Congenytal Dacryocele Associated to Intranasal Mucocele: Case Report and Review of the Literature
Congenital dacryocele is a rare clinical entity, which may be associated with intranasal mucocele. We present the case of a female patient, full-term newborn, with a neonatal diagnosis of right congenital dacryocele. She was hospitalized for management of dacryocystitis, with intravenous and topical antibiotics, with good response at the beginning. The imaging study revealed ipsilateral intranasal mucocele. She was evaluated by medical ophthalmology and otorhinolaryngology. Surgical resolution with an endoscopic approach was decided, by resection of the cyst, marsupialization and installation of a silicone probe (Monoka®). The procedure was performed without incident, without recurrence or complications after a six month follow-up. This pathology is described through a review of the literature.
Introduction
Congenital dacryocele represents a rare pathology. Its association with intranasal mucocele has been described. The individual experience of each center is limited, so medical knowledge is based on clinical case reports and small case series, with short-term follow-up.
The objective of this paper is to present a clinical case of congenital dacryocele associated with intranasal mucocele evaluated at Santiago, Chile, along with a review of the literature.
Clinical Report
Newborn full-term Chilean patient, female, with no perinatal history, with a neonatal diagnosis of right congenital dacryocystocele.
She was evaluated at emergency room when she has 6 days of life, due to symptoms characterized by an increase in volume in the right internal canthus, which extends towards the ipsilateral lower eyelid, approximately 2 cm in its greatest diameter, associated with erythema and local temperature (Figure 1). She has no fever or respiratory distress. The rest of the ophthalmological examination was normal. The general status of the patient was evaluated, and no alterations was found.

She was admitted with diagnosis of infected congenital dacryocele. The initial management was therapy with intravenous cloxacillin and cefotaxime, with a favorable initial response. However, on the fourth day of antibiotic treatment, the clinical improvement regressed, with a new increase in volume (Figure 2). It was decided to change the antibiotic scheme to intravenous ampicillin-sulbactam, in association with topical tobramycin and dexamethasone.
She was evaluated by otorhinolaryngology and ophthalmology as a team, and surgical resolution through an endonasal approach was decided.
A Computed Tomography (CT) study of the paranasal cavities was requested, which evidenced the presence of ipsilateral intranasal mucocele (Figure 3).
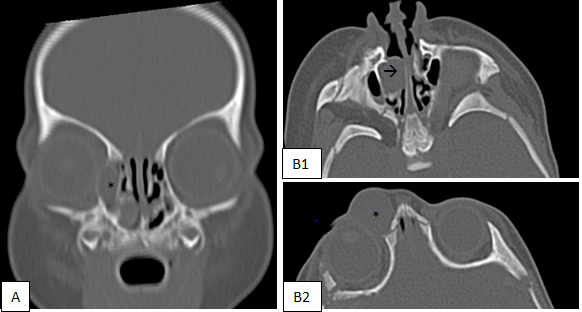
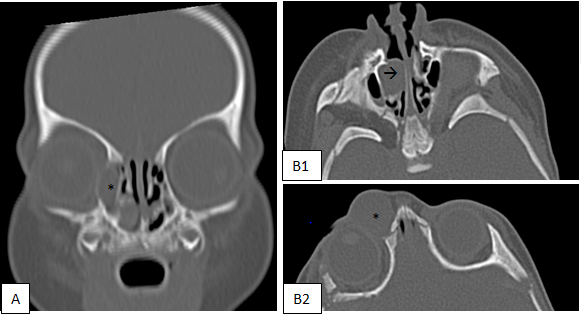
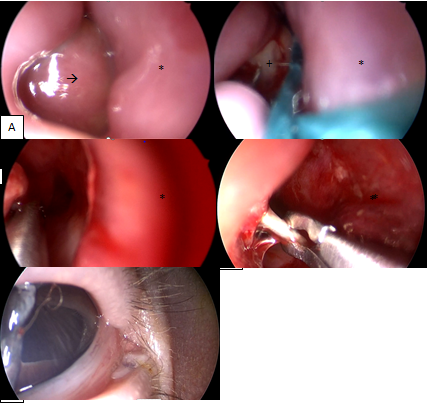
Figure 4: Patient at Operating Room. A. Mass at the Inferior Meatus at the Right Nostril with 0° Endoscopic Vision. B. Opening of the Mass with Pus. C. Resection and Marsupialization of the Medial Wall. D. Intranasal Identification of the Probe. Irrigation was performed. E. Monoka® Properly Installed by O Ophtalmologist at Inferior Canaliculus. * Septum, à Mucocele Intranasal, Inferior to Inferior Turbinate, + Pus.
Under general anesthesia, an increase in volume was observed in relation to the inner canthus of the eye. With an endoscope of 0º and 3 mm, a cystic mass dependent on the inferior meatus was identified at the right nostril. The incision of the endonasal cyst releases pus and serous discharge. Marsupialization, lacrimal duct dilation, and silicone monocanalicular catheter (Monoka®) were installed through the inferior canaliculus without incident (Figure 4).
Due to clinical improvement, medical discharge was decided after the surgery, with oral amoxicillin-clavulanic acid and clinical follow up.
The patient has a great recovery, without recurrence or complications, at six month of follow-up (Figure 5).
Discussion
Congenital obstruction of the nasolacrimal duct affects from 30 to 84% of all newborns. Obstruction can occur at different levels of the nasolacrimal system and is due to multiple causes [1].
Dacryocele is also known as congenital mucocele of the nasolacrimal sac. Is a rare condition. It corresponds to a dilation of the lacrimal sac, which would occur as result of an obstruction of the nasolacrimal duct, both proximal, at the level of the Rosenmuller valve, and distal at the level of the Hassner valve, with consequent accumulation of epidermal debris, mucus, and tears [2].
The prevalence of this pathology is estimated to affect 0.1% of patients with congenital obstruction of the nasolacrimal duct [3]. It is more frequent in the female sex [1, 2, 3]. It usually presents unilaterally, however, it has been observed that up to 25% subsequently manifest contralateral involvement [1, 2, 3].
The main symptom is a blue-pink tumor in the lower part of the medial canthus. The average age of presentation is 7 to 29 days of life. It can manifest with dacryocystitis or preseptal cellulitis, or both, in up to 60% of cases [1, 2, 3, 4]. Even isolated cases of meningitis, sepsis and brain abscesses have been reported. Bacterial infections in neonates can be life-threatening, so a septic condition must always be ruled out, and they usually require admission to the hospital in order to use of intravenous antibiotics. In addition, it can be associated with other manifestations, such as feeding and breathing difficulties. Respiratory complications are present in 22% of unilateral cases and up to 77% of bilateral cases [1].
The differential diagnosis of dacryocele mainly includes meningoencephalocele, capillary hemangioma, dermoid cyst, nasal glioma [2].
Antenatal diagnosis can be made using three- dimensional ultrasound, which allows for early management (Wonf 2015) Bachelard 2013.
Imaging helps differentiate dacryocele from other clinical entities. Study modalities include: ultrasound, CT, Nuclear Magnetic Resonance (MR) and dacryocystography [1].
Ultrasound is a non-invasive method, which does not require sedation. The characteristic findings of a dacryocele include a medial cystic mass communicating with the dilated nasolacrimal duct, with fluid content inside [2].
Pulsation of the mass
Hypertelorism
Associated facial clefting syndrome
Nasal bridge defect
Palpable bony defects
Unusually large lesion
Atypical localization
Known central nervous system abnormlity
Lack of epiphora Table 1: Indication of brain images in patients with dacryocele according ti Paysee, et al [1].
CT helps define the nasal anatomy prior to surgery. In cases of respiratory distress, it makes it possible to exclude other causes, such as choanal atresia [1]. Other indications for requesting neuroimaging in patients with dacryocele are summarized in Table 1.
Nuclear Magnetic Resonance (MR) has the advantage that it does not irradiate the patient, which is especially important at pediatric age [2].
There is a small number of cases reported in the literature of association of intranasal mucocele with dacryocele [1, 2, 3, 4], therefore the relevance of this clinical case. Mucocele corresponds to the intranasal extension of the dacryocele due to progressive filling of the nasolacrimal duct, with consequent prolapse of this and nasal mucosa towards the nasal cavity, at the level of the inferior meatus. Its prevalence is unknown, but it could be present in up to 70% of cases of congenital dacryocele. It may be underestimated if nasal examination is not performed on all patients with dacryocele, [1, 2] therefore always an otolaryngologist consultation must be performed in pediatric patients with dacryocele.
It is important to mention that up to 17% of patients with unilateral dacryocele have bilateral mucocele, which can manifest before or after the dacryocele.1Intranasal mucocele can manifest as snoring or respiratory distress or be a just a finding on examination of the nasal cavity or in imaging studies [3].
The nasal physical examination is essential, with emphasis on the inferior meatus. The search for intranasal mucocele should be bilateral and as a rule in all patients with dacryocystocele, especially in those who present with respiratory distress [2].
Regarding the management of congenital dacryocele, with and without intranasal mucocele, multiple alternatives have been described.
In a series of 17 patients, with a total of 21 dacryoceles, a 76% resolution was obtained with conservative management, which included intravenous antibiotic therapy, local heat, and lacrimal sac massage. However, the remaining 24% evolved with dacryocystitis. This success rate has not been replicated in more recent works, with failure in 76-80% of cases [1, 2, 3].
Probing of the nasolacrimal duct has been shown to be effective in decreasing obstruction. Various models and materials of probes have been used [2, 3].
In this patient, the Monoka® probe was used, which is characterized by be a monocanalicular probe and is the election in pediatric patients of 1 to 2 years with nasolacrimal obstruction that undergo surgery [5].
The presence of concomitant undiagnosed intranasal cyst could be a cause of catheter failure [3].
In those case with associated intranasal mucocele, endoscopic surgical management with extensive marsupialization is recommended [1, 3].
Conclusions
Congenital obstruction of the nasolacrimal duct is a frequent condition in newborns, so as specialists we must be familiar with its multiple causes and its management options. Congenital dacryocele is a rare etiology of the obstruction of the nasolacrimal duct, which can be associated with complications. Its association with intranasal mucocele, such as the one described in this paper, has been reported in the literature.
Due to this association, possible complications, and the therapeutic option, it is advisable to rule out the presence of unilateral or bilateral endonasal mucocele in all patients diagnosed with dacryocele. The study must be complemented with images, being an alternative the CT. Once it is confirmed, definitive management is necessary.
The optimal treatment and timing for it has not been established. Prompt surgical resolution using an endoscopic approach and probing of the nasolacrimal duct with a Monoka® probe is discussed in this publication, with good results in a case with no response to antibiotics.
The evaluation and management of these patients requires timely referral, to be carried out by a multidisciplinary team that includes specialists in ophthalmology, radiology, pediatricians, and otorhinolaryngology.
In rare conditions like this, it is relevant to share the clinical experience in the different centers, to be a contribution to the community of specialists. It would be interesting to carry out a multicenter casuistry, in order to analyze the epidemiological data, management and results.
References
-
Paysse EA, Coats DK, Bernstein JM, Go C, Jong AL (2000) Management and complications of congenital dacryocele with concurrent intranasal mucocele. J AAPOS 4(1): 46- 53.
-
Cavazza S, Laffi GL, Lodi L, Tassinari G, Dall’Olio D (2008) Congenital dacryocystocele: diagnosis and treatment. Acta Otorhinolaryngol Ital 28(6): 298-301.
-
Wong RK, Vander Veen DK (2008) Presentation and management of congenital dacryocystocele. Pediatrics 122(5): e1108-12.
-
Aliseda Pérez de Madrid D (2001) Congenital Obstruction of the Nasolagrimal Duct. In: Toledano Fernandez N (Ed.), Current Management of Nasolacrimal Duct Obstructions. Spanish Society of Ophthalmology pp: 49-64.
-
Rodolfo Nazar S, Galia Gutierrez J, Miguel Leiva F, Romina Gianini V, Rosario Valdés O (2015) Management of lacrimal duct obstruction in children by intubation with Monoka® probe: Initial experience in HCUCh. Rev Fr Otolaryngology Cir Head Neck 75(3): 207-212.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?