SNHL of Childhood New Diagnostic Criteria. An Upgraded Clinical Approach to a ‘Failed’ BERA Test
Medical literature is replete with articles about the benefits of BERA, not merely as an auditory test, but also an aid for evaluating the CNS function represented by the brainstem activity in several clinical conditions, such as in comatose patients, bipolar disorders, attention deficit disorder, synapse dysfunctions and hydrocephalus. Irreversible sensorineural hearing loss (SNHL) in infants, identified by a failed BERA, in addition to its being one of major clinical features of intrinsic ear diseases, is also a sign of inborn disorders of white matter. Thus, a new dimension is attached unto the benefits of a failed-BERA. We will high lighten the way towards identifying the exact etiology of irreversible SNHL of non-intrinsicear-disease, in condition that other clinical features appear in conjunction with SNHL. To achieve this, we reviewed all the diseases, syndromes and triads, at which a failed-BERA is one of their major components of the clinical picture. We brought here a case report of an infant suffering from SNHL. Irreversible SNHL in childhood is one of the major features in certain neurologic disorders, but not necessarily the first to appear. It is a main marker for the diagnosis of Leukodystrophies, as well as Multiple Sclerosis. Otolaryngologists and clinicians in general should be conscious while following-up certain infants who have irreversible SNHL of non-intrinsic-ear-disease. The appearance of pendular nystagmus, truncal hypotonia, or intentional tremor with a staccato speech, in parallel with hyperreflexia, and spastic paraplegia is the core of our upgraded flow chart of SNHL clinical approach.
Nadim H Nasser*, Mohammad M Simri and Nadir N Nasir
Ilan & Clalit Health Organization, Tarshiha and Bokea’a Clinic, Israel, Tel:
+97249979129; Email: nasser_nadim9@hotmail.com
spastic paraplegia is the core of our upgraded flow chart of SNHL clinical approach.
Evoked Response Audiometry (equivalent to ABR); CERA: Cortical Evoked Response Audiometry; CNS: Central Nervous System; MS: Multiple Sclerosis; OAE: Oto Acoustic Emissions; SNHL: Sensory-Neural Hearing Loss;
SHL: Sensory Hearing Loss; PMLD: Paliazeus-Mertbacher- Like Disease.
Introduction
The medical literature, after 1962, is replete with articles about the diagnostic uses of the brainstem evoked response audiometry [BERA] electroencephalogram. The health problems currently investigated by BERA include, mainly, the detection of sensorineural hearing loss (SNHL), evaluating comatose patients, bipolar disorders as schizophrenia, attention deficits hyperactivity disorders, in addition to localization of occult areas of neuronal and synapse dysfunctions, which clinicians cannot disclose through clinical assessment [1, 2].
It is notable, by the way, that clinicians had abandoned the use of BERA for detection of acoustic tumors, because it is a false negative test for smaller than 1-centimeter masses. The pathology of SNHL may be located in the sensory organ, namely the cochlea, and/or the auditory nerve and the other auditory structures in the CNS, namely the neural retro-cochlear organs. Historically, it was difficult to differentiate between those sites-of-lesion in the sensory and neural systems because they are closely linked one to the other. The Mondini cochlear dysplasia, in one hand, which is a rare, but a treatable disease, and the cochlear dysplasia of Pendred syndrome, which leads to sensory hearing loss (SHL), in the other hand, are not the subject of this manuscript [1, 3, 4, 5].
The previous classifications for SNHL, so far, did not cover the whole of the existing causes, and yet failed to specify certain etiologies [6]. Recently, however, the ‘failed’ BERA had become one of the exclusive clinical features that manifest at bedside, in specific brain disorders, beyond the list of disorders mentioned in preceding researches [2, 7].
The genetic neuro-degenerative syndromes of gray and white matters constitute nearly 4-percent of all the known etiologies of SNHL. If we calculate the number of patients worldwide, then, it becomes a large number of such neural-deaf children [1, 3, 5, 6, 8, 9, 10, 11, 12, 13].
It is the clinicians’ duty to disclose the type and configuration of hearing loss, as a primary information required to determine further test procedures and to direct medical and/or audiological investigations and interventions. The identification of SNHL, in an infant, is a good catalyst to detect neuro-degenerative disorders. The upper motor neuron degeneration disorders, such as Tay- Sachs, cerebral and cerebellar cortical disease, (as opposite to the white matter disorders), are easy to diagnose at bedside. A large head circumference, early-in- life convulsion, deteriorating mental functions through infancy, and, in some cases, a macular cherry red spot in retinas; when conjoined together, they point to the gray matter upper neuron disorders.
In other hand, the white matter diseases, mainly, the cerebral myelin injuries are hard to diagnose, while the SNHL is the only clinical feature that manifestated. What we mean is that there is no single pathognomonic sign to point to white matter disease. However, we had a group of thirteen infants, homozygous to newly discovered mutation of Mitchap-60 leukodystrophy, which is actually, a Paliazeus-Mertbacher-like disease (PMLD). At this type of white matter disease, the SNHL had shown up, in combination with other major clinical features, in all of the patients. A triad of major clinical features, springing from myelin defect in three organs in the brain at same patients and in all the other known leukodystrophies: a) A 'failed' BERA (SNHL), b) Horizontal nystagmus, and c) Hypotonia of the axial muscles, we published in 2012 [8, 14] (Figure 1).
Well, upgrading protocols for the diagnosis of SNHL is a clinical interest. It is through this manuscript, that we expose a ‘new dimension’ to the list of health problems currently investigated by BERA.
Materials & Methods
We reviewed the relevant medical literature, concerning genetic SNHL, aiming to identify all the diseases, syndromes and triads, at which the congenital SNHL is one of the main clinical characteristics Table 1. We selected a case report, which represents the group of infants who suffered from the same leukodystrophy mutation, named as D29G Hsp60 chaperonopathy [15, 16]. Our aim is highlighting the policy of “wait” in a certain infant who suffers from sensorineural deafness, and “see” if other accompanying major clinical features will appear.
Results
BERA test is a good tool to point out the level of damage in brain. The combination of a failed BERA with abnormal eye movements and axial hypotonia, staccato speech and tremor is a clinical pointer to three anatomic structures of the brain, where the defects had struck, that is, a key to early diagnosis of diseases of leukodystrophies and MS [2, 7, 17, 18, 19, 20]. Table 1 details syndromes and triads, at which SNHL is one of their major features:
| Incidence of | Signs of Upper | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Syndrome or Triad | Incidence of Nystagmus & Other Signs | ||||||||||
| SNHL | Neuron Disorders | ||||||||||
| Charcot’s triad (Childhood) | High | High | + | ||||||||
| Peliazeus-Mertzbacher disease | // | // | + | ||||||||
| Peliazeus-Mertzbacher-like diseases [Mitchap-60 disease] | // | // | + | ||||||||
| Metachromatic leukodystrophy | // | // | + | ||||||||
| Refsum disease | // | // | + | ||||||||
| Zellweger disease | // | // | + | ||||||||
| Alexander disease | // | // | + | ||||||||
| Canavan disease | // | // | + | ||||||||
| Krabbe' disease | // | // | + | ||||||||
| Vanishing white matter | // | // | + | ||||||||
| Aircadi-Goutie'res syndrome | // | // | + | ||||||||
| “Mais-Nadim Nasser Triad” (Childhood) | // | Primary hypotonia, nystagmus, abnormal BERA test | + | ||||||||
| Fechtner's syndrome (Childhood) | Low | Nephritis, SNHL, eye abnormalities | unknown | ||||||||
| Congenital rubella retinopathy (Childhood) | Low | Cataracts, deafness, congenital heart disease | unknown |
Table 1: The syndromes in pediatric-Otolaryngology, with high/low incidence of sensorineural deafness (SNHL). SNHL is a major sig
B.O. was adequate for birth weight. A term newborn, with Apgar score of 9/10. The screening ABR failed, but Oto-acoustic emissions (OAE) passed. B.O.’s parents were descendants of a tribe, which had a high frequency of consanguineous marriages, and consequently an exceeding percentage of genetic diseases. The known inborn disorders are SNHL, thalassemia, sickle cell anemia, Pendred and Mondini syndromes, all in same family. At the infant's first–time visit to our clinic, at 2- months-age, parents were anxious about the baby's movements, and were worried that something was wrong with his hearing. Physical examination, at the time, had excluded dysmorphism. We noticed truncal hypotonia which manifested by a swinging head and a head lag. Several weeks later, we noticed uncontrolled pendular eye movements. Social smile was absent. The neurologist noted that the baby had a hypotensive frontal fontanelle, slight spastic paraplegia, and tendon hyperactive reflexes. Later, at 6-months old, the AC& BC BERA tests had failed at 70-decibels thresholds. OAE and tympanometry were normal. His parents refused to carry out a brain MRI. The hypotonia of back and neck muscles, the pendular nystagmus, and the failed result of BERA, are a triad of features, which, in addition to signs depicted by the neurologist, have diverted our attention to a central dysfunction of the myelin of the white matter. That happened a long time before the genetic tests had revealed the Hsp60 Chaperonopathy mutation, which is
Discussion & Conclusions
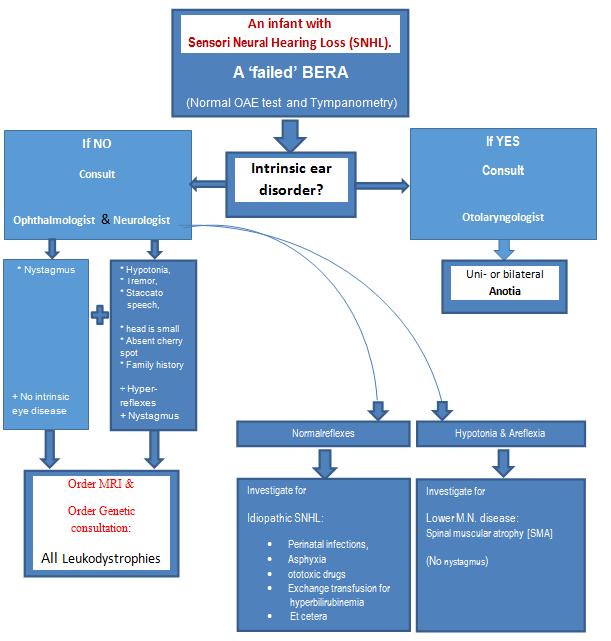
It is through this manuscript, that we expose a ‘new dimension’ to the list of health problems currently investigated by BERA. That is, in addition to its importance as an auditory test, BERA is also a neurologic marker to evaluate possible injuries at the level of brainstem, which is one organ among white matter organs in human. In retrospect, the triad of markers, including SNHL, hypotonia of back and neck, and pendular eye movements, is pathognomonic for all the inborn and congenital disorders of central white matte, named as leukodystrophies. This paper highlights the feasibility of bedside clinical diagnosing of one of the rare etiologies of irreversible SNHL in the presence of other major markers [1, 14]. The next novel flowchart is an applicable diagram, for clinical identification of rare etiologies of SNHL, including those that did not appear in previous classifications of SNHL. Please note that the starting point in the flowchart is ‘An infant with SNHL’, and the end- result is leukodystrophy. However, it is quite possible that at the end of the diagram we will reach to a different etiology, depending on the family history in combination with symptoms and signs the patient has.
Axial hypotonia, which is accompanied by pendula nystagmus and SNHL consist a triad for diagnosis of LD, where the failed BERA bone conductance test is the pointer to the level at which the injury occurred in the brain. (U.M.N. = upper motor neuron, L.M.N. = lower motor neuron disease, LD=leukodystrophy or white matter disease. AC & BC BERA = Air-conductance & Bone- conductance BERA) Nadim H Nasser, September 2015.
Pediatricians advise to re-examine every discharged infant from neonatal intensive care units, by BERA, at one- year of age and 3-years, as a step to early discover SNHL [11], and investigate other possible etiologies, such as myelin disorders of the CNS. In certain neurological diseases, SNHL is infrequently the sole manifestation, but it might be one feature among other clinical signs, which could precede the neural deafness. Therefore, the previous classifications of irreversible SNHL, which do not take into account the entire spectrum of neurological diseases, need further upgrading, exploiting other accompanying clinical features, namely, axial hypotonia with spastic paraplegia and hyperreflexia, pendular nystagmus, intention tremor, staccato speech and other minor signs [9].
Conclusively, our perspective concerning a failed BERA test, namely, SNHL in infants, is that it should always alert the otolaryngologist for the possibility of occult but serious diseases of CNS, particularly, white matter disorders. The more so when part of the features of myoclonus, ataxia, truncal hypotonia, pendular nystagmus, interrupted staccato speech, intention tremor, and a familial history of brain disorders, exist [21, 22, 23, 24]. We advise to employ those accompanying features within the flow charts of the differential diagnosis of SNHL Figure 1. When the combination of signs is clear-cut, it soon becomes a very sensitive and highly specific combination of characteristics, which directs us to defects of white matter of the CNS.
It is important to diagnose degenerative brain disorders as the etiology of irreversible infantile SNHL, because this group of axonal disease have yet a very bad prognosis, and no cure. Most annoying questions from parents of children, who suffer from those incurable diseases, are those that begged for whatever medication to cure their child, when the SNHL per se becomes a marginal matter compared to them, at a time their child is on his deathbed. Physicians usually attempt to reassure parents that their sick baby will have his meals through a gastric tube, vaccinated against viral and bacterial diseases, and treated for every infection by the appropriate medicines, etcetera. Those answers, though necessary, might be much more annoying for them than to just say: ”No, we have nothing to do”. It was pleasant, however, to hear that there is certainly a glimmer of hope in the clinical trials currently underway, with promising results of enhancing complete re-myelination and recovery of previously demyelinated fibers in lab animals with MS. The contribution of such research, as an appropriate medication for those dying patients is great, especially when we start such therapy as soon as possible.
Summary
SNHL could be a preliminary feature of CNS disorders. The implication of this statement is our advice to rule out CNS disorders, by taking the following steps: a) Evaluating every infant with motor delays by a BERA test. b) Evaluating every infant with pendular nystagmus by a BERA test. c) Evaluating every infant with motor delays and pendular nystagmus by a BERA test. d) Evaluating every infant with pendular nystagmus for the sake of detectinghypotonia and SNHL. e) Evaluate every infant with staccato speech or intension tremor by a BERA test. f) Evaluate every infant with hypotonia by a BERA test.
Acknowledgement/Disclosure
Thanks to Ms. Hanadi Nasser, a Medical student of the Szeged University, Hungary, for her endeavour and generous contribution for preparing the flowchart and table for this ‘SNHL of Childhood New Diagnostic Criteria; An Upgraded Clinical Approach to a ‘Failed’ BERA Test’ article. No funding, no grants & No Disclosures. Authors Agreement: We authors of this manuscript state that we are in agreement with the content of the manuscript. In addition, we state here that there were no funding sources, financial conflicts, or any potential conflict of interest.
References
-
Overell J, Lindahl A (2004) Neuro-otological syndromes for the neurologist. J Neurol Neurosurg Psychiatry 75(4): 53-59.
-
Gunther E (2015) Auditory Brainstem Response as a Diagnostic Tool for Patients Suffering From Schizophrenia, Attention Deficit Hyperactivity Disorder, and Bipolar Disorder: Protocol. JMIR Res Protoc 4(1): 16.
-
Alves de Sousa LC, Rodrigues Lda S, Piza MR, Ferreira DR, Ruiz DB (2007) Occasional finding of neurological disorders during children hearing loss evaluation using the ABR. Rev Bras Otorrinolaringol 73(3): 424- 428.
-
Renée Punch L (2009) Incidence, Prevalence, and aetiology of Childhood Hearing loss. Victorian deaf education institute.
-
Walch C, Anderhuber W, Köle W, Berghold A (2000) Bilateral sensorineural hearing disorders in children: etiology of deafness and evaluation of hearing tests. Int J Pediatr Otorhinolaryngol 53(1): 31-38.
-
Poliana L, da Silva A, Quiroz F, Lima I (2006) Etiology of Hearing Impairment in Children and Adolescents of a Reference Center APADA in the city of Salvador, state of Bahia. Brazilian Journal of Otorhinolaryngology 72(1): 33-36.
-
Nasser N (2014) “Mais –Nasser Nadim Triad”, a useful marker for Leukodystrophies diagnosis. J Genet Syndr & Gene Ther 5: 5.
-
Ochs R, Markand ON, Demyer WE (1979) Brainstem auditory evoked Responses in leukodystrophies. Neurology 29(8): 1089-1093.
-
Nasser HN (2015) New Diagnostic Criteria for Infantile Nystagmus. Int J Ophthalmol Clin Res 2: 4.
-
Morlet T, Nagao K, Bean SC, Mora SE, Hopkins SE, et al. (2018) Auditory function in Pelizaeus-Merzbacher disease. J Neurol 265(7): 1580-1589.
-
Kohlschütter A, Eichler F (2011) Childhood leukodystrophies: a clinical perspective. Expert Rev Neurother 11(10): 1485-1496.
-
Coticchia JM, Roeder MAD, Zuliani GF, Alexander Gow, James Y Garbern (2011) Auditory testing profiles of Pelizaeus-Mertzbacher disease. Int J Pediatr Orothinolaryngol Extra 6(1): 23-29.
-
Sanyelbhaa H, Kabel A, Abo-El-Naga HAE, Sanyelbhaa A, Salem H (2017) The risk ratio for development of hereditary sensorineural hearing loss in consanguineous marriage offspring. Int J Pediatr Otorhinolaryngol 101: 7- 10.
-
Antonio SAM, Meyers AD (2016) Syndromic Sensorineural Hearing Loss. Department of Otolaryngology Head and Neck Surgery, Eastern Virginia Medical School. Medscape.
-
Roberts A, MrGibbin K (2008) Ministry of Defense. Synopsis of Causation Sensorineural Hearing University Hospital, Queen’s Medical Centre, Nottingham.
-
Schwartz RA, Rohena LO (2015) Genetics of Waardenburg Syndrome. Medscape.
-
Rogowski M, Michalska BI (2001) The importance of brain stem evoked potentials in the diagnosis of neurosurgical patients. Neurol Neurochir Pol 35(4): 667-679.
-
Zhou G, Dornan B, Hinchion W (2012) Clinical Experience of Auditory Brainstem Response Testing on Pediatric Patients in the Operating Room. Int J Otolaryngol 2012: 350437.
-
Evoked potential studies (2006) Comprehensive auditory evoked response testing and comprehensive Otoacoustic (AEPs), brainstem auditory evoked potentials (BAEP), BERA, BSER, and BSRA. Metachromatic leukodystrophy, Pelizaeus- Merzbacher disease.
-
Fortnum HM, Summerfield AQ, Marshall DH, Bamford JM (2001) Prevalence of permanent childhood hearing impairment in the United Kingdom and implications for universal neonatal hearing screening: questionnaire based ascertainment study. BMJ 8(323): 536-540.
-
Moktar ECM, Riahi Z, Hachmi HL, Veten F, Meiloud G, et al. (2016) Etiology and associated GJB2 mutations in Mauritanian children with non-syndromic hearing loss. Eur Arch Otorhinolaryngology 273(11): 3693- 3698.
-
Ching TY, Oong R, Van Wanrooy E (2006) The ages of intervention in regions with and without universal newborn hearing screening and prevalence of childhood hearing impairment in Australia. Australian and New Zealand Journal of Audiology 28(2): 137-150.
-
Davidson J, Hyde ML, Alberti PW (1989) Epidemiologic patterns in childhood hearing loss: a review. Int J Pediatr Otorhinolaryngol 17(3): 239- 266.
-
Open access guide to audiology & hearing aids for otolaryngologists. Swanepoel & Claude Laurent. pp: 1-4. http://www.entdev.uct.ac.za
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?