Health System Resilience in a PHC Setting in India—A study of Assam and MP
Context: To bolster the ambitious Program of Government of India (GOI), to build a strong and resilient healthcare system plans to establish 1,50,000 Health and Wellness Centres (HWCs) across the country by 2024, the GOI gave a clear to its partners to explore options. Aim: Therefore, LEHS | WISH, initiated a baseline study to assess the service availability and service readiness (SARA) status of 18 Sub-centres (SCs) and Primary Health Centres (PHCs) to be upgraded as HWCs to deliver the twelve package of services as envisaged in HWC guidelines to strengthen the primary healthcare system. Settings and Design: Health system resilience, was assessed against the 10 Areas of Concern, elaborated in National Quality Assurance Standards (NQAS) for all the 12 thematic areas of service delivery of HWCs. Methods and Material: A sequential mixed method of design was adopted, which included both quantitative and qualitative components of assessment. The major focus of the study was quantitative in nature to assess HWC facility level gaps across key areas. Qualitative study with stakeholders including that of the community was undertaken to elicit reasons for such gaps and awareness of the community to respond/ engage with health systems better. Statistical Analysis Used: STATA was used a quantitative analysis tool undertake the analysis. Results: on average, both the last mile healthcare delivery system (PHC and SC) and the community are less than 25% resilient, even for disasters. Conclusion: It is not possible to make the system resilient unless focused effort is made. Therefore, there’s a need to clearly define the essential services and its resource requirement to be made available 24X7 for 365 days without fail, offer regular training to the staff to ensure process resilience, create awareness within the community to engage with the health system optimally, strengthen local governance to assure provision of essential services.
Introduction
To bolster the ambitious Program of Government of India (GOI), of establishing 1,50,000 Health and Wellness Centres (HWCs) across the country by 2022, the GOI gave a clear to its partners to explore options. The LEHS | WISH therefore initiated a baseline study to assess the service availability and service readiness (SARA) status of 18 Sub-centres (SCs) and Primary Health Centres (PHCs) to be upgraded as HWCs to deliver the twelve package of services as envisaged in HWC guidelines to strengthen the primary healthcare system (Box 1).
Post COVID, the definition “Health system” as “ensemble of all public and private organizations, institutions, and resources mandated to improve, maintain or restore health”, has taken a wider connotation in include “Resilience”. Thus the term “Health System Resilience” means sustenance of baseline levels and quality of routine healthcare, including removal of barriers to accessing care; access to flexible financing, clear governance, and coordination structures; availability of surge capacity for maintaining quality care; access to sufficient quantity and quality of medical supplies, workforce; and commitment to continuous quality improvement. Further, community awareness and it participation in the facility is important for ensuring health system resilience. Therefore, adequate and appropriate awareness generation must be ensured to enhance the opportunities for resilience. This entails a system-wide and multi-sectoral input with proportionate prioritization of individual and population-based health services; attaching due attention on one hand to the usual tenants and determinants of health, equity, and quality; and on the other proactive attention and response-focused measures against public health challenges to from prevention to preparedness, and response to recovery [1].
Aim
Therefore, the LEHS | WISH used this opportunity to assess the existing PHCs and SCs to be developed as HWCs using an integrated and holistic approach to building a resilient and strong health system. Objectives Therefore, the study objectives used the following characteristics of Health System Resilience as laid down by WHO to assess the 18 study facilities:
- System is aware of its own strengths and vulnerabilities related to health system components and linkages to wider society;
- Addresses a wide range of health system challenges and population health problems, i.e 12 packages of services under the HWC guidelines as laid down by the government of India;
- Improves health systems’ functioning to protect population health during public health crises;
- Maintains core health system functions to protect population health while effectively responding to public health crises;
- Learns from crises and other public health events to transform themselves and improve the functions of promoting and protecting population health;
- Integrates various actors and their actions in a coordinated fashion for positive health outcomes;
- Brings dividends to positive health outcomes in both everyday settings and extreme events.
Approach and Methodology
The health system resilience, therefore, evaluated the internal strengths and weaknesses of the system using the 10 Areas of Concern, elaborated in National Quality Assurance Standards (NQAS) for all the 12 thematic areas of service delivery of HWCs in both the states of Assam and Madhya Pradesh (Box 2). The scope of the study included a total of 18 facilities, which included 10 tea Garden facilities in Assam (6 PHC level and 4 SC level); and 8 government facilities in Madhya Pradesh (MP); which included 3 SCs and 5 PHCs. This apart, a qualitative study was undertaken with 38 service providers (19 in each State-Medical Officers, Nurses, Pharmacists, and ward boys) and 1084, and 868 community members each across the catchment areas of the hospitals across Assam
and MO respectively to understand their knowledge attitude and practices around seeking care and extending assistance during disasters [2, 3]. A comprehensive checklist was deployed for assessing the PHCs/SCs for their resilience. The assessment tool deployed in all the facilities was designed with various checkpoints of NQAS guidelines (referred as 10 different Areas of Concern) as base for assessment. Further, relevant checkpoints from the WHO Hospital Emergency Response Checklist, 2011; National Disaster Response & Management Guidelines (NDRM), Hospital Disaster Management Guidelines (DHS, Kerela), 2018 were added to the NQAS Checklist to make it more comprehensive tool for assessment [4]. Health Systems Resilience apart, special focus was laid on Disaster Resilience. The reality check that happened on the extent of preparedness across levels of hospitals and support desired from community during the COVID pandemic has clearly chartered the need to prepare the system to such challenges in future [5].
Results
The comprehensive checklist was deployed for assessing the PHCs/SCs for their resilience. The assessment tool deployed in all the facilities, was designed with various checkpoints of NQAS guidelines(referred as 10 different Areas of Concern) as base for assessment. Further, relevant checkpoints from the WHO Hospital Emergency Response Checklist, 2011; Hospital Disaster Management Guidelines (DHS, Kerela), 2018 were added to the NQAS Checklist to make it more comprehensive tool for assessment. The key findings of the assessment revealed that:
Health System Resilience
A. Command Centre
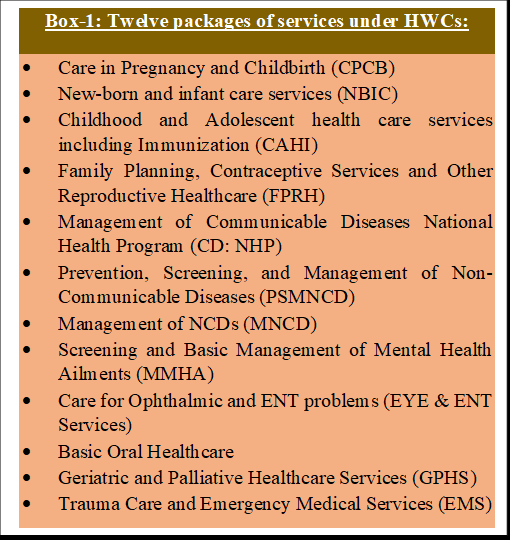
- 10% facilities in Assam and 37.5% facilities in MP, had documented SOP/Protocol for operationalizing/ activating an emergency plan.
- 20% staff of Assam’s facilities and 87.5% staff of MP’s facilities, had been adequately trained and were aware of the emergency responses & job responsibilities during outbreaks.
B. Communication with Relevant Authorities and
- 50% of facilities of Assam and 75% of facilities of MP, had a designated nodal person from the PHC who communicated with Block & District Health authorities during emergency response.
- 50% of facilities in Assam and 25% of facilities in MP, had IEC Materials for dissemination of key messages to the target audience (the patients, staff, public) in preparation for emergency response.
C. Safety and Security of the Staff, Patients, and Public • 20% of facilities in Assam and 75% of facilities in MP, presented with a procedure for stepping up security needs at special areas like entry/exits, food/water access points, pharmaceutical stockpiles, parking area, and the PHC backyard.
D. Triage
- 10% of facilities of Assam and 0% facility of MP, had a designated covered area (triage area).
- 20% of facilities in Assam and 25% of facilities in MP, had an SOP/protocol for discharging/referring patients.
E. Surge Capacity
- None of facilities in Assam and 12.5% of facilities in MP, had SOP available to handle or calculate extra need for an increased patient load during emergency.
- No facilities of Assam and 12.5% facilities of MP, had oxygen supply available for handling medical emergencies for any increase in patient load.
- 40% of the pharmacists/ MOs of Assam’s facilities and 87.5% of pharmacists/ MOs of MP were aware of a method to forecast medication.
F. Human Resource • Only 12.5% of facilities in Assam, and 50% in MP had alternative arrangements for managing the sick/injured staff/dependents of staff.
G. Logistics and Supply Management • Most supplies in both states for equipment, medicines, and consumables are handled by state supplies. However, in Assam tea garden facilities supplies are routed through tea garden management upon request raised to the state health department. The supplies are a part of the planned budget, and all facilities in both states had most of the equipment and supplies for the level of care they offer. Further, in the eventuality of a shortage, the stock- out of essential drugs is handled at local levels through local purchases from approved vendors; and patients are not asked to spend out-of-pocket for the same.
H. Infection Control All the facilities of Assam, and MP as far as infection control is concerned practice only hand washing, use Personal Protective Equipment, and follow standard rules laid down by the Government of India for Bio- Medical Waste Management and Handling. This includes the provision of color-coded bins with linings for the segregation of waste at the source of generation. However, in Assam and MP, most of the SCs did not have Sharp’s container, disinfectants, and auto-disable syringes as infection prevention, and control measures. • Most facilities in MP and a few in Assam have outsourced their final disposal of sharp wastes and incineration of infected wastes as per the national guidelines. Two facilities in Assam dumped their wastes on flat ground or in open pits and practiced open burning of infected waste in the pit. All the facilities of Assam and MP have a biomedical waste storage room.
I. Fire Safety-) • None of the facilities had provision for a firefighting system, nor the teams were aware of mitigation measures in such an eventuality to douche the fire. Several facilities lacked adequate firefighting equipment.
Disaster Resilience
As regards disaster resilience, the study findings indicate that the assessed facilities, are not adequately prepared to handle disasters, particularly pandemics. The qualitative interview (Figure 1) reflected that none of the facilities complied with the expected level of disaster reliance. The tea garden hospitals in Assam were found to be completely unprepared for handling disasters. On the other hand, all the HWCs in MP were aware and relatively better prepared, which could be attributed to state-level referral practices and interventions from the government in terms of training and capacity building of staff. Over 80% of the staff in Assam were untrained to manage emergencies and disasters. However, approximately 60% of the staff responded that they had adequate experience to estimate the requirements for handling disasters and were aware of how to source necessary resources (Figure 2).
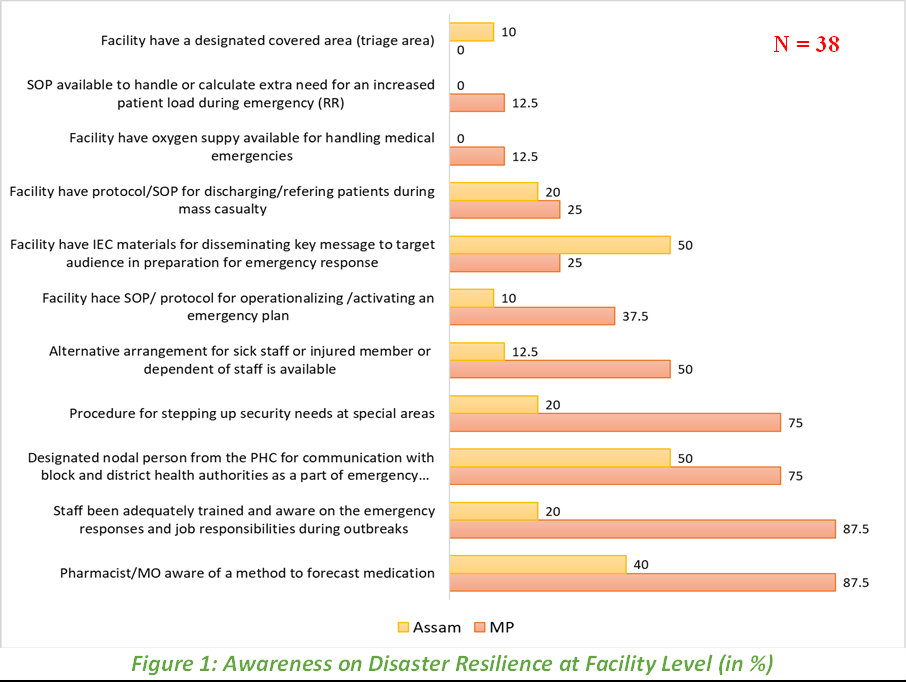
In contrast, in MP, the level of untrained staff was much lower at 12.5%, meaning 87.5% had received requisite training for disaster management. Additionally, a significant percentage (80%) of the staff in MP were aware of how to respond to emergencies and make estimates on resource requirements during disasters.
Community Level - Disaster Resilience
The analysis of disaster resilience at the community level revealed low levels of awareness about disaster management in both Assam and MP. Only 1.5% of members in the tea garden community in Assam and 4.92% of community members in MP reported having awareness about disaster management. In total, across both states, only 3.23% of the population demonstrated awareness regarding disaster management. However, there was a significant difference in the percentage of community members who had received training on disaster management. In MP, 37.50% of community members (48 individuals) reported receiving training, while in Assam, a higher percentage of community members, 86.87% (15 individuals), mentioned having received training.
The analysis also highlights that the state government and NGOs were the most common organizations providing training on disaster management in both Assam and MP. These organizations play a crucial role in building community resilience and enhancing awareness and preparedness for disasters.
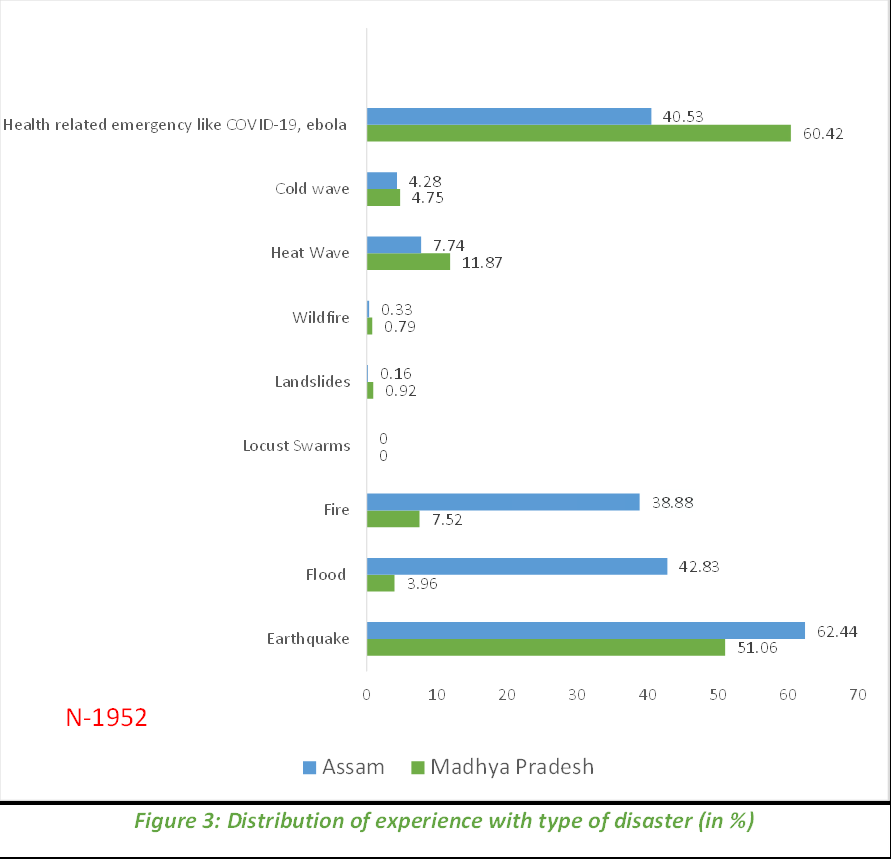
Community Level – Awareness
The common types of disasters that the community is aware of are COVID, earthquakes, health waves, fire and cold wave in that descending order (Figure 3).
Discussion
The findings reveal that the PHCs and SCs that provide last-mile care to the population are less than 25% ready in terms of their ability to respond to the demand surges during routine and of course disasters. Even as the PHCs will be converted as HWCs, it is not possible to make the system resilient unless focused effort is made to make the system. This calls for:
- Clearly defining what services and its resources/ infrastructure should be considered as essential, and therefore, should be made available 24X7 for 365 days without fail. For instance, in a PHC availability of one doctor, one nurse, and one paramedic is most critical to ensure the system stays resilient. Similarly, vital drugs and equipment should be clearly defined and maintained. The national guidelines for essentials of HWCs are clearly defined and hence need to be fully complied with to ensure reliance on the system.
- Offering regular training to the staff to ensure process resilience.
- Creating awareness within the community to support the health system to optimally respond to the requirements of the community, especially during disasters; so that lives can be saved.
- Finally, local governance be strengthened to assure provision of essential services in the facilities for the population. References
1. National Health Systems Resource Centre (2015) Technical Support Institute with National Health Mission.
2. World Health Organisation (2011) WHO Hospital Emergency Response Checklist.
3. (2018) Hospital Disaster Management Guidelines. DHS Kerala.
4. Sahu S, Syed A, Verma P, Singh RR, Nagarajan S, et al.
(2023) Role of prescription practice in ensuring patient safety in the primary health care Settings in India. Indian J Public Health 67(1): 162-5.
5. Das AK, Nagarajan S, Bhargava R, Singh RR, Srivastava
AD (2020) Factors Impacting Prescription Practice in Primary Healthcare Setting in India: A Case Study in Rajasthan. Medrxiv.
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal
- Biological Efficacy of an Adulticide Mixture (clothianidin + deltamethrin) as an Indoor Residual Spray against Adult Anopheles flavirostris in Palawan, the Philippines