Tracheostomy Decannulation: Traditional Method vs Single Stage Comparison
Objective: To evaluate the predictive relationship between independent variables (age, sex, BMI, hypertension, diabetes mellitus, chronic obstructive pulmonary disease (COPD), stroke, heart disease, pychiatric history and seizures, and successful tracheostomy decannulation (TD) with either the traditional method or single-stage method. Study Design: Retrospective chart review of both in-patient and out-patient clinic charts between the periods of January 1, 2013 and July 31, 2020 at Detroit Medical Center for information related to TD. Methods: Inclusion criteria include any patient diagnosed with tracheostomy status over the age of 18 years with decannulation. Exclusion criteria included no information about tracheostomy decannulation, i.e. incomplete medical records. Tracheostomy patients who underwent traditional TD (with capping trial) were compared to those who underwent newer single-stage TD (without capping trial). Chi-square analysis, multinomial regression analysis and t tests were performed to assess if there was a significant difference in successful TD between traditional method versus single-stage method. Binary dependent variable and independent variable relationship were analyzed with multinomial regression analysis with p<0.05 indicate a statistical significance. Results: Only 93 met the inclusion and exclusion criteria after 115 patient charts review. Majority of subjects were males 57% (n=53) .Oldest patient age was 81 years (mean=54.08; SD= 11.449). 49 was the highest BMI (mean=28.2; SD=6.86). There was no statistically significant difference between mean in age, sex, BMI, hypertension, diabetes mellitus, COPD, stroke, heart disease, psychiatric history, and seizures. Conclusion: This study showed the age, sex, BMI, hypertension, diabetes mellitus, COPD, stroke, heart disease, psychiatric history, and seizures are not significant indicators for successful TD in either method.
Introduction
A tracheostomy is a surgical airway for long term ventilator-dependent patients whom are unable to be intubate due to upper airway obstruction and impending upper airway obstruction [1, 2, 3]. Tracheostomy tubes are inherently foreign bodies, and as such cause tracheal stomal granulation, tracheal wall granulations, tracheal stenosis,, bleeding from tracheostomy wall due to aggressive tracheostomy suction, frequent lower respiratory tracheal infections, and loss of natural speech [4, 5]. Anxiety and depression are also common in tracheostomized patients due to loss of speech [6]. In view of above complications and sequelae, patients always want to remove their tracheostomy tube as soon as possible [7].
The process of weaning from tracheostomy to maintenance of spontaneous respiration and /or airway protection is termed “decannulation”. Currently, there are no universally accepted protocol for this Tracheostomy decannulation (TD) due to variability in existing algorithms [8].
Objective criteria for each of these may help better the clinical judgement of decannulation. This apparent simple step requires a near perfect coordination of brain, swallowing, coughing, phonation and respiratory muscles. Multifactorial aberrations in this complex interplay can result in its failure.
Moreover, inappropriate assessment of the above factors increases the risk of aspiration during and after the decannulation process. Old age, obesity, poor neurological status, sepsis and tenacious secretions are the predominant reasons of failed decannulation. This study evaluated the predictive relationship between independent variables (age, sex, hypertension, diabetes mellitus, COPD, stroke, heart disease, psychiatric history, seizures and BMI) and binary dependent variables (TD) with level of statistical significance of p<0.05.
Materials and Methods
Patient data was collected retrospectively from Electronic medical records in Detroit Medical Center. In- Hospital and ENT clinic patient records were examined between the periods of January 1, 2013 and July 31, 2020 for information related to TD in each study participant.
Inclusion criteria include any patient who had underwent tracheostomy over the age of 18 years with decannulation. Exclusion criteria included no information about the endeavor of decannulation due to incomplete documentation.
Clinical criteria of the patient for a considering TD in our institution include patients must pass swallow study without any aspiration, must not have tracheostomy secretions, must be alert and oriented x3 (person, time, place), must be weaned from mechanical ventilation for more than 72 hours.
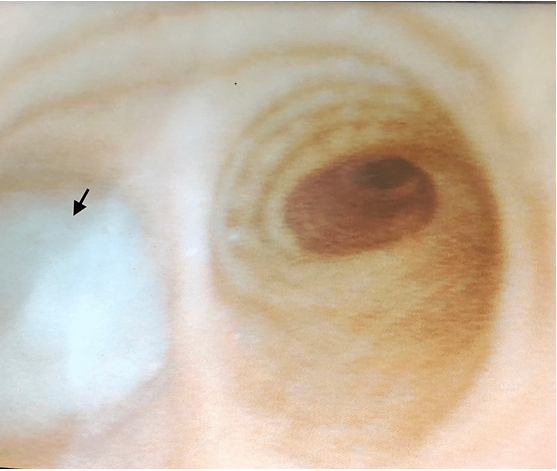
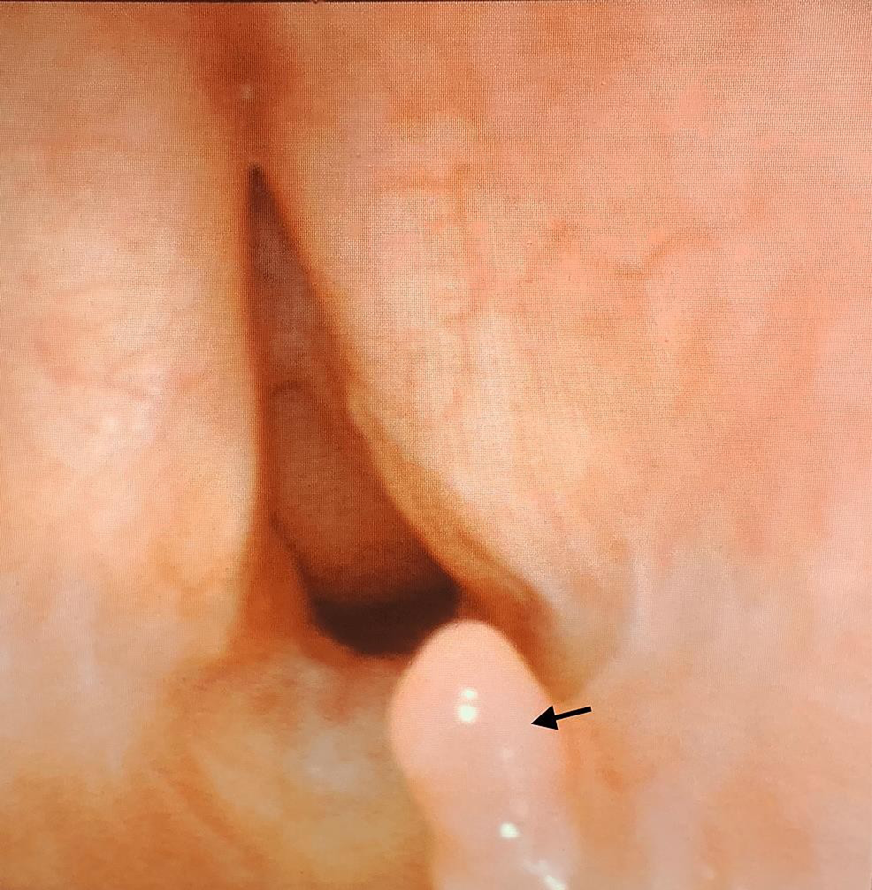
Once the patient met above criteria, the patient undergoes TD trial with either the single-stage method (TD without capping) or traditional method (TD with capping). Single-stage TD includes flexible fiberoptic laryngoscopy to evaluate the upper airway and vocal cord function. The tracheostomy tube is removed, and a bronchoscope is passed through the established tracheal stoma to evaluate the trachea and bronchus for secretions (Figure 1) and lesions such as tracheomalacia (Figure 2) .Bronchoscopy includes retroflexion for evaluation of subglottic stenosis and lesions (Figure 3).

If no abnormalities are found with laryngoscopy and bronchoscopy, occlusive dressing is applied over tracheal stoma without tracheostomy tube reinsertion. If no respiratory issues occur overnight (i.e. tachypnea >20 breaths per minute or oxygen desaturation <90% on room air), the patient can be discharged to home the next morning.
Traditional TD includes flexible fiberoptic laryngoscopy to evaluate the upper airway and vocal cord function. A bronchoscope is passed through the tracheostomy tube to evaluate the trachea and bronchus for lesions and secretions. If no abnormalities are found with laryngoscopy or bronchoscopy, the tracheotomy tube is changed to a capped No.4 cuff less tracheostomy tube, and the patient monitored overnight. The capped tube is then removed if the patient tolerates the capping trial and no respiratory issues occur overnight (i.e. tachypnea >20 breaths per minute or oxygen desaturation <90% on room air). Then, patient can be discharged to home.
Statistical Analysis
Minimum of 30 subjects were required for statistical analysis based on SPSS power analysis with confidence level of 99% with error margin is kept at 20%. 115 subjects were included.
Chi-square analysis, multinomial regression analysis and t tests were performed to assess if there was a significant difference in successful TD between traditional method versus single- stage method. The Categorical variables comparisons were done with Chi-square and Fisher exact test. Binary dependent variable and independent variable relationship were analyzed with multinomial regression analysis with p<0.05 indicate statistical significance.
Results
The aim of this study was to evaluate the predictive relationship between independent variables on successful TD. Independent variables include any age, sex, BMI, hypertension, diabetes mellitus, COPD, stroke, heart disease, psychiatric history, and seizures.
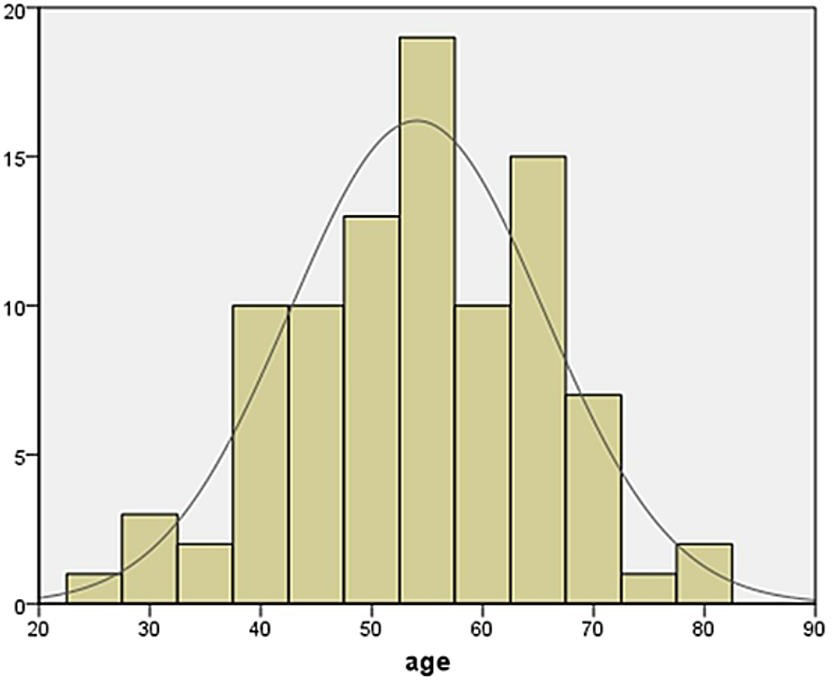
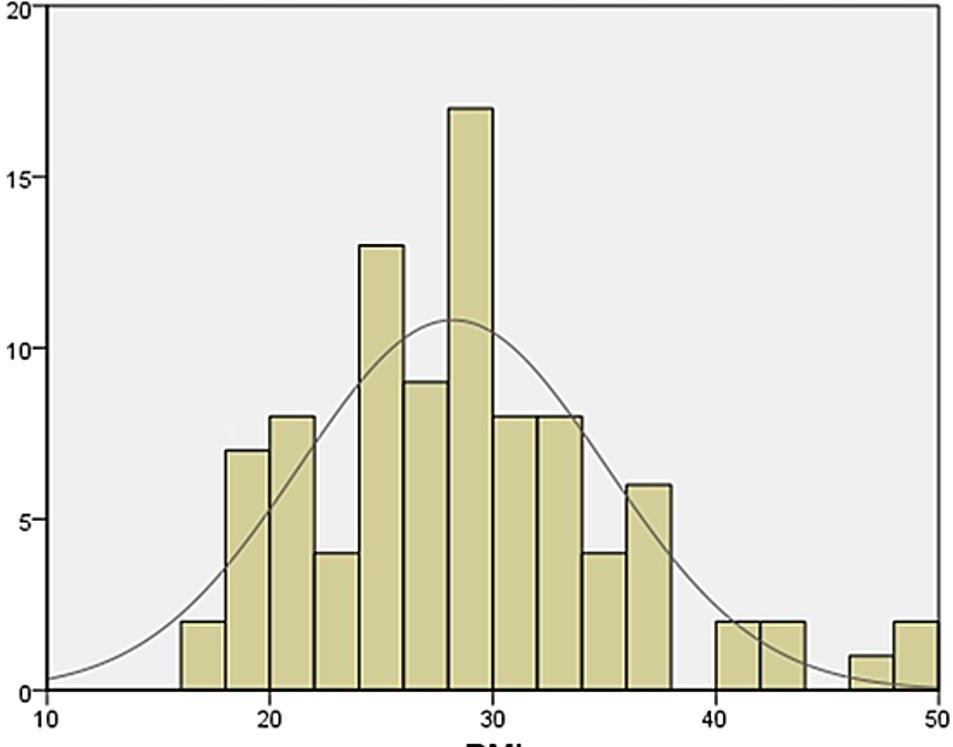
Only 93 met the inclusion criteria after 115 patient charts review. 61 subjects in traditional method and 32 subjects in single stage method were decannulated successfully. Majority of subjects were males 57% (n=53). 81 years was oldest and youngest was 25 years (mean=54.08; SD= 11.449) showed in age histogram (Figure 4). Figure 5 showed 49 was the highest BMI (mean=28.2; SD=6.86) Multinomial logistic regression was performed to determine predictive relationship between the independent variables and the binary dependent variables. Independent variables include age, sex (dummy codes: male=1, female=0), BMI, hypertension, diabetes, COPD, stroke, heart disease, psychiatric history, and seizures. The examined dependent variables were successful TD with traditional method versus single-stage method.
Our statistical analysis indicates no meaningful difference in sex (Χ2=0.049, p=0.825), hypertension (Χ2=0.051, p=0.822), diabetes mellitus (Χ2=0.912, p=0.34), COPD (Χ2=0.322, p=0.57), stroke (Χ2=0.191, p=0.662), heart disease (Χ2=0.299, p=0.584), psychiatric history (Χ2=0.569, p=0.451), and seizures (Χ2=0.136, p=0.712), indicating that these were not a predictor for traditional TD or single-stage TD in successful decannulation (Table 1).
| No of Tracheostomy decannulation without capping (Total-32) | No of Tracheostomy decannulation with capping first (Total-61) | χ2 | p | Significance | |
|---|---|---|---|---|---|
| Sex(male=1, female=0 | 18 | 35 | 0.05 | 0.83 | No |
| Hypertension | 22 | 40 | 0.51 | 0.82 | No |
| Diabetes mellitus | 9 | 20 | 0.91 | 0.34 | No |
| CPOD | 2 | 4 | 0.32 | 0.57 | No |
| Stroke | 2 | 4 | 0.19 | 0.66 | No |
| Heart Disease | 7 | 9 | 0.3 | 0.58 | No |
| Psychiatric history | 4 | 9 | 0.57 | 0.45 | No |
| Seizures | 3 | 4 | 0.14 | 0.71 | No |
Table 1: Multinomial Logistic Regression Showing Predictive Relationship between Independent and Binary Dependent Variables.
An independent sample t-test was conducted to determine if there is a difference between the mean in Age, sex, BMI, hypertension, diabetes mellitus, COPD, stroke, heart disease, psychiatric history and seizures of Single stage TD and Traditional TD (Table 2).
There was no statistically significant difference between mean in age, sex, BMI, hypertension, diabetes mellitus, COPD, stroke, heart disease, psychiatric history, and seizures.
- 1-single stage decanulation
- 0-trach capping first
- N
- Mean
- Standard
- Deviation
- Standard error of Mean t- value
- P- value
- Age in years
- 1
- 32
- 56.3
- 9.7
- 1.71
- 1.371
- 0.173
- 0
- 61
- 52.9
- 12.17
- 1.55 sex—male-1
- 1
- 32
- 0.56
- 0.504
- 0.089
- -0.103
- 0.918
- Female -0
- 0
- 61
- 0.57
- 0.498
- 0.063
- BMI
- 1
- 32
- 27.3
- 8.093
- 1.43
- -0.907
- 0.366
- 0
- 61
- 28.6
- 6.13
- 0.031
- HTN positive-1
- 1
- 32
- 0.68
- 0.47
- 0.08
- 0.305
- 0.76
- 0
- 61
- 0.65
- 0.479
- 0.061
- DM positive-1
- 1
- 32
- 0.28
- 0.456
- 0.08
- -0.456
- 0.649
- 0
- 61
- 0.327
- 0.473
- 0.06
- COPD positive-1
- 1
- 32
- 0.062
- 0.245
- 0.043
- -0.056
- 0.954
- 0
- 61
- 0.065
- 0.249
- 0.031
- Stroke
- 1
- 32
- 0.062
- 0.245
- 0.043
- -0.056
- 0.954
- 0
- 61
- 0.065
- 0.249
- 0.031
- Heart disease
- 1
- 32
- 0.218
- 0.42
- 0.074
- 0.858
- 0.392
- 0
- 61
- 0.147
- 0.357
- 0.045
- Psychiatric
- Disease
- 1
- 32
- 0.125
- 0.336
- 0.059
- 0.965
- 0.336
- 0
- 61
- 0.065
- 0.249
- 0.031
- Seizures
- 1
- 32
- 0.093
- 0.296
- 0.052
- 0.484
- 0.629
- 0
- 61
- 0.065
- 0.249
- 0.031
Table 2: Independent Sample T-Test.
Discussion
TD is a vital procedure for weaning tracheostomy- dependent patients on mechanical ventilation and eventually removing the cannula. However, there are no universally accepted criteria on which patients are eligible to attempt TD, nor is there a widely accepted protocol for TD [9].
These decisions are traditionally made by the expertise of the individual surgeon or by the multidisciplinary team in each hospital.
While TD appears like a simple step, it requires a near perfect coordination of brain, swallowing, coughing, phonation, and respiratory muscles [10]. Several other published articles also highlighted the importance of spontaneous cough, cough strength, airway patency, presence of secretions, and level of consciousness for successful decannulation [11, 12, 13].
TD process can be done with the traditional capping trial (multiple stages) or with the newer single-stage method. According to Criner et al., the traditional capping trial method may limit respiratory muscle function due to increase in airway resistance [14]. The traditional method is a slow process most of the time, leading to increased possibility of nosocomial infections and increased cost due to longer hospital stay [15].
In view of above mentioned disadvantages of traditional TD, Cohen et al. proposed the single- stage TD after a three- step endoscopic confirmation that evaluates the upper airway for vocal cord mobility, tracheobronchial wall lesions and secretions, and subglottic stenosis. In adult patients, single-stage TD is as safe as traditional TD and may provide the benefit of shortened hospital stay [8].
In our study, there was no significant difference with successful TD techniques (traditional versus single-stage) in regards to age, BMI, sex, hypertension, diabetes mellitus, COPD, stroke, heart disease, psychiatric history, and seizures. Our findings suggest that these factors are not significant indicators for predicting successful TD with either method.
Since we do not have large number of subjects, we cannot make a clear recommendation for how to proceed with TD.
However, this study highlights that there is no significant difference between traditional TD and single-stage TD.
It was conducted by two otolaryngology physicians at a single academic institution and retrospective data collections are the major limitations of this study.
Conclusions
Tracheostomy is surgical airway for longterm ventilator- dependent patients, unable to intubate due to upper airway obstruction and impending upper airway obstruction. However, the tracheostomy tube tends to cause several morbid complications as it is a foreign body to the upper airway. Therefore, TD should be considered as soon as possible with either traditional method or single-stage method, depending on the physician’s preference.
This study showed the age, sex, BMI, hypertension, diabetes mellitus, COPD, stroke, heart disease, psychiatric history, and seizures are not significant indicators for successful TD in either method.
Conflict of Interest: No competing interests have been disclosed in this article.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for- profit sectors.
References
-
Combes A, Luyt CE, Nieszkowska A, Trouillet JL, Gibert C, et al. (2007) Is tracheostomy associated with better outcomes for patients requiring long-term mechanical ventilation?. Crit Care Med 35(3): 802-807.
-
Rane S, Bathula S, Thomas RL, Natarajan G (2014) Outcomes of Tracheostomy in the Neonatal Intensive Care Unit: Is There an Optimal Time?. J Matern Fetal Neonatal Med 27(12): 1257-1261.
-
Hsu CL, Chen KY, Chang CH, Jerng JS, Yu CJ, et al. (2005) Timing of tracheostomy as a determinant of weaning success in critically ill patients: a retrospective study. Crit Care 9(1): 46-52.
-
Engels PT, Bagshaw SM, Meier M, Brindley PG (2009) Tracheostomy: from insertion to decannulation. Can J Surg 52(5): 427-433.
-
Singh RK, Saran S, Baronia AK (2017) The practice of tracheostomy decannulation—a systematic review. Journal of Intensive Care 5: 38.
-
O Connor HH, Kirby KJ, Terrin N, Hill NS, White AC (2009) Decannulation following tracheostomy for prolonged mechanical ventilation. J Intensive Care Med 24(3): 187- 194.
-
Mallick A, Bodenham AR (2010) Tracheostomy in critically ill patients. Eur J Anaesthesiol 27(8): 676-682.
-
Cohen O, Tzelnick S, Lahav Y, Stavi D, Shoffel-Havakuk H, et al. (2016) Feasibility of a single-stage tracheostomy decannulation protocol with endoscopy in adult patients. Laryngoscope 126(9): 2057-2062.
-
Mitchell RB, Hussey HM, Setzen G, Jacobs IN, Nussenbaum B et al. (2013) Clinical consensus statement: tracheostomy care. Otolaryngol Head Neck Surg 148(1): 6-20.
-
Garuti G, Reverberi C, Briganti A, Massobrio M, Lombardi F, et al. (2014) Swallowing disorders in tracheostomised patients: a multidisciplinary/ multiprofessional approach in decannulation protocols. Multidiscip Respir Med 9(1): 36.
-
Bishnoi T, Sahu PK, Arjun AP (2020) Evaluation of Factors Determining Tracheostomy Decannulation Failure Rate in Adults: An Indian Perspective Descriptive Study. Indian journal of otolaryngology and head and neck surgery 74(S3): 4849-4854.
-
Enrichi C, Battel I, Zanetti C, Koch I, Ventura L et al. (2017) Clinical Criteria for Tracheostomy Decannulation in Subjects with Acquired Brain Injury. Respiratory care 62(10): 1255-1263.
-
Perin C, Meroni R, Rega V, Braghetto G, Cerri CG et al. (2017) Parameters Influencing Tracheostomy Decannulation in Patients Undergoing Rehabilitation after severe Acquired Brain Injury (sABI). International archives of otorhinolaryngology 21(4): 382-389.
-
Criner G, Make B, Celli B (1987) Respiratory muscle dysfunction secondary to chronic tracheostomy tube placement. Chest 91(1): 139-141.
-
Heffner JE, Hess D (2001) Tracheostomy management in the chronically ventilated patient. Clin Chest Med 22(1): 55-69.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?