Anatomy of the IV Ventricle Applied to the Auditory Brainstem Implant (ABI)
Introduction: Hearing loss in its different degrees is widely recognized as one of the most common disabilities of humanity, it affects approximately 100 million people around the world, only in the United States there are more than 28 million1 Americans who suffer from it and it is expected These figures will increase significantly in the coming decades. The first Auditory Brainstem Implant (ABI) was developed in 1979 at the House Ear Institute in the United States by Dr. William House and Dr. William Hitselberger. The intricate anatomy of the IV ventricle is of great importance in ABI surgery. The IV ventricle in an ependymal cavity of the rhombencephalon, limited anteriorly by the brainstem and posteriorly by the cerebellum, in terms of its structure it can be divided into a roof, floor and two lateral recesses, it continues towards the cephalad with the cerebral aqueduct and caudally with the central medullary canal. Objective: To value the complex anatomy of the fourth ventricle Materials And Methods: A descriptive observational study was carried out in the chair of Normal Anatomy and Imaging Dr. Luis Dellepiane, from the Universidad del Salvador, CABA. During the months of August and September 2022. 6 cerebellums with brain stem and 3 formolized heads were used. Results: The fourth ventricle is a cavity that lies dorsal to the brainstem, ventral to the cerebellum, and medial to the cerebral peduncles. A floor and a roof are described as limits, in addition to two extensions called lateral recesses. The arrangement of these can be seen when performing a sagittal cut where the fourth ventricle shows the shape of a tent, with the floor being the base with a vental orientation, and the walls the roof with a dorsal orientation. Conclusions: The anatomical knowledge of the complex structure of the fourth ventricle is of vital importance in ABI surgery, it is necessary that the neurosurgeon and the otolaryngologist know the above for a better understanding of its intricate anatomy.
Introduction
Hearing loss in its different degrees is widely recognized as one of the most common disabilities of humanity, affecting approximately 100 million people around the world. In the United States there are more than 28 million [1]. Americans who suffer from it and it is expected that these numbers will increase significantly over the next few decades.
Its treatment depends on the degree and type of hearing loss. Cases of profound or severe sensorineural hearing loss due to a cochlear defect with an intact auditory nerve could be candidates for a cochlear implant, but those patients with an absence of the cochlea or cochlear nerve, auditory rehabilitation is possible with the insertion of an Auditory Brainstem Implant (ABI) [2].
The first ABI was developed in 1979 at the House Ear Institute in the United States by Dr. William House and Dr. William Hitselberger. The design of the electrodes has been changing since the first attempts to electrically stimulate the cochlear nuclei and consequently the results have improved and a greater stabilization of the device has been achieved.
The ABI is a device that provides sound perception through electrodes surgically implanted in the cochlear nuclei of the brainstem, directly stimulating the brainstem neurons by bypassing the cochlea and cochlear nerve.
Structurally, the ABI is similar to a cochlear implant. It has a series of internal devices that are placed during surgery: receiver coil, decoder and electrodes, and external devices: transmitter coil, speech processor and microphone.
The electrodes and their arrangement deserve special mention since, unlike the cochlear implant, the ABI has a silicone electrode holder (3 x 8.5 mm) with 21 platinum electrodes arranged in 3 rows (electrode diameter 0.7 mm), a Dacron device that stabilizes the electrodes by allowing the growth of connective tissue from the brainstem around it [3].
The sound is received by the external microphone located behind the auricle, this signal is transmitted to the language processor which transforms it into a digital stimulus that is transmitted to the internal processor and from it through the electrodes to the cochlear nuclei.
In general terms the ABI is indicated in those patients with absence or alterations in the cochlear nerve or cochlea. Historically, the patients most frequently selected for this type of implant were those with neurofibromatosis type 2, but with the development of medical engineering, the indications for ABI have been extended [4].
The IV ventricle in an ependymal cavity of the rhombencephalon, limited anteriorly by the brainstem and posteriorly by the cerebellum, in terms of its structure it can be divided into a roof, floor and two lateral recesses, it continues towards the cephalad with the cerebral aqueduct and caudally with the central medullary canal. The objective of this manuscript is to carry out an anatomical description of the IV ventricle applied to the ABI.
Objective
Value the complex anatomy of the fourth ventricle.
Materials and Methods
An observational descriptive study was carried out in the chair of Normal Anatomy and Imaging Dr. Luis Dellepiane, from the Universidad del Salvador, Buenos Aires, Argentina, during the months of August and September 2022.
6 cerebellums with brainstem and 3 formalized heads were used. To obtain images, a Nikon Kit D5600 camera was used.
Results
Regarding the human cadaveric material, the pertinent dissections were performed in the 6 cerebellums with brainstem and the 3 heads, all 10% formalized preparations. The dissection was systematized in 1- recognition activity of the anatomy of the region 2- description of the roof, floor, lateral recesses and vascular relations of the 4th ventricle.
Anatomical Review
The fourth ventricle is a cavity that lies dorsal to the brainstem, ventral to the cerebellum, and medial to the cerebral peduncles. It is continuous with the rest of the ventricular system through the cerebral aqueduct, located rostrally and communicated with the third ventricle, and opens caudally to the central medullary canal. In addition, it communicates with the subarachnoid space, laterally through Luschka’s foramina, continuous with the cerebellopontine cisterns, and with the cisterna magna through Magendie’s foramen.
A floor and a roof are described as limits, in addition to two extensions called lateral recesses. The arrangement of these can be seen when performing a sagittal cut where the fourth ventricle shows the shape of a tent.
Roof of the IV ventricle: It is formed by two portions, one superior and one inferior, which meet at a common point, the fastigium. The upper roof is formed, laterally, by the ventricular surfaces of the superior and inferior cerebellar peduncles, and towards the midline by the superior medullary velum, a thin layer of white matter lying between the superior cerebellar peduncles and the lingula of the vermis, also fixed to the posterior face of the midbrain by the frenulum of the
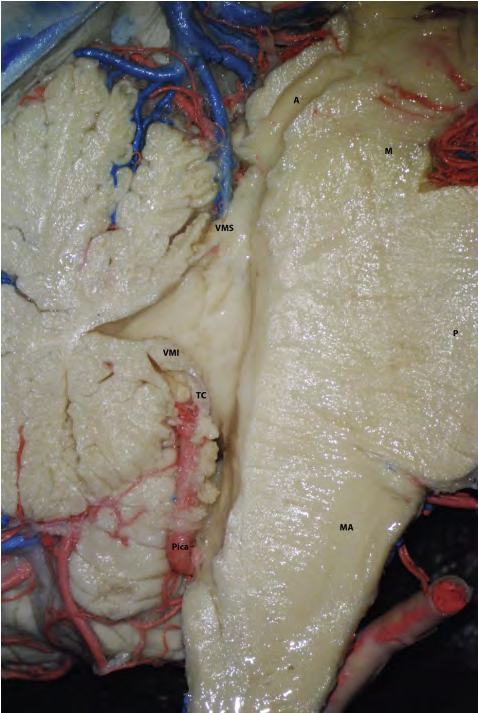
superior medullary velum. The inferior roof is formed by the nodule of the vermis, the inferior medullary velum, and the tela choroidea. The latter is a thin layer of connective tissue and ependymal cells from which the choroid plexuses originate and are fixed, both being arranged in the shape of an inverted “L” so that they are not only located on the lower roof but also cover the lateral recesses (Figures 1-4).
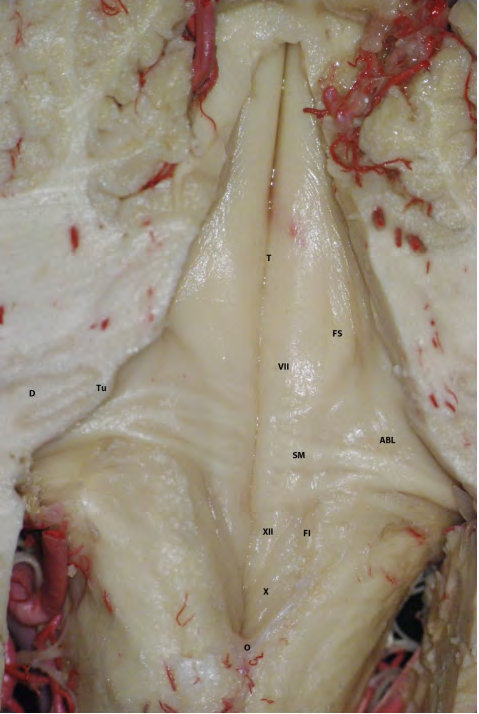

Floor of the IV ventricle: Corresponds to the posterior face of the pons and bulb, due to its shape it is also known as rhomboid fossa, with the upper end of the fossa continuous with the cerebral aqueduct and the lower one corresponding to the obex. Transversely, it is divided into three portions: a pontine, triangular in shape, whose base is an imaginary line that joins the lower margin of the cerebellar peduncles; a medullary, inverted triangular in shape, whose base is the taenia of the lower part of the lateral recess where the tela choroidea is fixed; and an intermediate one, in the form of a band, arranged between the first two. It is divided longitudinally by two vertical grooves: the median groove, arranged in the midline, and the sulcus limitans, which divide the two halves of the floor of the fourth ventricle into the median eminence and the vestibular area. The first one describes, from rostral to caudal, the facial colliculus, a protrusion caused by the presence of the abducens nucleus being surrounded by fibers of the facial nerve; and three triangular areas: the hypoglossal trigone, the vagus trigone, and the area postrema. In the vestibular area there are: the stria medullaris and the auditory tubercle [5].
In addition, two depressions are described in the sulcus limitans, the superior and inferior fovea (Figure 5 & 6).


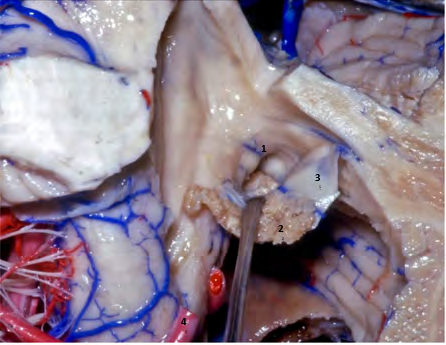
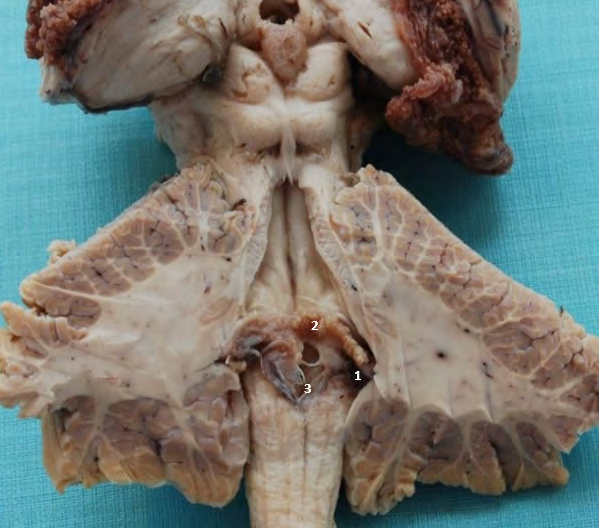
Lateral recesses: correspond to two extensions that continue the fourth ventricle to its opening in the cerebellopontine cisterns through the foramina of Luschka. Two portions are described: a peduncular, rostrally oriented, formed by the caudal margin of the inferior cerebellar peduncle, and a cisternal, ventrally oriented, formed by the rhomboid lip, a layer of white matter that is located at the level of Luschka’s foramen. . The entire floor of the lateral recesses, oriented caudally, is upholstered by tela choroidea.
Rhomboid lip: it is a sheet of white matter that forms the ventral limit of the foramen of Luschka [6, 7, 8].
The apparent origin of the pairs IX and X are located towards the dorsal side of the latter and that of the pairs VII and VIII towards the rostral side. The first segments of the AICA are also related to this structure.
The choroid plexus is an important point of reference since, being fixed to the tela choroidea that forms the floor of the lateral recess, it reaches Luschka’s foramen and in most cases protrudes through it on the opposite side of the rhomboid lip.
Vascular relationships: Each limit of the fourth ventricle is in close relationship with each of the fissures described between the cerebellum and the brainstem. The superior cerebellar artery courses in relation to the cerebello- mesencephalic fissure and the superior roof of the fourth ventricle. The anterior inferior cerebellar artery (AICA) is related to the lateral recess and Luschka’s foramen, especially in its lateral pontine and flocculo-peduncular segment on its way through the cerebellopontine fissure. Finally, the posteroinferior cerebellar artery (PICA) in its course through the cerebellomedullary fissure is related to the inferior roof of the fourth ventricle, especially the tonsillomedullary and telovelotonsillar segments [9, 10].
Discussion
Regarding the anatomy of the IV ventricle in the works published by Matsushima, Mercier and Longatti, there is a coincidence in the cadaveric anatomical description of the same with that made by the authors of this work [11, 12, 13]. In a regulated manner, all systematically describe the fourth ventricle as a dilation of the ependymal canal, conical in shape, located posterior to the brain stem and anterior to the cerebellum.
Its representation is organized into a superior or pontine portion, an intermediate or bulbo-protuberant portion, and a lower or bulbar portion. According to the study carried out by Antar in 2019, the IV ventricle has a mean length of 54.3 ±3.67 mm and a distance between Luschka’s foramina of 22.51 ±2.43 mm. Structurally, it is divided into a roof for better understanding, made up of the upper and lower medullary velum, cerebellar peduncles and tela choroidea. A floor furrowed by 2 lines, posterior longitudinal sulcus and sulcus limitans, separated by a distance of 5.51 ± 0.88 mm [14]. These grooves delimit 2 areas: vestibular to lateral and median to medial eminence, the latter presenting as relevant accidents from cephalic to caudal: locus coeruleus, facial colliculus, hypoglossal trigone and vagus trigone. (eleven).
The cochlear nuclei, of great importance in ABI implantation, are located lateral to the sulcus limitans and are divided into two parts: the dorsal cochlear nucleus and the ventral cochlear nucleus. As a whole, they have an extension from the floor of the IV ventricle to the root of the vestibulocochlear nerve of 1.28 cm [15]. Functionally, these nuclei divide tonotopically, with the dorsal cochlear nucleus receiving the highest frequencies and the ventral cochlear nucleus receiving the lowest frequencies [16].
The dorsal cochlear nucleus is located in the floor of the lateral recess, at the rostral margin of Luschka’s foramen and is related to the posterior region of the inferior cerebellar peduncle. It is located lateral to the vestibular and caudolateral area of the facial colliculus [6]. Macroscopically, this nucleus is represented by a prominence located on the floor of the fourth ventricle, the auditory tubercle [15]. This structure is located approximately 67 mm from the posterior longitudinal groove [17] and 49 mm from the sulcus limitans6. It has a medial - lateral extension of 55mm to the right and 50mm to the left and a rostro - caudal extension of 21mm on the right side and 22mm on the left side [17].
On the other hand, the ventral cochlear nucleus is located directly at the junction between the vestibulocochlear nerve and the brainstem, on the lateral margin of the dorsal cochlear nucleus [6]. Topographically it is located at the junction between the lateral recess and the cerebellopontine angle and is related to the flocculus [18]. Unlike the dorsal cochlear nucleus, it does not produce a bulge on the surface of the brain stem, but lies deep within the pons, above the medulla pontine sulcus6. According to the study carried out by Terr and Edgerton [19], the ventral cochlear nucleus is partially located within the Luschka foramen.
Medial to the sulcus limitans, in the already mentioned median eminence is the facial colliculus. This structure, located at the bulbo-pontine level, is the most prominent on the surface of the fourth ventricle and is formed by the nucleus of the abducens nerve and the ascending segment of the facial nerve [6]. Motor fibers leave the facial nerve nucleus located ventrolateral to the abducens nerve nucleus and lie medially to it. The facial colliculus is located 0.6 mm from the posterior median sulcus and has measurements of 6.8 mm in the craniocaudal direction and 5.7 mm in the mediolateral direction [20]. Cranial to the facial colliculus at the median eminence is the loecus coeruleus. Located in the dorsolateral region of the pons, it is part of the ascending reticular activation system and exerts its function predominantly through the release of norepinephrine [21].
The lateral recesses are tunnel-like structures that extend lateral to the pontomedullary junction. Its length is from 10.4 to 24.3 mm with an average of 8.5 mm, and a width of 2.8 to 6.5 mm with an average of 4.mm [22]. The study of the morphology of these structures dates back to the end of the 19th century, where attempts were already being made to clarify the limits and meaning of its components from both morphological and embryological approaches [23]. With the advent of microsurgery, interest in this region has increased [24, 25, 26] but even so there are controversies in its anatomy. Most agree that the rostral wall is formed by the caudal margin of the cerebellar peduncles, the peduncle of the flocculus, and the flocculus, and that the ventral wall is formed by the rhomboid lip and the lateral part of the floor of the fourth ventricle containing the cochlear nuclei [22, 27]. But, on the other hand, regarding the caudal wall, while some maintain that it is formed by extension of tela choroidea [27], others include the rhomboid lip, evidencing that this last structure is not yet clearly defined in the literature [22].
At the topographic level, the lateral recesses have an intraventricular and an intracisternal portion, divided by the origin of the rhomboid lip. This conception, introduced in recent years, makes it easier to locate the cochlear nuclei since the fixing edge of the lip extends over the ventral cochlear nucleus9 22.
Considering the situation of the lip with respect to Luschka’s foramen, the retraction of the choroid plexus allows visualization together with the interior of the lateral recess, immediately behind the lip is the intraventricular portion of the ventral cochlear nucleus and then the ventral
Luschka’s foramen is located at the end of the lateral recess and communicates the fourth ventricle with the pontocerebellar cistern. Regarding its relationship with the neighboring cranial nerves, it is located towards the anteroinferior of the accessory and hypoglossal nerves, posteroinferior of the facial and vestibulocochlear nerves, and dorsal to the glossopharyngeal and vagus nerves [29], with the latter the profusion of the choroid plexus of the fourth ventricle, named historically as the Bockdalek flower basket after the Czech anatomist who first described it [30]. The arterial relationships are more variable: the PICA runs below the foramen, in relation to the glossopharyngeal and vagus [29]; the AICA runs caudally and can send branches through the foramen [31], being duplicated and tripled in 26% and 2% of cases respectively, as well as being variably related through its branches with the vestibulocochlear complex [32]. This last relationship is important to avoid serious sequelae in this type of surgery [33]. Lastly, the initial portion of the vein of the middle cerebellar peduncle and that of the cerebellomedullary fissure are those with the most relevant relationship with Luschka’s foramen [34].
dorsal nucleus. (6 18 19) The latter is located in the upper portion of the floor of the lateral recess and is visualized thanks to the fact that it forms a prominence, the auditory tubercle10 15 (Figure 7). Another important consideration of the rhomboid lip was described by Y. Nakahara, who reported the possibility of an enlarged presentation of this that covers the exit of the cranial nerves adjacent to the Luschka foramen with the possibility of confusing it with arachnoids; this variation would coexist with a foramen Luschka’s also enlarged. Likewise, he reported the possibility of detecting this variation using conventional magnetic resonance imaging [28].
Conclusions
Anatomical knowledge of the complex structure of the fourth ventricle is important in ABI surgery and it is necessary for both neurosurgeon and otorhinolaryngologist. In this manuscript a limited description of the IV ventricle is made, pointing out relevant structures in ABI surgery so that the general otolaryngologist has access to a simplified representation of its intricate anatomy.
References
-
Dhanasingh A, Hochmair I (2021) ABI-auditory brainstem implant. Acta Otolaryngol 141(S1): 63-81.
-
Colletti V, Carner M, Miorelli V, Guida M, Colletti L, et al. (2005) Auditory brainstem implant (ABI): new frontiers in adults and children. Otolaryngol Head Neck Surg 133(1): 126-38.
-
Colletti L (2007) Beneficial auditory and cognitive effects of auditory brainstem implantation in children. Acta Otolaryngol 127(9): 943-946.
-
Diamante V, Pallares N (2011) Brainstem auditory implantation in four children with cochlear nerve aplasia. REVISTA FASO AÑO 18 - Nº 5 – 2011 pp: 42-44.
-
Komune N, Yagmurlu K, Matsuo S, Miki K, Abe H, et al. (2015) Auditory brainstem implantation: anatomy and approaches. Neurosurgery 11(S2): 306-320.
-
Abe H, Rhoton AL (2006) Microsurgical anatomy of the cochlear nuclei. Neurosurgery 58(4): 728-739.
-
Kuroki A, Møller AR (1995) Microsurgical anatomy around the foramen of Luschka in relation to intraoperative recording of auditory evoked potentials from the cochlear nuclei. J Neurosurg 82(6): 933-939.
-
Vautrin R, Mertens P, Streichenberger N, Ceruse P, Truy E (1998) Oto-neuro-surgical approach and accessibility to the cochlear nuclei. Significance in auditory brain stem implant. Rev Laryngol Otol Rhinol (Bord) 119(3): 171- 176.
-
Terr Ll, Fayad J, Hitselberger WE, Zakhary R (1990) Cochlear nucleus anatomy related to central electro auditory prosthesis implantation. Otolaryngol Head and Neck Surg 102(6): 717-721.
-
Matsushima K, Peris-Cell M (2022) Cerebellum and brainstem. In: Rhoton A, Peris-Cell M, et al. (Eds.), Rhoton-Atlas of head,neck and brain. Amolca pp: 384- 394.
-
Matsushima T, Rhoton AL, Lenkey C (1982) Microsurgery of the fourth ventricle: Part 1. Microsurgical anatomy. Neurosurgery 11(5): 631-667.
-
Mercier P, Bernard F, Delion M (2021) Microsurgical anatomy of the fourth ventricle. Neurochirurgie 67(1): 14-22.
-
Longatti P, Fiorindi A, Feletti A, D’Avella D, Martinuzzi A (2008) Endoscopic anatomy of the fourth ventricle. J Neurosurg 109(3): 530-535.
-
Antar V, Turk O, Katar S, Ozden M, Sahin B et al. (2019) Morphometric Assesment of the External Anatomy of Fourth Ventricle and Dorsal Brainstem in Fresh Cadavers. Turk Neurosurg 29(3): 445-450.
-
Quester R, Schröder R, Klug N (2004) Optimization of microsurgical operation technique to insert auditory brainstem implants, taking into account the results of a morphometric study. HNO 52(8): 706-13.
-
Biacabe B, Chevallier JM, Avan P, Bonfils P (2001) Functional anatomy of auditory brainstem nuclei: application to the anatomical basis of brainstem auditory evoked potentials. Auris Nasus Larynx 28(1): 85-94.
-
Quester R, Schröder R (1999) Topographic anatomy of the cochlear nuclear region at the floor of the fourth ventricle in humans. J Neurosurg 91(3): 466-476.
-
Dublin WB (1982) The cochlear nuclei revisited. Otolaryngol Head Neck Surg 90(6): 744-760.
-
Terr LI, Edgerton BJ (1985) Three-dimensional reconstruction of the cochlear nuclear complex in humans. Arch Otolaryngol 111(8): 495-501.
-
Yang SH, Park H, Yoo DS, Joo W, Rhoton A (2021) Microsurgical anatomy of the facial nerve. Clin Anat 34(1): 90-102.
-
Ferrucci M, Giorgi FS, Bartalucci A, Busceti CL, Fornai F (2013) The effects of locus coeruleus and norepinephrine in methamphetamine toxicity. Curr Neuropharmacol 11(1): 80-94.
-
Akiyama O, Matsushima K, Nunez M, Matsuo S, Kondo A, et al. (2018) Microsurgical anatomy and approaches around the lateral recess with special reference to entry into the pons. Journal of Neurosurgery 129(3): 740-751.
-
Blake JA (1900) The roof and lateral recesses of the fourth ventricle, considered morphologically and embryologically. Journal of Comparative Neurology 10(1): 79-108.
-
Matsushima K, Yagmurlu K, Kohno M, Rhoton AL (2016) Anatomy and approaches along the cerebellar-brainstem fissures. J Neurosurg 124(1): 248-263.
-
Lawton MT, Quiñones-Hinojosa A, Jun P (2006) The supratonsillar approach to the inferior cerebellar peduncle: anatomy, surgical technique, and clinical application to cavernous malformations. Neurosurgery 59(4 Suppl 2): ONS244-ONS252.
-
Kawashima M, Matsushima T, Nakahara Y, Takase Y, Masuoka J, et al. (2009) Trans-cerebellomedullary fissure approach with special reference to lateral route. Neurosurg Rev 32(4): 457-464.
-
Rhoton AL (2000) Cerebellum and fourth ventricle. Neurosurgery 47(S3): S7-S27.
-
Nakahara Y, Matsushima T, Hiraishi T, Takao T, Funakiet T et al. (2013) Importance of awareness of the rhomboid lip in microvascular decompression surgery for hemifacial spasm. J Neurosurg 119(4): 1038-1042.
-
Johal J, Paulk PB, Oakes PC, Oskouian RJ, Loukas M, et al. (2017) A comprehensive review of the foramina of Luschka: history, anatomy, embryology, and surgery. Childs Nerv Syst 33(9): 1459-1462.
-
Horsburgh A, Kirollos RW, Massoud TF (2012) Bochdalek’s flower basket: applied neuroimaging morphometry and variants of choroid plexus in the cerebellopontine angles. Neuroradiology 54(12): 1341- 1346.
-
Sharifi M, Ungier E, Ciszek B, Krajewski P (2009) Microsurgical anatomy of the foramen of Luschka in the cerebellopontine angle, and its vascular supply. Surg Radiol Anat 31(6): 431-437.
-
Martin RG, Grant JL, Peace D, Theiss C, Rhoton AL (1980) Microsurgical relationships of the anterior inferior cerebellar artery and the facial-vestibulocochlear nerve complex. Neurosurgery 6(5): 483-507.
-
Rhoton AL (1974) Microsurgery of the internal acoustic meatus. Surg Neurol 2(5): 311-318.
-
Rhoton AL (200) The posterior fossa veins. Neurosurgery 47(S3): S69-S92.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?