The Effect of Effortful Swallow with Progressive Resistance on Swallow Function in Post-Stroke Dysphagia: A Case Study
Background: Dysphagia management is vital in individuals reporting swallowing difficulties post-stroke. The literature review recommends the effortful swallow maneuver as a simple technique with multiple benefits for treating patients with oropharyngeal dysphagia due to stroke. No studies have documented the effect of effortful swallow and progressive resistance in individuals with swallowing difficulties post-stroke. Aim: To investigate whether the effortful swallow with added progressive resistance helps alleviate the swallowing function in individuals with dysphagia following stroke. Case report: In this case report, we describe a 30-year-old male who presented with left middle cerebral artery infarction and subsequent swallowing difficulty. The treatment procedure included 20 sessions of swallowing therapy incorporating effortful swallow with progressive resistance. Conclusion: Following 20 sessions of swallow treatment, significant improvement was seen in oro-facial measurements such as anterior and posterior tongue strength, anterior and posterior tongue endurance, and typical and effortful swallow tongue pressure. Functional oral intake level, dysphagia outcome and severity levels also improved significantly, contributing to better quality of life. Fiberoptic Endoscopic Evaluation of Swallowing (FEES) examination showed improved swallow safety and efficiency post-therapy. Conclusion: Effortful swallow with progressive resistance effectively improved oro-pharyngeal swallow functions in an individual who presented with dysphagia following stroke. The case study highlights the effect of effortful swallow with progressive resistance in treating swallowing difficulties in a participant who presented with dysphagia following stroke
Introduction
Dysphagia or swallowing difficulty affects 39-80% of stroke survivors [1]. The early identification and management of dysphagia in acute stroke survivors is essential to avoid complications such as aspiration, dehydration and death. Most dysphagia treatment aims to prevent complications and promote quality of life. Swallowing maneuvers constitute a vital part of treatment in patients with oropharyngeal dysphagia. According to Molfenter, et al. [2], one such maneuver is the Effortful Swallow (ES), often used to enhance swallowing and reduce pharyngeal residue while also serving as a strength training exercise. Many authors regard the ES maneuver as a ‘volitional manipulation of the oro-pharyngeal phase of swallowing’ [3]. The tongue is an essential component of this maneuver, pressing firmly against the hard palate in an upward and backward motion while simultaneously contracting the throat muscles and swallowing as forcefully as possible [4].
The effortful swallow maneuver assists the progress of bolus flow via the pharynx, increasing the intrabolus pressure and thereby facilitating tongue base contact with the posterior pharyngeal wall during swallowing, which clears the vallecular residue [5]. Thus, the effortful swallow aids in safe bolus propulsion by lowering the risk of aspiration by lengthening the time of laryngeal vestibule closure and reducing bolus residue [3, 6].
Studies documenting the effect of an effortful swallow on post-stroke dysphagia have shown positive findings in targeting labial and lingual strength and oro-pharyngeal swallow functions [4, 7]. A recent study by Oh [8] reported that effortful swallow in conjunction with progressive resistance improves swallow abilities, particularly in older adults. Providing progressive resistance overloads the muscles and increases strength [9]. It would be interesting to investigate whether increasing resistance in conjunction with an effortful swallow could aid in regaining swallow function and boosting tongue strength in people who have experienced a decrease in swallow function secondary to stroke. Moreover, quantifying the effort in ES is challenging, and hence, it would also be interesting to study whether providing feedback would enable more active participation and better swallow outcomes.
Studies documenting the effect of the effortful swallow with progressive resistance and feedback using Iowa Oral Performance Instrument (IOPI) are limited. Additionally, there are no studies documenting the treatment effect of this technique on oro-pharyngeal swallow functions and functional outcome measures such as functional level of oral intake, severity of dysphagia, and quality of life in individuals exhibiting swallowing difficulties post-stroke. Hence, the objective of the study was to investigate the effect of effortful swallow with progressive resistance on tongue strength (anterior and posterior), tongue endurance (anterior and posterior), typical and effortful swallow tongue pressure, functional level of oral intake, the severity of dysphagia and quality of life by comparing pre, mid and post-treatment scores in an individual with post-stroke dysphagia.
Case Report
A 30-year-old male diagnosed with oro-pharyngeal dysphagia secondary to stroke served as the participant in the study. The participant reported to the centre for swallowing disorders with the primary complaint of difficulty swallowing thin liquids (10 ml and above) with intermittent cough post- consumption of thin liquids since one month. He belonged to lower socio-economic status and was an auto driver by profession. A detailed history revealed that the participant had co-morbidity (hypertension) since 1year and was under medication for the same. No other significant medical history was reported. The Computed Tomography (CT) findings revealed acute infarct in the left frontoparietal regions. The patient underwent craniectomy, post which a CT scan showed a left-fronto-parietal craniectomy defect with post- operative changes. Small epidural collections were seen at the operative site. The left fronto-parietal lobe showed white matter edema. The participant was under medication as prescribed by the neurologist (Ecosprin-AV75 & Liofen-10).
The clinical swallow evaluation revealed that he could take semisolids and solids orally (5-10ml) without choking or swallowing difficulty. The participant demonstrated poor bolus preparation and propulsion for bolus volumes (>10ml) and exhibited multiple swallows and oral residue. Additionally, the participant reported longer meal times. The oro-motor examination, language, cognitive, and swallow evaluations (FEES, FOIS & DOSS) are summarized in (Tables 1 & 2).
The study followed the “Ethical Guidelines of Bio- Behavioral Research Involving Human Subjects” [10] and was approved by the Ethical Committee of the Institute (No. DOR.9.1/Ph. D/BC/920/2021-2022 dated 10th February 2023). Before the commencement of the training, the study purpose, the risk, and the procedure were explained to the participant and the caregiver, and written consent was obtained. A baseline evaluation was carried out in which the measures of tongue strength and endurance (anterior and posterior) and typical and effortful swallow tongue pressure were obtained using the Iowa Oral Performance
Instrument® (IOPI), version 3.1(IOPI Pro, Model 3.1; Medical LLC, WA, USA). In addition, the Functional level of oral intake was evaluated using the Functional Oral Intake Scale (FOIS; [11]), the functional severity of dysphagia was measured using Dysphagia Outcome Severity Scale (DOSS; [12]) and the quality of life was assessed using swallowing quality of life tool (SWAL-QOL; [13]). After the baseline evaluation, 20 sessions of effortful swallow with progressive resistance training were provided (5 days/week for four weeks). All the measures obtained at baseline were repeated at mid- treatment (10th session) and post-treatment phase (20th session).
| Test administered | Findings |
| Oral Peripheral Mechanism Examination (OPME) | Jaw at rest- NormalJaw movements (vertical, rotatory, lateral)- AffectedLips at rest- Deviated towards the rightProtrusion and retraction- Restricted range and speed.Tongue at rest- Normal Tongue protrusion, elevation, retraction, sweep, and alternate movements- are affected.Hard palate- NormalSoft palate- NormalSoft palate elevation- normal; Gag- presentPharyngeal wall- NormalMedial wall movement- Present |
| Gugging Swallowing Screen (GUSS) | A score of 15-19 indicates slight dysphagia with aspiration risk, swallowing semisolids successful, and swallowing liquids and solids can be deficient. |
| Penetration/ Aspiration Score (PAS) | Thin liquids, score 4: Material enters the airway, contacts the vocal folds, and is ejected from the airway |
| Pharyngeal Residue Severity Rating Scale | Overall score of III- Indicative of mild residue for all the consistencies |
| Functional Oral Intake Scale (FOIS) | Level 5: Total oral diet with multiple consistencies requiring special preparation or compensations. |
| Dysphagia Outcome and Severity Scale (DOSS) | Level 5: Mild dysphagia |
Table 1: Findings of Swallow Evaluation.
| Test administered | Findings | |
|---|---|---|
| Speech | Informal evaluation | The participant has limited verbal output. The speech intelligibility was fair. Reduced loudness and strained voice quality were observed. |
| Language | Western Aphasia Battery in Kannada (WAB-K) | Fluency-02/10Auditory Verbal Comprehension- 5/10Repetition-02/10Naming- 03/10Apraxia component- AbsentImpression: Broca’s Aphasia |
| Cognition | Montreal Cognitive Assessment (MoCA-K) | A score of 21 on 30, indicative of mild cognitive impairment |
Table 2: Findings of Speech, Language, and Cognitive Examination.
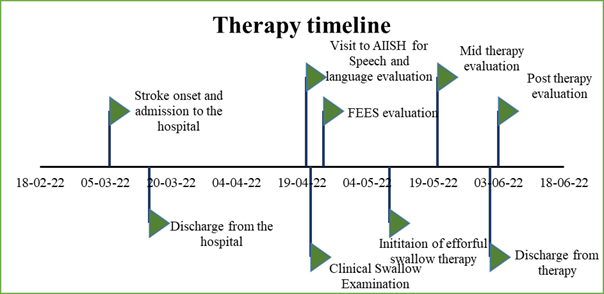
The participant was enrolled for swallow therapy using the effortful swallow with progressive resistance program for 20 sessions. The participant was not offered any other swallowing maneuver and sensory enhancement techniques. A timeline of patient admission and entire therapy details are shown in Figure 1.
Intervention
The participant recruited for the study received effortful swallow with a progressive resistance training regime. The participant was asked to sit upright on a solid chair with an armrest, and the following instruction was given: “Swallow very hard while squeezing the tongue in an upward-backward motion toward the soft palate” [14]. In the first ten sessions, the participant performed 30 effortful swallows with 50% of the lingual peak pressure, followed by 45 effortful swallows (subsequent ten sessions) with pressure increased to 70% (measured at the end of the 10th session training program). The intensity of the effortful swallow and external resistance was progressively increased based on the strength training principles [9]. The investigator affirmed the performance by directly observing oro-facial structures and palpating suprahyoid muscles under the chin [4]. Additionally, IOPI was utilized to assess the accuracy of the effortful swallow regimen and to offer feedback (verbal and visual).
Results
The patient was discharged after completing 20 sessions of swallow therapy incorporating the abovementioned protocol. The results of the outcome measures related to swallow safety, efficiency, functional outcomes and oro-facial measurements are listed in Table 3.
| Domain | Pre-therapy | Mid-therapy | Post-therapy |
|---|---|---|---|
| Penetration/ Aspiration Score (PAS) | Thin liquids: score 4 Thick liquids: score 3 Semi solids: score 2 Solid: score 2 | Thin liquids: score 2 Thick liquids: score 1 Semi solids: score 1 Solid: score 1 | Score 1: Material does not enter the airway (all consistencies) |
| Pharyngeal Residue Severity Rating Scale | Score III: Mild residue noted for all consistencies | Score I: Indicative of no residue for all consistencies except thick liquid. | Score I- Indicative of no residue for all consistencies except thick liquid. |
| Functional Oral Intake Scale (FOIS) | Level 5: Total oral diet with multiple consistencies requiring special preparation or compensation. | Level 6: Total with multiple consistencies, but without special preparation but with specific food limitation | Level 7: Total oral diet without any restrictions |
| Dysphagia Outcome and Severity Scale (DOSS) | Level 5: Mild dysphagia | Level 6: within functional limits/ modified independence | Level 7: Within normal limits; No symptoms of dysphagia |
| Swallowing quality of life | 41.4/100 | 62.9/100 | 71.6/100 |
| Anterior tongue strength (kPa) | 32 | 36 | 42 |
| Posterior tongue strength (kPa) | 33 | 35 | 40 |
| Anterior tongue endurance (sec) | 16 | 43 | 60 |
| Posterior tongue endurance (sec) | 9 | 9 | 15 |
| Typical swallow tongue pressure (kPa) | 28 | 31 | 37 |
| Effortful swallow tongue pressure (kPa) | 36 | 45 | 56 |
Table 3: Summary of the FEES Evaluation, Functional Outcomes Measures and Oro-Facial Measurements: Pre-Therapy, Mid- Therapy (
Note: PAS score- Score 4- material enters the airway, contacts the vocal folds, is ejected from the airway; Score 3- material enters the airway, remains above vocal folds, is not ejected from the airway; Score 2- material enters the airway, remains above the vocal folds, and is ejected from the airway. Table 3: Summary of the FEES Evaluation, Functional Outcomes Measures and Oro-Facial Measurements: Pre-Therapy, Mid- Therapy (10th Session), and Post-Therapy (20th Session).
Discussion
The study involved the administration of effortful swallow with progressive resistance on a single participant with post-stroke dysphagia (1month post-stroke). The effortful swallow exercise program is task-specific and suitable for targeting oral and pharyngeal swallowing functions. After the treatment (20 sessions), the participant showed remarkable improvement in tongue strength, tongue endurance, typical and effortful swallow tongue pressure, functional swallow outcome measure, and swallowing quality of life. Hence, the technique effectively increases swallow-related muscle strength, alleviates the severity of dysphagia, and improves the quality of life.
For swallowing, the tongue plays a vital role in bolus propulsion by pushing against the hard palate. It creates adequate intraoral pressure and facilitates pharyngeal pressure and safe swallowing. Typically, patients with dysphagia exhibit weaker oro-pharyngeal strength, sequentially affecting swallowing quality of life [7]. It is deemed essential to target tongue strength and thereby facilitate swallow function and quality of life. Various tongue- related measures, i.e., tongue strength and endurance (anterior and posterior), typical and effortful swallow tongue pressure measures improved compared to baseline. These effects can be attributed to the training regime of effortful swallow with progressive resistance in improving oral muscle strength.
Additionally, the participant received immediate feedback, which helped him understand the complex yet subtle swallowing process, thereby improving swallow motor control. Robbins, et al. [15] state that using resistance training (IOPI) significantly improves oral muscle strength and further contributes to safe swallowing due to improving muscle strength. Kim, et al. [7] found similar results using the tongue to palate resistance training which facilitated tongue pressure.
Functional outcome measure in terms of oral intake level, quality of life improved compared to baseline. The dysphagia severity was reduced with the intensive treatment protocol. The current study is the first to document the effect of effortful swallow with progressive resistance on outcome measures such as FOIS, DOSS, and SWAL-QOL. Studies support the effect of traditional therapy and specific treatment protocols (NMES, Mc Neil Dysphagia therapy) on FOIS [16, 17]. The Dysphagia severity measure decreased from mild to normal in all circumstances, suggesting that the participant could now swallow all types of food with all consistencies without exhibiting any aspiration symptoms. Due to improved oro- muscular strength and swallow functions, quality of life progressed towards near normalcy. In addition, Steele, et al. [18] proposed that tongue resistance exercise improves swallowing quality of life in stroke patients by successfully reducing aspiration and penetration. The current study accounts for significant improvement in all swallowing quality of life domains post-treatment protocol.
Conclusion
The case study is the first study that varied the resistance and offered feedback (IOPI) along with effortful swallow. The study results are promising in targeting tongue strength, endurance, typical and effortful swallow tongue pressure, functional swallow outcome measures, and quality of life in an individual with post-stroke dysphagia. The single case study is a preliminary attempt to evaluate the long-term training (20 sessions) effect of effortful swallow with progressive resistance in an individual with swallowing difficulty secondary to stroke. The case study incorporating effortful swallow with progressive resistance unravels the benefits of a simple technique for effectively treating dysphagia following a stroke. Further studies on a larger population are warranted to provide evidence for the technique.
Acknowledgment
The authors thank Dr. M. Pushpavathi, Director, AIISH, for permitting the study and providing the necessary resources and infrastructure. We would also like to thank the University of Mysuru (UOM) for its constant support. The authors also thank the participant of the current study.
Statement of Ethics
The participant had given his written informed consent. According to the Declaration of Helsinki, the ethical clearance was obtained from the Institutional Review Board, AIISH Ethics Committee (AEC), Approval number: No.DOR.9.1/Ph. D/BC/920/2021-2022 dt 10th February 2023.
Conflict of Interest
The authors have no conflict of interest to declare.
Funding Sources
There are no funding sources to declare
Author Contributions
BC and SN: conceptualizing and designing the research study, seeking ethical approval, data collection, analyzing the data, and drafting the manuscript in whole or in part. Both authors have approved the final manuscript.
Data Availability Statement
All data generated or analyzed during this study are included in the article. Further inquiries can be directed to the corresponding author.
References
-
Takizawa C, Gemmell E, Kenworthy J, Speyer R (2016) A Systematic Review of the Prevalence of Oropharyngeal Dysphagia in Stroke, Parkinson’s Disease, Alzheimer’s Disease, Head Injury, and Pneumonia. Dysphagia 31(3): 434-441.
-
Molfenter SM, Hsu CY, Lu Y, Lazarus CL (2018) Alterations to Swallowing Physiology as the Result of Effortful Swallowing in Healthy Seniors. Dysphagia 33(3): 380- 388.
-
Nekl CG, Lintzenich CR, Leng X, Lever T, Butler SG (2012) Effects of Effortful Swallow on Esophageal Function in Healthy Adults. Neurogastroenterol Motil 24(3): 252- 256.
-
Park H, Oh D, Yoon T, Park J (2019) Effect of Effortful Swallowing Training on Tongue Strength and Oropharyngeal Swallowing Function in Stroke Patients with Dysphagia: A Double‐Blind, Randomized Controlled Trial. Int J Lang Commun Disord 54(3): 479-484.
-
Pouderoux P, Kahrilas PJ (1995) Deglutitive Tongue Force Modulation by Volition, Volume, and Viscosity in Humans. Gastroenterology 108(5): 1418-1426.
-
Hind JA, Nicosia MA, Roecker EB, Carnes ML, Robbins J (2001) Comparison of Effortful and Noneffortful Swallows in Healthy Middle-Aged and Older Adults. Arch Phys Med Rehabil 82(12): 1661-1665.
-
Kim HD, Choi JB, Yoo SJ, Chang MY, Lee SW, et al. (2017) Tongue-to-Palate Resistance Training Improves Tongue Strength and Oropharyngeal Swallowing Function in Subacute Stroke Survivors with Dysphagia. J Oral Rehabil 44(1): 59-64.
-
Oh JC (2022) Effects of Effortful Swallowing Exercise with Progressive Anterior Tongue Press Using Iowa Oral Performance Instrument (IOPI) on the Strength of Swallowing-Related Muscles in the Elderly: A Preliminary Study. Dysphagia 37(1): 158-167.
-
Burkhead LM, Sapienza CM, Rosenbek JC (2007) Strength-Training Exercise in Dysphagia Rehabilitation: Principles, Procedures, and Directions for Future Research. Dysphagia 22(3): 251-265.
-
Basavaraj V, Venkatesan S (2009) Ethical Guidelines for Bio-Behavioural Research Involving Human Subjects. All India Institute of Speech and Hearing pp: 1-23.
-
Crary MA, Mann GDC, Groher ME (2005) Initial Psychometric Assessment of a Functional Oral Intake Scale for Dysphagia in Stroke Patients. Arch Phys Med Rehabil 86(8): 1516-1520.
-
O’ Neil KH, Purdy M, Falk J, Gallo L (1999) The Dysphagia Outcome and Severity Scale. Dysphagia 14(3): 139-145.
-
McHorney CA, Martin-Harris B, Robbins J, Rosenbek J (2006) Clinical Validity of the SWAL-QOL and SWAL- CARE Outcome Tools with Respect to Bolus Flow Measures. Dysphagia 21(3): 141-148.
-
Bülow M, Olsson R, Ekberg O (1999) Videomanometric Analysis of Supraglottic Swallow, Effortful Swallow, and Chin Tuck in Healthy Volunteers. Dysphagia 14(2): 67- 72.
-
Robbins J, Kays SA, Gangnon RE, Hind JA, Hewitt AL, et al. (2007) The Effects of Lingual Exercise in Stroke Patients with Dysphagia. Arch Phys Med Rehabil 88(2): 150-158.
-
Huang KL, Liu TY, Huang YC, Leong CP, Lin WC, et al. (2014) Functional Outcome in Acute Stroke Patients with Oropharyngeal Dysphagia after Swallowing Therapy. J Stroke Cerebrovasc Dis 23(10): 2547-2553.
-
Carnaby GD, LaGorio L, Silliman S, Crary M (2020) Exercise‐based swallowing intervention (McNeill Dysphagia Therapy) with adjunctive NMES to treat dysphagia post‐stroke: A double‐blind placebo‐ controlled trial. J Oral Rehabil 47(4): 501-510.
-
Steele CM, Bailey GL, Polacco REC, Hori SF, Molfenter SM, et al. (2013) Outcomes of Tongue-Pressure Strength and Accuracy Training for Dysphagia Following Acquired Brain Injury. Int J Speech Lan Pathol 15(5): 492-502.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?