Association of Shift Pattern and Shift Duration with Burnout among Healthcare Technologists Working in Emergency and Intensive Care Units: A Comparative Cross-Sectional Study
Background: Healthcare technologists working in the emergency department (ED) and intensive care unit (ICU) experience substantial occupational stressors associated with burnout. Prolonged irregular shift patterns and shift durations may exacerbate burnout. This study aimed to examine the association of shift pattern and shift duration with burnout among healthcare technologists. Material & Methods: A comparative cross-sectional study was conducted from December 2024 to June 2025 at tertiarycare public and private hospitals of Islamabad, Pakistan. Stratified random sampling was used to recruit 278 healthcare technologists working in the ED and ICU of selected hospitals. A structured data collection form and the Maslach Burnout Inventory-Human Services Survey (MBI-HSS) were used for data collection. Descriptive statistics, group comparison tests using the chi-square test, correlation analysis, and multiple linear regression were performed. Results: The majority (63.3%) of participants with emotional exhaustion (EE) reported moderate burnout, whereas burnout was significantly higher (74.1%) among those with depersonalization (DP), and most participants had low personal accomplishment (PA) (92.8%), indicating reduced professional fulfillment. There were significant correlations between shift patterns and emotional exhaustion (p = 0.003), with higher burnout levels among permanent night shift workers. EE was positively correlated with the length of shifts (r = 0.132, p = 0.028). ICU technologists had significantly higher DP than ED technologists (p = 0.018). Conclusions: The findings indicate a high burden of burnout-related symptoms among Pakistani healthcare technologists working in ED and ICU settings. Organizational factors, particularly shift pattern, shift duration, and department, were more consistently associated with burnout dimensions than sociodemographic factors.
Abbreviations
ED: Emergency Department; ICU: Intensive Care Unit; EE: Emotional Exhaustion; DP: Depersonalization; MBI-HSS: Maslach Burnout Inventory-Human Services Survey; PA: Personal Accomplishment; EE: Emotional Exhaustion.
Introduction
Burnout is a work-related syndrome characterized by emotional exhaustion, depersonalization, and reduced personal accomplishment resulting from chronic occupational stress. It is aggravated by continued exposure to traumatic incidents, insufficient staffing, and unmanaged work schedules, which may lead to dissatisfaction with the job, absenteeism, and turnover. The impact of shift patterns on burnout varies depending on individual and institutional factors such as age, experience, and workload [1, 2]. In healthcare settings, burnout is a substantial occupational health concern and has become a pressing concern among healthcare technologists. It has important consequences, including reduced patient safety, increased medical errors, and greater staff turnover, which in turn burdens the healthcare systems [2, 3]. Furthermore, the effects of shift patterns on burnout may vary among ED and ICU settings, which have distinct patient populations, workflows, and staffing models [4]. The different duty hour shift patterns in place significantly influence the risks of burnout among medical practitioners. Irregular working hours, including rotating shifts, night shifts, and prolonged duty hours, disrupt circadian rhythms and wakefulness, contributing to chronic fatigue that impairs cognitive functioning from operating well.
Shift work affects social and personal life as well, in that healthcare technologists may experience reduced social and family engagement. Social isolation heightens psychological stress, which increases the risk of burnout [6]. Besides, longer shifts, when combined with insufficient time for recovery, increase physical and emotional exhaustion, thus harming performance and well-being [7]. Individual factors such as age, experience, and resilience, and institutional factors like workload and staffing levels, also influence the relationship between shift patterns and burnout. For instance, irregular schedules may be exceptionally challenging to younger or less-experienced healthcare technologists, while heavy workloads due to inadequate staffing levels increase stress and, consequently, lead to burnout [8]. Organizational culture and resource differences between public and private healthcare systems also influence variations in the impact of shift patterns on levels of burnout among professionals [9].
Medical technologists work in high-stress environments in both EDs and ICUs, requiring sustained emotional resilience and cognitive focus. Such chronic exposure to stressors precipitates emotional exhaustion, which is a primary dimension of burnout characterized by feelings of fatigue and depletion of emotional resources [3]. The other two dimensions include depersonalization, which is detachment from patients and colleagues, and diminished personal accomplishment, reflecting feelings of reduced professional efficacy and satisfaction, thereby reinforcing the burnout cycle [10]. Despite the consequences of this issue, most prior research has focused primarily on physicians and nurses, with less attention to healthcare technologists [11]. Other studies have been conducted in single-site settings, ignoring the probable differences in shift patterns and levels of burnout across different health systems [9]. Therefore, the multi-site quantitative study aims to assess the association of shift patterns and shift duration with burnout among ER and ICU healthcare technologists across multiple healthcare settings. The study may inform evidence-based recommendations for shift scheduling and staff support to mitigate the stressors and enhance well-being and job satisfaction among healthcare technologists, ultimately improving patient care and workforce sustainability in ED and ICU settings.
Methodology
The multicenter cross-sectional comparative study was conducted after approval from the ethical review board committee of Health Services Academy, Islamabad, Pakistan (Ref. No: 000713/HSA/MSPH-2023) to assess burnout levels among healthcare technologists working under different shift patterns. The study was performed in accordance with the ethical standards set out in the 1964 Declaration of Helsinki. The study was carried out in public and private tertiary care hospitals in Rawalpindi, Pakistan, from December 2024 to June 2025. The primary data were collected using the Maslach Burnout Inventory-Human Services Survey (MBI- HSS). The questionnaires were administered to ED and ICU healthcare technologists for direct measurement of burnout levels after explaining the purpose of the study and obtaining informed written consent.
The study employed a stratified random sampling technique. Within each stratum, participants were selected using simple random sampling. The sampling frame was stratified by hospital type, department, and shift pattern. The population of interest includes healthcare technologists working in the ED and ICU. Strata were defined by hospital type (public/private), department (ED/ICU), and shift pattern (day, rotating, permanent night). Proportional allocation was used. After identifying the relevant strata, a random sample was used to select individuals within each group.
Based on an estimated population of healthcare technologists in the study area, the sample size was calculated using the OpenEpi calculator with 95% confidence interval and 5% margin of error, resulting in a required sample size of 278 participants to ensure adequate statistical power and generalizability. The healthcare technologists, who had been working in their current department for at least 6 months in the ED or ICU, were included in this study, while administrative staff, interns or trainees, staff on prolonged leave, and incomplete questionnaires were excluded.
A structured questionnaire was used to collect sociodemographic and occupational data, alongside the MBI-HSS. MBI-HSS assesses burnout in three dimensions: Emotional Exhaustion (EE), which measures feelings of emotional depletion and fatigue, Depersonalization (DP), which assesses detachment and impersonal responses toward patients, and Personal Accomplishment (PA), which evaluates feelings of competence and achievement. The instrument consists of 22 items, and each item was rated on a 7-point Likert scale (0 = Never to 6 = Every day). Higher scores on EE and DP indicate higher burnout, whereas lower scores on PA indicate higher burnout [3].
The tertiary care hospitals were visited personally after institutional permission to distribute and collect data on a paper questionnaire. Data were analyzed in SPSS version 27. Descriptive statistics summarized participant characteristics and burnout scores in numbers and percentages. Associations between categorical variables were examined using chi-square or Fisher’s exact test, as appropriate. Spearman’s correlation and multiple linear regression were used to evaluate associations between workplace factors and burnout dimensions. A two-sided P-value <0.05 was considered statistically significant.
Results
Maslach Burnout Inventory-Human Services Survey
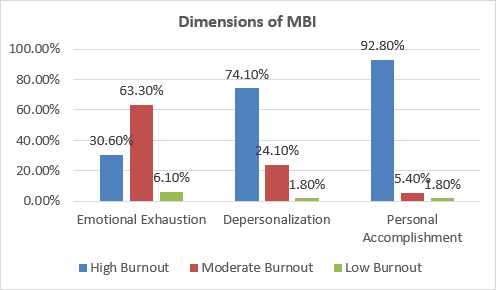
The study found different levels of burnout on the three dimensions (Figure 1). The majority (63.3%) of participants in EE expressed moderate burnout, with 30.6% expressing high burnout, and only 6.1% having low burnout. In DP, burnout was significantly higher: 74.1% of participants were in the high burnout category, 24.1% were in the moderate burnout category, and only 1.8% were in the low burnout category. Most participants (92.8%) had low personal accomplishment, indicating reduced professional fulfillment, whereas 5.4% and 1.8% of the participants comprised moderate and low burnout groups, respectively.
Association of Shift Pattern and Shift Duration with Burnout Levels in Hospital Settings
Emotional Exhaustion (EE)
The analysis in Table 2 indicates that emotional exhaustion (EE) among healthcare technologists was not significantly influenced by department (emergency vs. ICU) or shift length, suggesting that working in high-acuity units or longer shifts alone did not determine EE levels. However, the shift pattern showed a significant association with EE (p = 0.003), with permanent night and rotating shifts exhibiting higher levels of emotional exhaustion compared to day/evening shifts. This suggests that non-traditional work schedules, particularly night and rotating shifts, may contribute more to emotional fatigue, likely due to circadian disruption, sleep disturbances, and increased work stress.
| Distribution | Emotional Exhaustion (EE) | Total | p Value | |||
|---|---|---|---|---|---|---|
| Low EE | Moderate EE | High EE | ||||
| Department | Emergency | 8 (2.9%) | 84 (30.2%) | 39 (14.0%) | 131 (47.1%) | 0.962 |
| Department | ICU | 9 (3.2%) | 92 (33.1%) | 46 (16.5%) | 147 (52.9%) | 0.962 |
| Shift Length | <8 hrs | 7 (2.5%) | 70 (25.2%) | 21 (7.6%) | 98 (35.5%) | 0.112 |
| Shift Length | 8-12 hrs | 7 (2.5%) | 54 (19.4%) | 34 (12.2%) | 95 (34.2%) | 0.112 |
| Shift Length | >12 hrs | 3 (1.1%) | 52 (18.7%) | 30 (10.8%) | 85 (30.6%) | 0.112 |
| Shift Pattern | Day only (including evening) | 1 (0.4%) | 51 (18.3%) | 34 (12.2%) | 86 (30.9%) | 0.003 |
| Shift Pattern | Rotating (including Night) | 11 (4.0%) | 52 (18.7%) | 29 (10.4%) | 92 (33.1%) | 0.003 |
| Shift Pattern | Permanent Night | 5 (1.8%) | 73 (26.3%) | 22 (7.9%) | 100 (36.0%) | 0.003 |
Table 2: Association of Emotional Exhaustion with Work-Related Variables (n = 278).
Depersonalization (DP)
Table 3 demonstrates DP association with work-related variables. DP levels differed significantly by department (p = 0.015), with ICU staff showing higher proportions of high DP (41.7%) compared to emergency department staff (32.4%).
DP was not significantly associated with shift length or shift pattern (p > 0.05 for both). Overall, ICU work appears to be the key factor linked to higher depersonalization among healthcare technologists, likely reflecting the intense and emotionally demanding nature of critical care environments.
| Distribution | Depersonalization (DP) | Total | p value | |||
|---|---|---|---|---|---|---|
| Low DP | Moderate DP | High DP | ||||
| Department | Emergency | 5 (1.8%) | 36 (12.9%) | 90 (32.4%) | 131 (47.1%) | 0.015 |
| Department | ICU | 0 (0.0%) | 31 (11.2%) | 116 (41.7%) | 147 (52.9%) | 0.015 |
| Shift Length | <8 hrs | 1 (0.4%) | 24 (8.6%) | 73 (26.3%) | 98 (35.3%) | 0.4 |
| Shift Length | 8-12 hrs | 4 (1.4%) | 23 (8.3%) | 68 (24.5%) | 95 (34.2%) | 0.4 |
| Shift Length | >12 hrs | 0 (0.0%) | 20 (7.2%) | 65 (23.4%) | 85 (30.6%) | 0.4 |
| Shift Pattern | Day only (including evening) | 2 (0.7%) | 25 (9.0%) | 59 (21.2%) | 86 (30.9%) | 0.645 |
| Shift Pattern | Rotating (including Night) | 2 (0.7%) | 21 (7.6%) | 69 (24.8%) | 92 (33.1%) | 0.645 |
| Shift Pattern | Permanent Night | 1 (0.4%) | 21 (7.6%) | 78 (28.1%) | 100 (36.0%) | 0.645 |
Table 3: Association of Depersonalization with Work-Related Variables (n = 278)
Personal Accomplishment (PA)
The prevalence of PA scores across work-related variables was examined in Table 4. High levels of personal accomplishment were reported by the majority of healthcare technologists across departments, shift lengths, and shift patterns, with no significant differences observed (p > 0.05 for all). Specifically, 44.6% of emergency staff and 48.2% of ICU staff reported high PA, while moderate and low PA were rare. Similarly, shift duration and work schedule had minimal impact on PA. This suggests that, despite the demanding critical care environment and long or non-traditional shifts, most healthcare technologists maintain a strong sense of achievement and professional efficacy.
| Distribution | Personal Accomplishment (PA) | Total | P-Value | |||
|---|---|---|---|---|---|---|
| High PA | Moderate PA | |||||
| Department | Emergency | 124 (44.6%) | 4 (1.4%) | 3 (1.1%) | 131 (47.1%) | 0.206 |
| Department | ICU | 134 (48.2%) | 11 (4.0%) | 2 (0.7%) | 147 (52.9%) | 0.206 |
| Shift Length | <8 hrs | 91 (32.4%) | 7 (2.5%) | 0 (0.0%) | 98 (35.3%) | 0.21 |
| Shift Length | 8-12 hrs | 90 (32.4%) | 2 (0.7%) | 3 (1.1%) | 95 (34.2%) | 0.21 |
| Shift Length | >12 hrs | 77 (27.7%) | 6 (2.2%) | 2 (0.7%) | 85 (30.6%) | 0.21 |
| Shift Pattern | Day only (including evening) | 80 (28.8%) | 6 (2.2%) | 0 (0.0%) | 86 (30.9%) | 0.545 |
| Shift Pattern | Rotating (including Night) | 85 (30.6%) | 4 (1.4%) | 3 (1.1%) | 92 (33.1%) | 0.545 |
| Shift Pattern | Permanent Night | 93 (33.5%) | 5 (1.8%) | 2 (0.7%) | 100 (36.0%) | 0.545 |
Table 4: Association of Personal Accomplishment with Work-Related Variables (n = 278).
Correlation Matrix of Burnout Dimensions
Correlation Analysis: Department, Shift Length, Shift Pattern, Burnout Correlation In Table 5, correlation analysis revealed significant relationships between work-related factors and burnout dimensions. Department was significantly associated with shift length (p = 0.043) and DP (p = 0.037), indicating that ICU staff, compared to emergency staff, experienced longer shifts and higher DP. Shift length showed a significant positive correlation with EE (p = 0.028), suggesting that longer working hours contribute to higher EE. Similarly, shift pattern was significantly correlated with EE (p = 0.009), reflecting increased emotional exhaustion among staff on rotating or permanent night shifts. No significant correlations were observed between PA and any work-related factors, indicating that sense of professional achievement remains stable regardless of department, shift length, or shift pattern. Overall, these findings highlight that EE is particularly sensitive to shift-related factors, DP is influenced by departmental assignment, and PA is largely unaffected by work conditions.
| Department | Shift Length | Shift Pattern | EE | DP | PA | |
|---|---|---|---|---|---|---|
| Department | . | 0.043 | 0.495 | 0.81 | 0.04 | 0.28 |
| Shift Length | 0.043 | . | 0.798 | 0.03 | 0.78 | 0.57 |
| Shift Pattern | 0.495 | 0.798 | . | 0.01 | 0.14 | 0.98 |
| EE | 0.81 | 0.028 | 0.009 | . | 0.3 | 0.29 |
| DP | 0.037 | 0.776 | 0.144 | 0.3 | . | 0.24 |
| PA | 0.28 | 0.568 | 0.977 | 0.29 | 0.24 | . |
Table 5: Spearman’s Correlation of Department, Shift Characteristics, and Burnout Dimensions (n = 278) Table 5: Spearman’s Correl
Table 5: Spearman’s Correlation of Department, Shift Characteristics, and Burnout Dimensions (n = 278) Table 5: Spearman’s Correlation of Department, Shift Characteristics, and Burnout Dimensions (n = 278) Abbreviations: EE: Emotional Exhaustion, DP: Depersonalization, PA: Personal Accomplishment Predictors of Burnout Dimensions (Multiple Linear Regression) In Table 6, multiple linear regression analysis was performed to identify workplace factors predicting burnout dimensions among healthcare technologists (n = 278). For emotional exhaustion (EE), both shift length (B = 0.087, p = 0.034) and shift pattern (B = -0.104, p = 0.010) were significant predictors, indicating that longer shifts and non-traditional schedules contribute to higher EE. Depersonalization (DP) was significantly predicted by department (B = 0.136, p = 0.021), suggesting that ICU assignments increase feelings of detachment. In contrast, personal accomplishment (PA) was not significantly predicted by any workplace factor, reflecting that a sense of professional achievement remains stable regardless of department, shift length, or shift pattern. These findings emphasize that EE and DP are sensitive to work schedules and departmental assignments, whereas PA is resilient to workplace conditions.
| Measure | Model 1 (EE) | Model 2 (DP) | Model 3 (PA) | |||
|---|---|---|---|---|---|---|
| B | p value | B | p value | B | p value | |
| Department | 0.005 | 0.946 | 0.14 | 0.021 | 0.02 | 0.619 |
| Shift Length | 0.087 | 0.034 | 0 | 0.095 | 0.02 | 0.407 |
| Shift Pattern | -0.1 | 0.01 | 0.05 | 1.408 | 0.01 | 0.719 |
Table 6: Multiple Linear Regression Analysis of Workplace Factors Predicting Burnout Dimensions (n = 278) Table 6: Multiple Linea
Table 6: Multiple Linear Regression Analysis of Workplace Factors Predicting Burnout Dimensions (n = 278) Table 6: Multiple Linear Regression Analysis of Workplace Factors Predicting Burnout Dimensions (n = 278) Abbreviations: EE: Emotional Exhaustion, DP: Depersonalization, PA: Personal Accomplishment The study demonstrates high levels of burnout in ED and ICU healthcare technologists, with the majority expressed as emotional exhaustion (EE). According to recent studies, burnout estimates vary widely according to setting, profession, instrument, and threshold definition. ICUs have consistently reported higher rates due to their naturally stressful work environment [12, 13]. The high rate of burnout observed in this study emphasizes the critical need for targeted interventions in these high- acuity healthcare settings. The exceptional 69.4% burnout prevalence among participants in this study far surpasses international averages cited in current literature. Recent studies from comparable environments cite burnout prevalence between 32-40% among ICU healthcare workers, with the emotional exhaustion dimension being the most commonly impacted [14, 15]. The higher rates found in this study can be attributed to the cumulative effect of long-term exposure to high-stress work conditions, enhanced patient acuity, and the challenging nature of emergency and critical care environments. Studies highlighted that job stressors are more likely to cause burnout compared to demographics, and found their results to be consistent with the rates of emotional exhaustion outcomes [16, 17].
Shift length and shift pattern were both significantly associated with emotional exhaustion. This finding is especially troubling because shift work throws off the body’s rhythm and shortens recovery time for the next shift. Non-
day shift schedules were associated with greater emotional exhaustion (p = 0.003), which is consistent with the current literature that suggests working night shifts has additional physiological and psychological stressors [18]. This is supported by recent research, which found that nurses working 12-hour shifts experienced noticeably higher levels of burnout than those working 8-hour shifts. The regression test also confirmed that increased shift length (p = 0.034) and pattern of shifts (p = 0.010) predicted emotional exhaustion and emphasized the core practice of scheduling in burnout development [19].
Some literature suggests that early-career healthcare workers have fewer coping skills and lower professional resilience [20, 21]. The prospective association of experience may simply index the accumulation of effective coping strategies and mounting familiarity with the stresses of critical care areas over time. The findings of this study are compatible with research literature, which shows variations in burnout among healthcare professionals. Healthcare professionals are prone to having dual burdens of professional obligations and personal family tasks, and thus enhance stress and susceptibility toward burnout. The cultural and social demands to fulfill multiple roles can intensify the effects of work-related stressors and hence produce more severe symptoms of burnout [22]. No statistically significant association was observed for marital status in the present analyses. This was consistent with the buffering effect for stress management of social support networks found in a study [23].
While no significant differences emerged between ED and ICU technologists for emotional exhaustion and personal accomplishment, ICU staff members had significantly higher depersonalization (p = 0.015). This is a reflection of the unique psychosocial demands of ICU environments, in that prolonged accompaniment by severely ill patients, end-of- life experiences, and high mortality levels render emotional detachment a survival technique [14, 24]. ICU technologists’ higher depersonalization scores should be read as a potentially maladaptive coping response to sustained emotional demands for managing emotional labor in critical care.
Implications for Healthcare Organizations
These findings also have significant policy and practice implications for healthcare. The observed high level of burnout requires immediate organizational intervention in shift selection, workload management, and support systems at the psychosocial level. Evidence-based scheduling protocols, like limits for consecutive shifts and mandated rest breaks, should be instituted to neutralize the detrimental effects of long working hours [25, 26]. Hospitals also need to identify the unique vulnerability through special support initiatives and mentoring programs. Implementation of evidence-based mental health intervention programs, such as stress management courses, building resilience programs, and peer support groups, is a priority on the organizational agenda [10, 27].
Limitations of the Study
While the study does provide insights into the situation, some limitations should be acknowledged. First, a cross- sectional design will not allow for inferring causality between shift patterns and burnout. In addition, since data is based on self-reports, underreporting or overreporting might occur about levels of burnout. Second, the study was conducted in selected tertiary hospitals in Islamabad, which may limit generalizability to other regions and healthcare settings.
Conclusions
This study indicates high burnout among ER and ICU health technologists, and emotional exhaustion and depersonalization as the areas most affected. Non-day shift schedules and longer duty hours were associated with higher emotional exhaustion, and sociodemographic variables showed less consistent associations. ICU workers exhibited slightly higher depersonalization than ED workers. The results require focused intervention through policy amendments to optimize shift scheduling and organizational interventions for psychosocial support. Burnout prevention is a professional need and an ethical responsibility for healthy personnel and enhanced patient safety.
References
-
Demerouti E, Mostert K, Bakker AB (2010) Burnout and work engagement: a thorough investigation of the independency of both constructs. Journal of occupational health psychology 15(3): 209-222.
-
Aiken LH, Clarke SP, Sloane DM, Sochalski J, Silber JH (2002) Hospital Nurse Staffing and Patient Mortality, Nurse Burnout, and Job Dissatisfaction. JAMA 288(16):1987-1993.
-
Maslach C, Jackson S (1981) The Measurement of Experienced Burnout. Journal of Organizational Behavior 2(2): 99-113.
-
Van Bogaert P, Timmermans O, Weeks SM, Heusden DV, Wouters K, et al. (2014) Nursing unit teams matter: Impact of unit-level nurse practice environment, nurse work characteristics, and burnout on nurse reported job outcomes, and quality of care, and patient adverse events—A cross-sectional survey. International Journal of Nursing Studies. 51(8): 1123-1134.
-
Folkard S, Tucker P (2003) Shift work, safety and productivity. Occupational Medicine 53(2): 95-101.
-
Lockley SW, Barger LK, Ayas NT, Rothschild JM, Czeisler CA, et al. (2007) Effects of Health Care Provider Work Hours and Sleep Deprivation on Safety and Performance. The Joint Commission Journal on Quality and Patient Safety 33(11): 7-18.
-
Barger SD, Donoho CJ, Wayment HA (2009) The relative contributions of race/ethnicity, socioeconomic status, health, and social relationships to life satisfaction in the United States. Qual Life Res 18(2): 179-189.
-
Fletcher D, Sarkar M (2012) A grounded theory of psychological resilience in Olympic champions. Psychology of Sport and Exercise 13(5): 669-678.
-
Stimpfel AW, Sloane DM, Aiken LH (2012) The Longer the Shifts for Hospital Nurses, the Higher the Levels of Burnout and Patient Dissatisfaction. Health Aff (Millwood) 31(11):2501-2509.
-
West CP, Dyrbye LN, Shanafelt TD (2018) Physician burnout: contributors, consequences and solutions. J Intern Med 283(6): 516-529.
-
Shanafelt TD, Boone S, Tan L, Dyrbye LN, Sotile W, et al. (2012) Burnout and Satisfaction with Work-Life Balance Among US Physicians Relative to the General US Population. Archives of Internal Medicine 172(18): 1377-1385.
-
Gualano MR, Sinigaglia T, Lo Moro G, Rousset S, Cremona A, et al. (2021) The Burden of Burnout among Healthcare Professionals of Intensive Care Units and Emergency Departments during the COVID-19 Pandemic: A Systematic Review. IJERPH 18(15): 8172.
-
Rani Garg P, Uppal L, Mehra S (2004) Family Planning and Young and Low Parity Couples: Learnings from Rural India. In: Tsikouras P, (Eds), Conception and Family Planning - New Aspects. Obstetrics and Gynecology. IntechOpen.
-
Van Mol MMC, Kompanje EJO, Benoit DD, Bakker J, Nijkamp MD (2015) The Prevalence of Compassion Fatigue and Burnout among Healthcare Professionals in Intensive Care Units: A Systematic Review. PLoS ONE 10(8): e0136955.
-
Chalil AR (2022) Physician burnout in critical care and emergency unit setting. International journal of health science 6(s6): 3158-3167.
-
Schaufeli WB, Desart S, De Witte H (2020) Burnout Assessment Tool (BAT)-Development, Validity, and Reliability. Int J Environ Res Public Health 17(24): 9495.
-
Maslach C, Leiter MP (2016) Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry 15(2): 103-111.
-
Shbeer A, Ageel M (2022) Assessment of Occupational Burnout among Intensive Care Unit Staff in Jazan, Saudi Arabia, Using the Maslach Burnout Inventory. Critical Care Research and Practice 16 :1-7.
-
Dall’Ora C, Ejebu OZ, Ball J, Griffiths P (2023) Shift work characteristics and burnout among nurses: cross- sectional survey. Occup Med (Lond) 73(4): 199-204.
-
Damico V, Margosio V, Teli M, Murano L, Ripamonti C (2021) Burnout-related symptoms among Italian ICU’s staff during the COVID-19 emergency. A multicentric survey study. Professioni infermieristiche 3: 166-172.
-
Migelheva A (2020) Prevalence and factors associated with Burnout Syndrome among employees of Emergency Treatment units at selected Teaching Hospitals in Sri Lanka. Longdom Publishing 9(3): 14-14.
-
Heidari H, Arabi M, Warziniack T, Kao SC (2021) Shifts in hydroclimatology of US megaregions in response to climate change. Environ Res Commun 3(6): 065002.
-
Gómez-Urquiza JL, De La Fuente-Solana EI, Albendín- García L, Vargas-Pecino C, Ortega-Campos EM, et al. (2017) Prevalence of Burnout Syndrome in Emergency Nurses: A Meta-Analysis. Crit Care Nurse 37(5): e1-e9.
-
Góis J, Santos C, Aragão N, Barbosa G, Rodrigues É, et al. (2024) Burnout Syndrome in Intensive Care Unit Workers in a City in Northeastern Brazil 12(8): 1-8.
-
Caruso R, Annaloro C, Arrigoni C, Ghizzardi G, Dellafiore F, et al. (2021) Burnout and post-traumatic stress disorder in frontline nurses during the COVID-19 pandemic: a systematic literature review and meta-analysis of studies published in 2020. Acta Biomed 92(S2): e2021428.
-
Stocchetti N, Segre G, Zanier ER, Zanetti M, Campi R, et al. (2021) Burnout in Intensive Care Unit Workers during the Second Wave of the COVID-19 Pandemic: A Single Center Cross-Sectional Italian Study. IJERPH 18(11): 6102.
-
Haruna J, Unoki T, Ishikawa K, Okamura H, Kamada Y, et al. (2022) Influence of Mutual Support on Burnout among Intensive Care Unit Healthcare Professionals. SAGE Open Nursing 8: 23779608221084977.
- Measuring What Matters: Data Gaps, Certificate of Need Reform, and Pediatric Psychiatric Inpatient Capacity in North Carolina
- Intersecting Epidemics and Climate Vulnerabilities in Conflict- Driven Displacement: Epidemiology, Systemic Challenges, and One Health Gaps in South Sudan
- Advancing Domestic Health Financing for Community Health System Sustainability in South Sudan: The Boma Health Initiative Model (2025–2035)
- Prevalence and Correlates of Post-Exposure Prophylaxis Uptake among Men Who Have Sex with Men in Kisumu County, Kenya
- Medical, Ethical, and Legal Conflicts Surrounding Euthanasia in Argentina. Its Global Implications
- Knowledge and Attitude on Menstrual Hygiene among Adolescent Girls Studying in Secondary Level in Public Schools of Chitwan District, Nepal