(6): 378-381.
-
Jones ML, Lyall MH, McCollum P (1992) Disc battery ingestion: A review and a management plan. J R Coll Surg Edinb 37(2): 120-122.
-
Grisel JJ, Richter GT, Casper KA, Thompson DM (2008) Acquired tracheoesophageal fistula following disc-battery ingestion: can we watch and wait? Int J Pediatr Otorhinolaryngol 72(5): 699-706.
-
Yardeni D, Yardeni H, Coran AG, Golladay ES (2004) Severe esophageal damage due to button battery ingestion: can it be prevented? Pediatr Surg Int 20(7): 496-501.
-
Litovitz TL (1983) Button battery ingestions: A review of 56 cases. JAMA 249(18): 2495-2500.
-
Lue A (2001) Esophageal perforation. BCM 10: 123-
-
Vaishnav A, Spitz L (1989) Alkaline battery-induced tracheo-oesophageal fistula. Br J Surg 76(10): 1045.
-
Sigalet D, Lees G (1988) Tracheoesophageal fistula secondary to disk battery ingestion. J Pediatr Surg 23(11): 996-998.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?