Huge Subglottic Stalked Polyp Treated by Endoscopic Polypectomy Snare at Jalalabad Afghanistan
Polyps are the common benign mucosal lesions of larynx. Usually present as exophytic lesion with thin mucosa. Horsiness is a common symptom and rarely large subglottic polyp causes dyspnea. A patient with horsiness and shortness of breath due to a huge laryngeal polyp around 2cm with thin stalk, linked to thyroid angle below the vocal cords. According the combined decision of Otorhinolaryngologist, Endoscopist and Anesthesiologist, underwent resection of the mass by endoscopic polypectomy snare with electrocautery without any residues and damages. The dyspnea and hoarseness relieved. The histopathological findings confirmed vocal cord benign mass lesion. We consider that careful intubation under the direct vision of bronchoscopy and electrocautery is the safest and useful procedure to secure the upper airway successfully in cases of large subglottic polyp showing dyspnea.
Introduction
Vocal cords nodules, polyp and Reinke edema are the most common benign mucosal lesions arise from the true vocal cords. Overall, prevalence of laryngeal lesions in the papulation reported 1.96%. After the vocal nodules (1.0- 1.7%) vocal polyps are the second most prevalent lesion (0.3 – 0.6%) [1]. Usually, occur along the mid membranous portion of the vocal fold and present as an exophytic or pedunculated lesion with thin mucosa. Voice abuse/disuse, smoking, allergy, gastroesophageal reflux and chronic infection are the common etiologies. People, who require occupationally excessive usage of voice, are at high risk [2, 3]. Generally, vocal fold polyps are benign and unilateral but can be bilateral or multiple.
Classified morphologically, as sessile or pedunculated, and histologically as fibrous vs. organized, gelatinous vs. translucent and angiomatous vs. hemorrhagic [4]. The clinical features in individuals, depend on the size and site of the polyps are; hoarseness, breathlessness and vocal fatigue, dysphonia, foreign body sensation, wheezing, stridor [2, 3], and in rare cases even upper airway obstruction by large or giant polyps [5, 6]. Polyps at the subglottic area would flop the rhythm of respiration following the polyp hinging. Given the possibility of airway obstruction and spasm caused by bouts of coughing, vomiting or any manipulation at the laryngeal inlet in the base of huge vocal polyp [7, 8, 9] one should be aware when a patient has a dyspnea and voice problem. As the surgery is adopted for the treatment of vocal fold lesion [10] the tracheostomy and microlaryngoscopic excision is a preferred method, carefully done by otolaryngologist and anesthetist, mutually carried out in cases of huge vocal polyp causing airway obstruction. However, recent researches demonstrated the importance of speech therapy as a primary treatment of polyps, with total or partial lesion regression, followed by surgery when the lesions are persistent or if the patients are dissatisfied with their vocal quality [11, 12, 13, 14]. We hereby report a case of huge subglottic polyp in which an intubation and endoscopic polypectomy procedure was executed for removing the subglottic stalked polypoidal mass successfully.
Case Report
A 52-year-old man visited ENT doctor with worsen hoarseness and shortness of breath that gradually increased in intensity since14 months. He was complaining deteriorating shortness of breath, in unusual situations such as in bathing and anxious states. He had sometimes coughed, but no odynophagia, dysphagia, lesion in the oral cavity, oropharynx and neck region.
As a shopkeeper in Kabul city that prompted voice overuse and throat irritation, he had snuff (a kind of tobacco substances used sublingual or behind the lips) addiction for more than 30 years, but no smoking and no history of gastroesophageal reflux diseases.
On physical examination, mild cyanosis on the face and lips, mildly tachypnea, biphasic inspiratory stridor with suprasternal recession were detected, but his body temperature, body mass index (BMI), and oxygen saturation were in normal ranges. No neck mass or enlarged lymph nodes, other systemic illness such as epiglottitis, angioedema, were detected and the chest x-ray was also normal.
A fiberoptic bronchoscopic laryngeal examination performed to oversee hypopharynx, larynx and probable laryngeal mass lesion. An about 2cm huge subglottic, rounded, reddish, nodular and a thin short stalk mass was adhered to the thyroid angle, flopping with respiration, occupying glottis area and leading to breathing difficulty (Figure 1). Other supraglottic area, epiglottis, vallecula, base of tongue and pyriform sinus were normal.
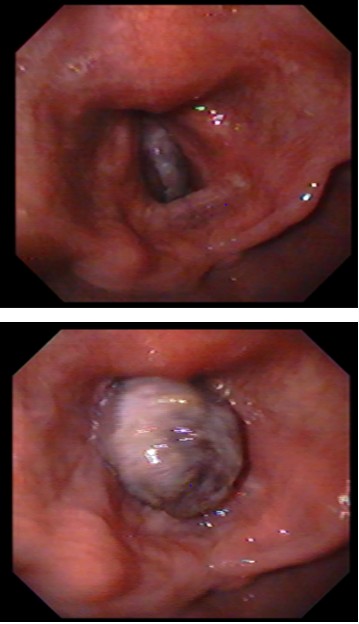
Image 1: Polyp Position Below from True Vocal Cards with Down Mobility. Olympus CLV 100
Image 2: Polyp Position Upper from True Vocal Cards with Up Mobility. Olympus CLV 100. Figure 1: Endoscopic View of Large Subglottic Polyp.
As the preferred Micro Laryngeal Surgery (MSL) with tracheostomy was considered relatively hard and complicated, while we had the experience of successful treatment of similar polyps in gastrointestinal tube with no or minor complications by endoscopic polypectomy electrocautery procedure, so with joint agreement of gastroenterology endoscopist, anesthesiologist, and otolaryngologist, the same endoscopic resection, as a trial to treat a vocal cord huge subglottic polyp was proposed.
After the performing all necessary lab examinations and medical consultations, patient had been pre-medicated as per OT protocol, given GA in supine position, carefully passed a small size tracheal tube around the free end of polyp to the trachea under the direct view of Gastroscope, placed with balloon inflation and blocked the airway. Patient positioned in Boyce Jackson position and provided chest support [15]. Adult gastro-scope passed through the chest support and settled just above the laryngeal inlet.

Medium size polypectomy snare (2.5cm) passed through the work channel of gastroscope and opened around the free end of polyp then rounded to the base of polyp stalk and gradually closed completely and cut with 300 of electrocautery. Fortunately, procedure ended successfully without any complication and also tolerated by patient (Figure 2). Removed polyp tissue specimen sent to pathology department for the final result.
At the end of endoscopic procedure, patient’s airway and secretions completely cleared, bleeding and tissue damages were prevented and he carried to the recovery room under the closed supervision of recovery staff and recovered (awaked form GA) in two hours, tracheal tube been removed, he was nauseated and groggy but able to self-respire, however prohibited from speaking up to sex hours. After the sex hours was able to speak without any restlessness and did not suffer from hoarseness and stridor.
Patient referred to the general ward and was hospitalized up to 24 hours to check the surgical site for signs of bleeding or infection, relieve pain and assure that vital signs are normal, then discharged with necessary medications, instructions. By day-3 and day-10 he was contacted via phone call and asked about his health states, as fortunately had no any previous and new complaints and was able to speak loudly. After a month he was asked to visit his doctors for final checkup examination. Clinically patient was breathing and speaking normally, no stridor and no chest tightness noted.
The follow-up fiberoptic bronchoscopic laryngeal examination revealed normal laryngeal appearance with normal vocal card movements. No subglottic edema, redness, residual lesion, granuloma or scare had seen and airway was completely open (Figure 3).
Polypoidal tissue biopsy showed surface ulceration and necrotic inflammatory exudate, therefore, histopathological findings indicated a diagnosis of vocal cord polyp with chronic dense inflammation.
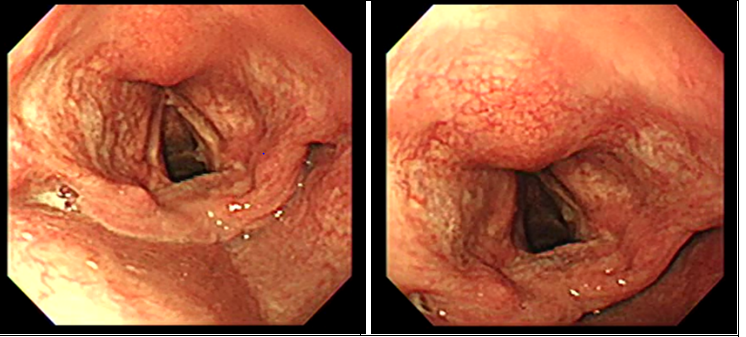
a b Figure 3: Paten airway after one month. Figures 3a & 3b: One Months Later From Polypectomy. Olympus CV 260.
Discussion
Vocal polyps are the usual benign lesions of larynx, present with hoarseness, vocal fatigue, cough or foreign body sensation, dysphonia rarely with acute airway obstruction.
Large laryngeal polyps usually cause acutely respiratory distress and rarely cause acutely airway obstruction which may become life threatening [7]. Small or hemorrhagic polyp is not indicated for surgical intervention, but large laryngeal polyps with some degree of airway obstruction need micro- laryngeal surgery. Repeated endotracheal intubations may damage the vocal cords and trachea rings or prompt laryngospasm and even complete airway obstruction [16].
Therefore, the tracheostomy for assisting and simplify the removal of polyp is the alternative choice [17].
And given the extent, size, length and diameter of the lesion in relation to vessels the laryngeal polyps, performed in general anesthesia with safe intubation to succor large polyps’ removal with laryngeal microsurgery [10, 18, 19].
Our case; a huge mobile stalked subglottic polyp, attached to the thyroid angle between the vocal cords was similar to the gastrointestinal tract polyps. Given to our over 5 years the gastrointestinal endoscopy and likewise the gastrointestinal polyps’ treatment experience with no or minor complications by endoscopic polypectomy electrocautery procedure, and compared via a number of liable discussions on; a) direct viewed field observation via screen in endoscopy vs. microscopic magnification in MLS procedure, b) less-time in endoscopy, as stalk cut and diathermy are both done simultaneously compared with MLS both procedures are performed separately, c) Bleeding and trauma chances are reasonably lees with endoscopic procedure, and other parameters of safety and efficacy of the endoscopic polypectomy electrocautery without tracheostomy. We judiciously validate the treatment as; endoscopic polypectomy resection without tracheostomy, as succeeded without any major or minor complication. This new treatment method has not mentioned yet in the literatures; therefore, we reported in detail as a case report.
In 2016 a case of large laryngeal polyp of 62year old women that caused airway obstruction was reported from Japan with performed trachiostomy under local anesthesis then examined by laryngoscopy to visualise the laryngeal mass, origineted from right vocal cord. Mass excised by a pair of microscissors, pathologically was benigen and after two weeks patient discharged [20].
A case of 48year old man with huge subglottic polyp was reported in Korea. He visited emergency department with sever dyspnea and dysphonia. First, was tracheostomy with local anesthesia then tried under general anesthesia for laryngeal microsurgery but was failed finally polyp removed with open laryngofissure surgery which was connected to the left vocal cord [21].
Conclusion
We consider that careful intubation under the direct vision of bronchoscopy or endoscopy and electrocautery with contribution of gastrointestinal tract endoscopist is the safest and useful procedures to guarantee the upper airway in cases of large subglottic polyp showing sever hoarseness and dyspnea. We hereby report a case of huge subglottic polyp in which an intubation and electrocautery with polypectomy snare was required for removing the subglottic mass successfully.
Acknowledgements
We would like to acknowledge the ENT specialist Dr. Jahanzib Sahar which assisted in the treatment procedure, anesthesiologist Dr. Gulam Gul Ahmadi and all staffs of OT, recovery and ward that cared and followed up the patient well.
Funding
This work was not funded
Disclosure Statement
No conflicts of interest for declaration by any of the authors.
Author contributions
Shinwari conceived the idea of endoscopic polypectomy by electrocautery, used gastrointestinal tract endoscopy accessories successfully during procedure. Safi discussed and leaded the combine decision for procedure and chest support instruments during procedure. Awab conceived the idea of case report, designed the study protocol and finally seen the manuscript. All authors read and approved the final manuscript and contributed to the intellectual content of the articles.
References
-
Woo SH, Kim RB, Choi SH, Lee SW, Won SJ (2014) Prevalence of laryngeal disease in South Korea: data from the Korea National Health and Nutrition Examination Survey from 2008 to 2011. Yonsei Medical Journal 55(2): 499-507.
-
Dikkers FG, Nikkels PG (1999) Lamina propria of the mucosa of benign lesions of the vocal folds. The Laryngoscope 109(10): 1684-1689.
-
Hantzakos A, Remacle M, Dikkers FG, Degols JC, Delos M, et al. (2009) Exudative lesions of Reinke’s space: a terminology proposal. European archives of oto-rhino- laryngology 266(6): 869-878.
-
Martins RHG, Defaveri J, Domingues MAC, E Silva RDA (2011) Vocal polyps: clinical, morphological, and immunohistochemical aspects. Journal of Voice 25(1): 98-106.
-
Kusunoki T, Fujiwara R, Murata K, Ikeda K (2009) A giant vocal fold polyp causing dyspnea. Ear Nose & Throat Journal 88(12): 1248-1249.
-
Yiing WC, Abdullah B (2011) Sudden airway obstruction secondary to bilateral vocal cords polyps. Pak J Med Sci 27(3): 699-701.
-
Hausfeld JN, Yanagisawa E, Pensak ML (1983) Sudden airway obstruction due to pedunculated laryngeal polyps. Annals of Otology Rhinology & Laryngology 92(4): 340-343.
-
Tanguay J, Pollanen M (2009) Sudden death by laryngeal polyp: a case report and review of the literature. Forensic Science Medicine and Pathology 5(1): 17-21.
-
Vadodaria B, Cooper C (2001) The anaesthetic management of a case of severe upper airways obstruction due to an enlarging subglottic benign polyp. European journal of anaesthesiology 18(11): 766-769.
-
Sulica L, Behrman A (2003) Management of benign vocal fold lesions: a survey of current opinion and practice. Annals of Otology Rhinology & Laryngology 112(10): 827-833.
-
Cohen SM, Garrett CG (2007) Utility of voice therapy in the management of vocal fold polyps and cysts. Otolaryngology-Head and Neck Surgery 136(5): 742-
-
Klein AM, Lehmann M, Hapner ER, Johns MM (2009) Spontaneous resolution of hemorrhagic polyps of the true vocal fold. Journal of voice 23(1): 132-135.
-
Nakagawa H, Miyamoto M, Kusuyama T, Mori Y, Fukuda H (2012) Resolution of vocal fold polyps with conservative treatment. Journal of voice 26(3): 107-110.
-
Yun YS, Kim MB, Son YI (2007) The effect of vocal hygiene education for patients with vocal polyp. Otolaryngology- Head and Neck Surgery 137(4): 569-575.
-
Watkinson J, Clarke R (2018) Scott-Brown’s otorhinolaryngology and head and neck surgery: In: 8th (Edn.), CRC Press, Boca Raton, USA.
-
Kanaya N, Kawana S, Watanabe H, Niiyama Y, Niiya T, et al. (2000) The utility of three-dimensional computed tomography in unanticipated difficult endotracheal intubation. Anesthesia & Analgesia 91(3): 752-754.
-
Cochet B, Hohl P, Sans M, Cox JN (1980) Asphyxia caused by laryngeal impaction of an esophageal polyp. Archives of Otolaryngology 106(3): 176-178.
-
Hunsaker DH (1994) Anesthesia for microlaryngeal surgery: the case for subglottic jet ventilation. The Laryngoscope 104(S65): 1-30.
-
Tsunoda A, Hatanaka A, Watabiki N, Ishige T, Okamoto M, et al. (2004) Suffocation caused by large vocal cord polyps. American Journal of Emergency Medicine 1(22): 63-64.
-
Ochiai A (2016) Large laryngeal polyp causing airway obstruction. Oxford Medical Case Reports 2016(8): omw050.
-
Hong YT, Yeo CD, Hong KH (2017) Huge Subglottic Polyp Treated with Tracheotomy and Laryngofissure. Journal of The Korean Society of Laryngology Phoniatrics and Logopedics 28(1): 52-54.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?