How to Address the Health of International Migrants in Latin America? An Evidence-Based Proposal
Introduction: Migration is a recognized social determinant of health. Latin America is one of the regions with the largest human migration. Latin America is now in a position of opportunity to protect the welfare and health of the international migrant population. Objective: The purpose of this paper is to propose a strategy for primary health approach to international migrants in the region of Latin America. This proposed approach is supported on the evidence available at present in the region, particularly in research that has been developed in recent years in Chile. Results: The scientific evidence delivers three central ideas: (i) broad socio-demographic diversity that characterizes the migrant population; (Ii) the centrality of the migration experience and living conditions in Chile as determinants of health of the population; and (iii) the violation of human rights in some groups of international migrants, including the right to social protection in health. With this in mind, an approach strategy focused on the pillars of Social Determinants of Health, Cultural Competence in Health and Human Rights is proposed. Conclusion: The protection of the health of migrant populations is now a priority for Latin America. Its success depends on articulated and sensitive multisectoral efforts, which should aim to create contextualized, effective and evidence-based healthcare services for this population.
Introduction
Migratory movements are as old as man. Since the beginning of human kind, people has moved from one territory to another looking for better hunting, refuge and security for the sustenance of their herd and thus ensure survival [1]. Today, people continue to move around the world [2]. Given the ease of access to information, the progress in communications and the shorter time and cost of transfers, moving from one place to another is Perspective nowadays faster and less expensive than ever before [3]. Various authors and international organizations have developed definitions of international migration, which reaffirms the complexity of the analysis of the migratory phenomenon. The International Organization for Migration, IOM, defines international migration as the movement of people who leave their country of origin or in which they have habitual residence, to settle temporarily or permanently in another country different from their own [4]. These people have had to cross a political border or country for this. The United Nations defines an international migrant, to the person who lives outside his usual place of residence for at least one year [5]. These definitions share to dimensions of relevance, those are the movement between different countries and the intention to reside, permanently or temporarily, in the receiving countries. In all cases, international migration defies our global understanding of social values, cultural norms, economic development, and social inequality. Living in places distant and different to our original location is always challenging, expensive and emotionally daunting. Migration is a recognized social determinant of health in the world [6] and in Latin America [7]. The conditions surrounding the migration process make this population potentially vulnerable and, therefore, human migration can have great impact on public health [8, 9, 10, 11]. Worldwide, it is estimated that there are around 200 million international migrants [2, 5]. Figures from 2011 show that in Latin America and the Caribbean, some 25 million people (around 4% of the total population) had emigrated to another country [4]. In general, the US It is the preferred destination for migrants from Latin America and the Caribbean, and the search for job opportunities is one of the main reasons for these movements. There is also a growing migration within the Latin American region, the so-called South-South migration, especially the movement of people living in less developed countries to closer developed countries within the region [12]. Latin America is one of the regions in the world with the greatest human migration flow. Central America and Mexico are considered one of the largest migratory corridors in the world, with people and communities that migrate for multiple reasons and in different ways, both legal and irregular. In South America, important migratory movements are also present, with extensive South-South and extra-continental migration. This variety of conditions in which migration takes place can generate greater vulnerability for the health and physical and psychological well-being of migrant populations and their families. Health systems are often the first gateway to the formal system of the host society by migrants, and they have the responsibility to address and resolve health and social problems that migrant populations experience.
Purpose of this Essay
The purpose of this document is to propose a health approach for international migrants in the Latin American region. This approach is based on the evidence currently available in the region, particularly on the research that has been carried out in recent years in Chile. This country has received a growing proportion of foreigners in recent years, currently reaching about 6% of the total population (approximately 1 million people). The information that exists today in this country is still incipient, but it allows generating some innovative, integrative and evidence- based proposals.
The Challenge of the Health of International Migrants
There is an urgent need today to define how to address the health of the international migrant population. That is, from what paradigm or perspective should be advanced in the subject of migratory health, a perspective that determines the way of making diagnoses, proposals for intervention, monitoring and monitoring, and even determines how the success or failure of a country in the protection and continuous improvement of the health of the immigrant population. Some classic approaches used in the past have been, for example, interculturality, family health and the life course. These approaches are not antagonistic to each other, and can be combined in practice, but certainly the selection of one over the other will have an impact on the design, implementation and evaluation of the health policy of migrants in any country. In addition to these theoretical proposals, it is necessary to give an account of what the scientific evidence proposes. Currently, quantitative and qualitative evidence in this area has suggested that: • The international migrant population is highly heterogeneous in terms of the country of origin, reasons to migrate, socioeconomic conditions, and health problems [13, 14].
• A low to moderate proportion of the migrant population self-reports as belonging to some indigenous people. In Chile for example, 6% in 2011 and 5.4% in 2013 according to CASEN survey, versus 8.1% in 2011 and 9.2% 2013 in Chilean population according to CASEN survey.
• There is a group of international migrants who do not have any health care provision and they are of urgent attention, especially the group of 0-14 years old. In Chile for example, 8% in the international migrant general population according to CASEN survey 2013 that grew to 22% according to CASEN 2017 [15].
• The main causes of hospital discharges in migrants are birth, external causes / accidents, tumors and digestive system problems [16].
• The health needs perceived by migrants are diverse and vary according to conditions of migratory process and length of residence [7, 17].
• The healthy migrant effect (or bias) (average migrant population with lower self-reported health problems than the Chilean local population) disappears in low socioeconomic migrants, in those who have been in the host country for a long time (e.g. more than 20 years in Chile), and those who come from some more vulnerable countries (e.g. in the case of Latin America Haiti, Bolivia, Ecuador, etc. according to the health condition studied) [18].
• There is a group of international migrants who, consistently over time, are not reached by population surveys or prefer not to report their immigration status in population surveys. In the case of Chile this is clear with the CASEN survey. In this country, those who prefer not to report their migration status tend to report low socioeconomic status, high proportion of children and may represent migrants in an irregular situation [19].
• There is evidence of the importance of recognizing the relationship between territory and health, both in local and international migrant populations. The territory affects the way life goes on, how people interact and how health care develops. The territory is relevant not only at the macro level but especially at the local micro level, including neighbourhoods. In this sense, there are now settlements of particular migrant groups in different locations in every country, which requires a local and culturally relevant territorial approach for migrants from each particular place, which may be very different from other neighbouring or distant areas [20].
• According to the available qualitative evidence, territorial areas that have organized migrant groups and integrated with the local community seem to know better the health system and their rights, as well as they seem to present greater cohesion and social capital, which is known it is an important protector of individual and family health.
• The health of migrants is closely related to their social position, which is manifested through their housing, work and education conditions; as well as its social networks and the spaces available for the construction of cultural identity, participation and social integration [21].
**An Evidence-Based Proposal**
In light of this evidence, it is possible to prioritize some approaches or perspectives to address the health of international migrants in Chile over others. In particular, three ideas are central to this decision: (i) the wide socio-demographic diversity that characterizes the migrant population, with the exception of ethnicity that is relatively low; (ii) the centrality of the migratory experience and living conditions in Chile as determinants of the health of this population; and (iii) the violation of human rights in some vulnerable groups of international migrants, including the right to social protection in health.
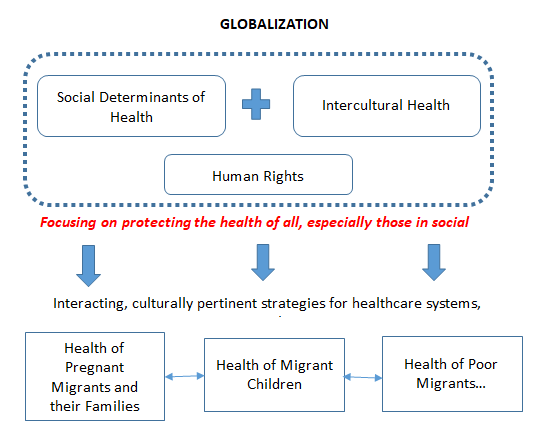
With the foregoing in mind, and from a general frame work of Globalization, the evidence proposes that the perspectives that are considered in the Latin American region to be prioritized are the Social Determinants of Health, Interculturality in Health and Human Rights. A diagram that synthesizes these concepts is presented in Figure 1. Table 1 presents the definitions of each of these concepts. The social determination approach proposes that living and working conditions (including the migration process if you wish to incorporate them) throughout life is the main factor that defines the health of populations.
The intercultural approach in health proposes that the healthcare delivery is a complex human interchange of expectations, beliefs and cultural norms that need to be understood, and that health workers must adapt to experiences and health needs of each client, in such a way that they probe to be culturally pertinent and effectively promote well-being, satisfaction and adherence. This approach is, from its conception, broader than others presented in the literature. It allows incorporating additional visions to some of historical development in Latin America and Chile, such as, for example, the intercultural approach in health that has been dedicated to working on the health of indigenous peoples in the past decades. Finally, the human rights approach is a minimum to be installed on migration issues, given the extensive current evidence of the brutal way in which rights are violated in some groups of migrants, in Chile for example in the case of children, African descendants, people from poorer countries that are often discriminated against, among others.
Human rights
According to Del Toro's multidimensional definition of human rights there are "Three ways to understand human rights: as (i) a normative reference composed of norms or laws that through treaties, pacts, conventions and the constitutions of each country recognize human rights; (ii) an ethical reference, which is made up of the provisions that guide relationships and coexistence among people from a framework of appreciation and respect for others, and (iii) as a utopian reference, which allows us to become aware of the developments that have taken place in the field of human rights and the pending challenges, which lead us to establish a common ideal and to organize ourselves politically with others to advance the breadth and depth of rights. "WHO affirms that" the enjoyment of The maximum degree of health that can be achieved is one of the fundamental rights of every human being ".
The right to health includes timely, acceptable and affordable access to health care services of sufficient quality. The right to health encompasses freedoms and rights. Freedoms include the right of people to control their health and body (for example, sexual and reproductive rights) without interference (for example, torture and non-consensual medical treatments and experiments). Rights include the right of access to a system of health protection that offers all people the same opportunities to enjoy the maximum degree of health that can be achieved.
| Social determinants of health | Social determinants of health are all those social conditions in which people, families and communities live and work and that affect their health. The Social Determinants of Health Model was created by the WHO Commission on Social Determinants of Health (CDSS) and has the following objectives: (i) to clarify the mechanisms through which social determinants generate inequalities in health; (ii) establish the ways in which different determining factors are related; (iii) establish a framework to evaluate the importance of each of them; and (iv) generate a map clearly identifying the places and levels of action and intervention in a population. |
| Social determinants of health | Two relevant concepts associated are: social inequality in health and social inequity in health. Social inequality in health is defined as systematic and structural differences between and within social groups that have some degree of hierarchy or vertical social structure. Social inequality in health is defined as social inequalities that are considered unjust, preventable and modifiable. |
| Intercultural health | Intercultural health: the health care delivery is marked by an intercultural encounter, -a concept coined from the psychotherapeutic experience with migrants -, generated through an intersubjective negotiation in which the foundations, limits and characteristics of the attention among people of diverse cultural trajectories. In addition to the skills of flexibility and adaptation, this concept recalls the importance of considering context, causal conditions, intervening conditions, properties, interaction strategies and their consequences in the creation of this negotiated space of encounter with the other. |
| Intercultural health | Culturally Competent Health Systems: those that recognize and incorporate at all levels, the importance of culture, the evaluation of intercultural relations, the vigilance towards the dynamics of power that result from cultural differences, as well as the knowledge and adaptation of services to meet unique cultural needs. |
| Intercultural health | Cultural Competencies in Health: they have been conceived as capacities of the health team to get to work effectively within the cultural context of the family, the individual, or the community. |
Table 1: Conceptos relacionados a la propuesta de abordaje de salud primaria de migrantes internacionales.
Conclusion
International migration is an opportunity for economic development, cultural and social diversity and wealth, improvement of international relations, and others. However, it is at the same time a huge challenge for integration, the appreciation of diversity and the reduction of social and political gaps that result in poorer population health outcomes. There is today the need to define how to address the health of the international migrant population in Latin America. That is, from what paradigm or perspective should be advanced in the subject of migratory health, a perspective that determines the way healthcare systems make diagnoses, proposals for intervention and monitoring. It also determines how the success a country will be in the protection of social welfare and population health over time.
Protecting the health of migrant populations is now a global priority in public health. It depends on multisectoral and multinational articulated and sensitive efforts, which should aim to generate conditions for providing friendly, contextualized, culturally pertinent, effective and evidence-based services. Improving the health of migrant people and families means contributing to the economic growth, reduction of poverty, social development and human security of all nations, including all countries of Latin America.
Funding
Fondecyt 11130042 "Developing intelligence in primary public health in Chile: a multi-method study" CONICYT, Government of Chile. Award El Mercurio Santander 2017 Scientific research in population health.
References
-
Vásquez R (2009) Impacto de las migraciones en Chile: Nuevos retos para el pediatra. Estamos preparados? Rev chil pediatr 80(2): 161-167.
-
United Nations (2006) Trends in total migrant stock: the 2005 revision. Department of Economic and Social Affairs. Washington DC.
-
Nelson S (2013) Global trends, local impact: the new era of skilled worker migration and the implications for nursing mobility. Nurs Leadersh (Tor Ont) 26 Spec No 2013: 84-88.
-
International Organization for Migration (2012) World Migration report 2011. World Migration report [Internet].
-
United Nations (2003) World Migration Managing Migration - Challenges and Responses for People on the Move.
-
Davies AA, Mosca D, Frattini C (2010) Migration and health service delivery. World Hosp Health Serv 46(3): 5-7.
-
Cabieses B, Pickett KE, Tunstall H (2012) Comparing sociodemographic factors associated with disability between immigrants and the Chilean-born: are there different stories to tell? International journal of environmental research and public health 9(12): 4403-4432.
-
Akhavan S, Bildt C (2004) Health in relation to unemployment and sick leave among immigrants in Sweden from a gender perspective. Ethnicity & health 6(3): 103-118.
-
Alver K, Meyer HE, Falch JA, Sogaard AJ (2005) Bone mineral density in ethnic Norwegians and Pakistani immigrants living in Oslo--The Oslo Health Study. Osteoporos Int 16(6): 623-630.
-
Azerkan F, Zendehdel K, Tillgren P, Faxelid E, Sparen P (2008) Risk of cervical cancer among immigrants by age at immigration and follow-up time in Sweden, from 1968 to 2004. International journal of cancer Journal international du cáncer 123(11): 2664-2670.
-
Beiki O, Allebeck P, Nordqvist T, Moradi T (2009) Cervical, endometrial and ovarian cancers among immigrants in Sweden: importance of age at migration and duration of residence. Eur J Cancer 45(1): 107-118.
-
Alvarado I, Sanchez H (2002) Migration in the Latin America and the Caribbean: A view from the ICFTU/ORIT. Trends in the regions 101-108.
-
Cabieses B, Bustos P (2016) Vulnerabilidad social en salud por parte de migrantes internacionales en Chile. In: Cabieses Bea, [Eds.], Vulnerabilidad social y sus efectos en salud en Chile. Santiago: UDD.
-
Cabieses B, Tunstall H, Pickett KE (2015) Understanding the socioeconomic status of international immigrants in Chile through hierarchical cluster analysis: a population-based study. International Migration Review 52(3): 303- 320.
-
Cabieses B, Tunstall H, Pickett KE, Gideon J (2012) Understanding differences in access and use of healthcare between international immigrants to Chile and the Chilean-born: a repeated cross-sectional population-based study in Chile. International journal for equity in health 11: 68.
-
Oyarte M, Cabieses B, Delgado I (2017) Egresos hospitalarios en Chile: Análisis comparativo entre migrantes internacionales y población local. In: Cabieses B, Bernales M, Chandia S, MacIntyre A, (Eds.), La migración como determinante social de la salud en Chile: miradas y propuestas para políticas públicas. Santiago Chile: Universidad del Desarrollo.
-
Bernales M, Cabieses B, MacIntyre A, Chepo M (2016) Población migrante internacional en Chile: desafíos pendientes percibidos por los trabajadores de Atención Primaria. Medwave 16(Suppl 6): e6759.
-
Cabieses B, Tunstall H, Pickett K (2013) Testing the Latino paradox in Latin America: a population-based study of Intra-regional immigrants in Chile. Revista medica de Chil 141(10): 1255-1265.
-
Cabieses B, Pickett KE, Tunstall H (2012) What are the living conditions and health status of those who don't report their migration status? A population- based study in Chile. BMC public health 12: 1013.
-
Vasquez A, Cabieses B, Tunstall H (2016) Where Are Socioeconomically Deprived Immigrants Located in Chile? A Spatial Analysis of Census Data Using an Index of Multiple Deprivation from the Last Three Decades (1992-2012). PloS one 11(1): e0146047.
-
Cabieses B (2014) La Compleja Relación Entre Posición Socioeconómica, Estatus Migratorio y Resultados de Salud. Value in Health Regional Issues 1(5): 1-6.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines