An Unusual Presentation of Oil Granuloma in Neck: A Rare Case Report
We introduce a male patient, age 51, with 20 years history of a left sided neck swelling, slowly progressive that was resistant to antibiotic treatment without any history of trauma. The results of the Ultrasound neck and the fine-needle aspiration biopsies were suggestive of epidermal cyst. Histological analysis of an excisional biopsy indicated a haemorrhagic granulation tissue seen with variable sized oil droplets and surrounding foreign body giant cell reactions. In the head and neck, oil granuloma is a fairly uncommon condition that often presents clinically with palpable, painless lymphadenopathy. The etiology of oil granuloma has been described by two mechanisms (1) exogenous foreign body reaction to a lipid or oil-like material and the more uncommon (2) endogenous degeneration related to an allergic/inflammatory mechanism as a result of extreme heat/cold and/or trauma. Oil granuloma has been referred to as lipogranuloma, lipid granuloma, oleogranuloma, paraffin granuloma. Conclusion: This case reports one of the rare clinical findings of primary oil granuloma of the neck without any antecedent cause.
Introduction
Oil granuloma is a soft tissue granulomatous, inflammatory reaction and composed of lipid accumulation and/or a substance that resembles oil. Clinical signs of Oil granuloma may include subcutaneous lumps and palpable lymphadenopathy. There are two theories as to how Oil granuloma develops: either as a foreign-body reaction to a lipid or oil-like substance, or as a result of endogenous lipid degeneration brought on by an allergic reaction and/ or trauma. Although Oil granuloma is well-described in the urological literature, it is quite uncommon to find one in the head and neck, especially when there is no antecedent cause. Oil granuloma has been referred to as lipogranuloma, lipid granuloma, oleogranuloma, paraffin granuloma and even chalazion in orbit [1].
Case History
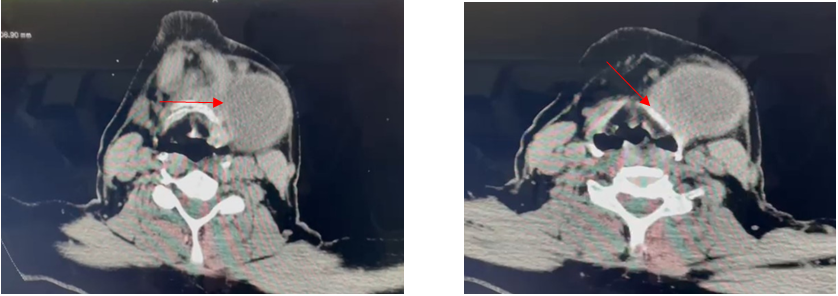
A 51-year-old male patient presented with slowly progressive swelling in the neck for past 20 years, no history of trauma, no history of any injection of oil into the neck without any other comorbidities. Examination findings shows a cystic mass in the left side of the neck of 5x4 cm extending upto the angle of mandible superiorly, medially 2cm from the thyroid notch, laterally upto the anterior border of sternomastoid. Skin over the swelling appeared normal and pinchable (Figure 1). Fine needle aspiration cytology revealed infected epidermal cyst; hence antibiotics were started but patient had no improvement to antibiotics. Ultrasonogram of the neck done and findings were suggestive of epidermal cyst. Contrast Enhanced CT scan of neck was done, which showed the lesion is abutting the hyoid bone (Figure 2A) and seems to be adherent with the thyroid cartilage (Figure 2B). Initially patient was given antibiotics for 2 weeks but with no improvement following which Excisional biopsy was planned under general anaesthesia.
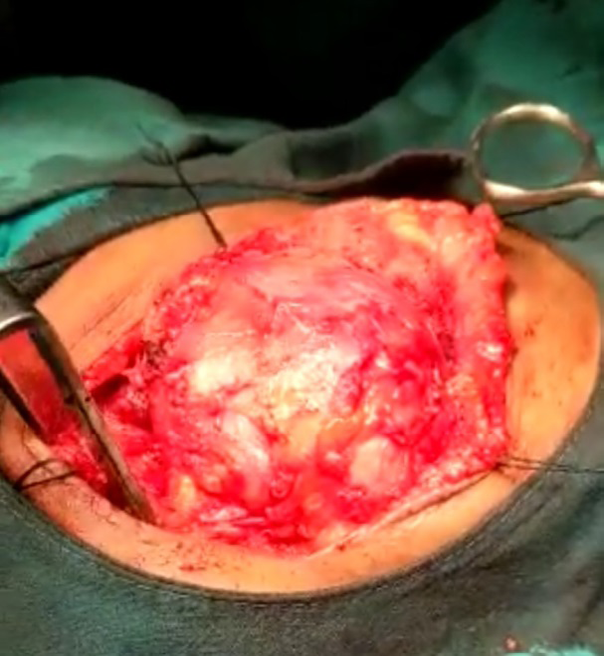
Transverse cervical incision given on left side of the neck 2cm below the angle of mandible, skin, platysma and fatty tissues incised and flap elevated, a yellowish- brown cystic mass of 5x4x2 cm was seen with irregular outer surfaces (Figure 3), the mass had some areas of solid component which was firmly adherent to adjacent submandibular gland and surrounding lymph nodes and fibrofatty tissue. It was also seen firmly attached to anterior strap muscles and thyroid cartilage but we were able to dissect the mass safely without injuring the thyroid cartilage. The total mass along with submandibular gland and surrounding lymph nodes with fibrofatty tissue were excised in-Toto and sent for Histopathology (Figures 4 & 5). Postoperative period was uneventful. Patient was discharged after suture removal on day 7. On follow-up after 2 months the post-operative wound is very healthy (Figure 9) and with no delayed complications.



Final Pathology Report
Gross: Brown coloured soft tissue piece with attached fibrofatty tissue of size 5x4x2 cm. Outer surface is irregular and congested. Cut surface shows cyst like structure which measures 3.5x2 cm.
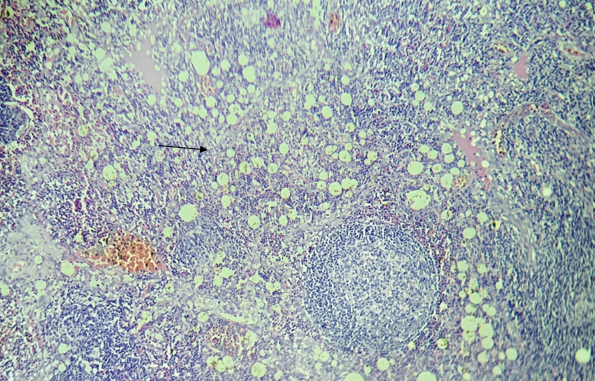
Microscopy: Section shows submandibular salivary glands and two lymph nodes showing reactive follicular hyperplasia. Both lymph nodes show multiple vacuoles (fat/oil droplets). Markedly congested and haemorrhagic granulation tissue seen with variable sized oil droplets and surrounding foreign body giant cell reactions (Figures 6A-8B). Diagnosis - Oil Granuloma.
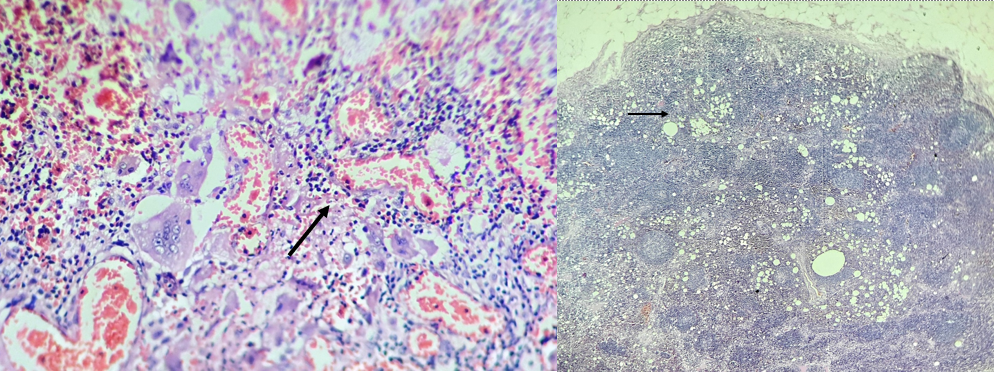
Figure 6A: Arrowhead Showing Foreign Body Giant Cells. Figure 6B: Panoramic View of Submandibular Lymph Node Showing Reactive Follicular Hyperplasia and Multiple Oil Droplets.
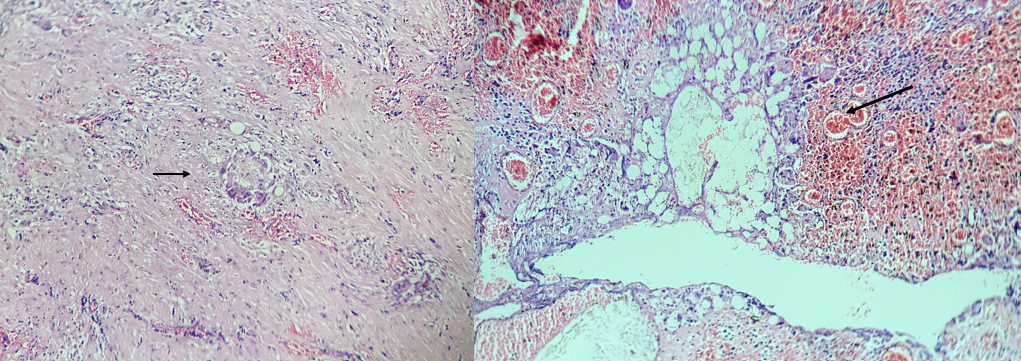
Figure 7A: Extranodal Fibrous Tissue with Foreign Body Granulomatous Reaction against Oil Droplets. Figure 7B: Extranodal Vascularized Soft Tissue with Foreign Body Granulomatous Reaction against Oil Droplets.

Discussion
The clinical manifestation of Oil granuloma, a granulomatous soft tissue reaction involving lipid or oil deposits, generally takes the form of subcutaneous nodules or rubbery lymphadenopathy. Although uncommon, Oil granuloma is frequently mentioned in urologic literature since it most frequently affects genitalia of young adults after receiving injections of foreign substances for penile enlargement, according to Hohaus K, et al. [2]. Only few papers are available in the literature that describe head and neck Oil granulomas. One year after rhinoplasty, Bassichis observed a Oil granuloma on the nasal sidewall that was considered to be caused by petroleum ointment- impregnated postoperative nasal packing [3]. In a similar vein, Guo reported three instances of eyelid Oil granulomas in patients who underwent endoscopic sinus surgery, all of which manifested within a month after the procedure [4]. Rare clinical finding of a patient with Oil granuloma likely secondary to endogenous inflammatory lipid degeneration was described by Fundakowski CE, et al. [5].
For a neck mass, the differential diagnosis is fairly broad. It is crucial to keep in mind that most patients will have some history of lipid deposition when evaluating the diagnosis of lipogranuloma (injection, surgical, traumatic). However, because the initial site of deposition could be in a distinct anatomic region from where the lipogranulomatous lymphadenopathy appears, one must also take lymphatic migration into account. As stated by Peoc’h M, et al. [6] where biopsy not only did not offer a diagnosis but mimicked lymphoma, lipogranuloma may first be mistaken for malignancy and FNA may be of limited help [6].
Periorbital and eyelid Oil granuloma was also been reported after injection of autologous fat [7, 8].
Both external and endogenous processes have been used to describe the pathophysiology of Oil granuloma. The body’s failure to metabolise exogenous oils in the tissue interstitium leads to a foreign body granulomatous reaction, which is the secondary cause of exogenous aetiology. When exposed to extreme heat, cold, or trauma, endogenous aetiology causes an allergic or inflammatory response that result in lipid degradation. Endogenous causes of Oil granuloma are a When endogenous lipid material is found inside a lymph node, it is known as lipogranulomatous lymphadenopathy. According to Hausner, lipogranulomatous lymphadenopathy is characterised by the presence of lipid material in both histiocytes and the extracellular space, giving the cell a vacuolated or foamy appearance. Histological identification of lipid material is based on a distinctive round, empty droplet appearance with pronounced individual droplet size variation (Figures 5 & 6). For confirmation, special lipid stains like Oil-red-O can be used.
The main differential diagnosis for this Oil Granuloma (Lipogranulomatous lymphadenopathy) of neck is same as any other lymphadenopathy of the region. In our case it was a submandibular swelling, with no history of intra swelling injections of oil, no history of implant use, no history of trauma and in both gross and histologic specimen no foreign material seen. As a result, endogenous cause for Oil granuloma with no antecedent cause, probably secondary to lipid degeneration is supported. This is a first report of its kind without any antecedent oil injection or trauma as no such cases have been reported in indexed search of literature.
Conclusion
In the differential diagnosis of a neck mass, Oil Granuloma (lipogranulomatous lymphadenopathy) should be taken into consideration though it is a rare entity and its management. Our goal is that, this report may be useful for Otolaryngologists, Head and Neck surgeons and other clinicians when dealing with a neck mass and their management.
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation (Indian- GCP, ICH-GCP, ICMR guidelines) and with the Helsinki Declaration of 1975, as revised in 2008.
Conflict of Interest: Nil
Financial Support: Nil
References
-
Corcoran ME, Chole RA, Sykes JM, McKennan KX (1996) Ointment granuloma complications after cosmetic and otologic surgery. Otolaryngology Head and Neck Surgery 114(4): 634-638.
-
Hohaus K, Bley B, Köstler E, Schonlebe J, Wollina U (2003) Mineral Oil Granuloma of the Penis. J Eur Acad Dermatol Venereol 17(5): 585-587.
-
Bassichis BA, Thomas JR (2003) Foreign Body Inclusion Cyst Presenting on the Lateral Nasal Sidewall 1 Year after Rhinoplasty. Arch Facial Plast Surg 5(6): 530-532.
-
Guo Y, Peng A, Xie D, Li Y, Ren J, et al. (2007) Diagnosis and Management of Lipogranuloma of the Eyelids from Nasal Endoscopic Surgery. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 21(8): 340-343.
-
Fundakowski CE, Chapman JR, Sargi Z (2013) Lipogranuloma of the Head and Neck. Int Med Case Rep J pp: 1-4.
-
Peoc’h M, Duprez D, Grice G, Fabre-Bocquentin B, Gressin R, et al. (2000) Silicone Lymphadenopathy Mimicking a Lymphoma in a Patient with a Metatarsophalangeal Joint Prosthesis. J Clin Pathol 53: 549-51.
-
Park YR, Choi JA, La TY (2013) Periorbital lipogranuloma after cryopreserved autologous fat injection at forehead: unexpected complication of a popular cosmetic procedure. Can J Ophthalmol 48(6): 166-168.
-
Park JY, Kim N (2016) Periorbital lipogranuloma after facial autologous fat injection and its treatment outcomes. Korean Journal of Ophthalmology 30(1): 10- 16.
- 4th Branchial Cleft Sinus Anomaly Presenting as Recurrent Thyroid Abscess in A Child: A Case Report
- Parotid Duct Injury Repaired Using an Angiocatheter Stent: A Case Report
- Organization and Functionality of the Referral and Counter-Referral System for ENT Disorders in District Hospitals of N’Djamena, Chad: A Cross-Sectional Analytical Study
- Facial Metastases from a Gastrointestinal Stromal Tumor: A Case Report
- Panorama of Ent Cancers and Literature Review: Epidemiological Profile and Therapeutic Management
- Could Antimicrobial Resistance Prove to Be Both a Threat and an Opportunity for us?