Psychiatric Morbidity among Victims of Violent Ethno-Religious Conflicts in Barkin Ladi, North Central Nigeria, Five Years After: Prevalence and Sociodemographic Correlates
Background: Mental health disorders are common presentations among persons who have faced crisis and other life threatening conditions. Several researchers in the past have tried to study the relationships between violent conflicts and mental health outcome. In this study, we assessed the prevalence and sociodemographic correlates of psychiatric disorders among victims of violent conflicts five years after ethno-religious conflicts in Barkin Ladi, Plateau State, North-Central Nigeria. Methodology: The study was a cross-sectional descriptive survey of victims of ethno-religious crisis in some communities of Barkin Ladi Local Government Area (LGA) of Plateau State, North-Central Nigeria. A total of 144 respondents were interviewed. Results: Majority of our study population were females (68.1%), while the mean age of all respondents was 41.2±2.9 years, with 43.8% within the 40-59 years age group. Eighty nine (61.7%) were married, 70.7% had no formal education and 83. 3% involved in low paying jobs. Among the victims, 56.3% had depression, 11.1% dysthymia, 52. 1% Post-traumatic stress disorder (PTSD), while 48.6%, had generalized anxiety disorders (GAD). Those with alcohol abuse and alcohol dependence were 19.4% and 8.3% respectively. With regards to the association between conflict, psychiatric morbidities and sociodemographic variables, age was associate with alcohol abuse (
Introduction
Violent conflicts have become universal challenge in all regions of the world [1]. The emotional aspects of trauma have been recognized since the inception of war. Violent conflict produces tremendous psychological as well as physical injuries and increases the burden of disease associated with negative mental health outcomes [2]. According to the Global Burden of Disease study, the burden of mental health and behavioral disorders is estimated to increase from 12 percent in 1990 to 15 percent in 2020 even as violent conflicts shift from the 16th to the 8th leading cause of disease [3]. The WHO estimated that, “10% of the people who experience traumatic events will have serious mental health problems and another 10% will develop behavior that will hinder their ability to function effectively. The most common conditions are depression, anxiety and psychosomatic problems such as insomnia, or back and stomach aches” [4]. Rubonis, et al. [5], conducted a meta- analysis of 52 studies, the report showed that psychiatric morbidity was 17% higher in groups that experienced a psychological trauma than in same groups before the disaster and in control groups. Nigeria has faced several ethno-religious conflicts since the wake of independence in 1960 [6] with several of these conflicts being witnessed in Jos, Plateau State [7]. Irrespective of the cause, conflicts, wars and terrorism produces psychopathological disorders on its victims. A cross-sectional cluster study of conflict in the Balkans has revealed that Kosovar Albanians aged 15 years or older reported a 17.1% prevalence rate for Post-Traumatic Stress Disorder (PTSD) [8]. Robert, et al. [9] while studying the mental health needs of victims of armed conflicts in Southern Sudan reported a prevalence of 36.2% for PTSD and 49.9% for depression. In a national multistage, cluster, population based survey in Afghanistan, symptoms of depression were found in 67.7% of respondents, symptoms of anxiety in 72.2%, and post-traumatic stress disorder (PTSD) in 42% [10]. The conflict between the majority Sinhala and minority Tamil population in Sri Lanka left 64.0% of its victims with one psychological problem or the other. Out of this percentage, the prevalence of Somatization was 41.0%, PTSD (27.0%), major depression (25.0%), anxiety disorders (26.0%) and functional disability (18.0%) [11]. In a recent study of internally displaced persons in one community in Plateau State, Agbir et al [12] found a 62.3% prevalence for depression. Other mental health problems associated with the victims include dysthymia (23.4%), alcohol abuse (30.5%), and alcohol dependence (21.0%). Generalized anxiety disorder (GAD) was 55.7% while posttraumatic stress disorder made up 58.7%. In a similar study, Maigari and Colleagues [13] studied the sociodemographic predictors of depression among survivors of armed conflict in Dogon na Hawa, Jos, Nigeria. They reported that 55.5% of the respondents had PTSD while the prevalence of depression was 44.7%. The study also observed that age, female gender, and being a household head were associated with depression. Pervasive violence and insecurity deteriorate social and economic conditions and impede access to basic needs including food, shelter, healthcare, education, and physical safety, which become a pivot for poor mental health. The psychopathological consequences of violent conflict cannot be overemphasized. The response to the psychological trauma by concerned authorities has not been encouraging. This could be due to dearth of information on the mental health consequences of violent conflicts in this part of the world. This study will therefore be an invaluable source of information for policy makers and disaster response agencies. The study assessed the prevalence and sociodemographic correlates of psychiatric disorders among victims of violent conflicts five years after ethno- religious conflicts.
Methodology
Ethical clearance was obtained from the Joint Ethics Committee of the Jos University Teaching Hospital. Permission was also sought from the Ward Head of the communities. The study is a multi-staged cross-sectional study of trauma victims 18years and above in Barkin Ladi Local Government Area of Plateau state. A total of 144 traumatized victims were interviewed. The sample size was calculated from the formula: N = Z2 x P(1-P)/d2 Where N = Sample size; Z = Confidence level = 1.96; P = Expected prevalence = 10% [4]; and d = Allowable error = 0.05 Putting the above into the formula; N = 1.962 x 0.1(1- 0.1)/0.052 = 138. This was scaled up to 144 to increase the statistical power of the result. In the first stage, Goldberg’s General Health Questionnaire (GHQ)-12 [14] was used to screen respondents, those who scored 4 and above were then administered the Mini International Neuropsychiatric Interview questionnaire (MINI) [15] in the second stage. The GHQ [14] is a self-reported screening instrument developed to detect diagnosable psychiatric disorders in primary care and community settings. The 12 item version is easier to administer and has been validated in different languages and cultures. It measures areas such as poor sleep, poor concentration, capability of making decisions, overcoming difficulties, enjoyment of normal activities etc. The MINI is a brief structured interview designed for major axis I psychiatric disorders in DSM-IV and ICD-10. It has both life time and current diagnosis versions. The life time diagnosis version was used for this study in order to provide a premise for comparing homogenous group. The Depression, Anxiety, PTSD, Alcohol Abuse, Alcohol Dependence and Dysthymia modules were used for this study. Sociodemographic variables were assessed with a semi-structured questionnaire designed by the authors. This was used to enquire about the age, gender, marital status, educational status and occupation. Data was analyzed using the Statistical Package for Social Sciences (SPSS) version 21. Descriptive statistics were used to summarize sociodemographic variables using frequency counts and percentages. The chi-square test was used to determine the association between categorical variables.
Results
| Frequency | Percentage (%) | |
|---|---|---|
| Gender: | ||
| Male | 46 | 31.9 |
| Female | 98 | 68.1 |
| Total | 144 | 100.0 |
| Age: | ||
| <20 years | 2 | 1.4 |
| 20-29 years | 23 | 15.9 |
| 30-39 years | 31 | 21.5 |
| 40-49 years | 37 | 25.7 |
| 50-59 years | 26 | 18.1 |
| ≥60 years | 25 | 17.4 |
| Mean±SD | 41.2±2.9years | Age range =40years |
| Total | 144 | 100.0 |
| Marital status: | ||
| Married | 89 | 61.7 |
| Never married | 22 | 15.3 |
| Divorced | 4 | 2.8 |
| Widowed | 27 | 18.8 |
| Separated | 2 | 1.4 |
| Total | 144 | 100.0 |
| Education: | ||
| 102 | 70.7 | |
| Primary | 26 | 18.1 |
| Secondary | 9 | 6.3 |
| Tertiary | 7 | 4.9 |
| Total | 144 | 100.0 |
| Occupation: (which classification please) | ||
| Group II | 3 | 2.1 |
| Group III | 4 | 2.8 |
| Group IV | 120 | 83.3 |
| Group V | 11 | 7.6 |
| Group VI | 6 | 4.2 |
| Total | 144 | 100.0 |
| Ethnicity | ||
| Berom: | 144 | 100.0 |
| Others | 0 | 0 |
| Total | 144 | 100.0 |
| Religion: Christianity | 144 | 100.0 |
| Islam | 0 | 0 |
| Others | 0 | 0 |
| Total | 144 | 100.0 |
Table 1: Sociodemographic variables of respondents.
| Psychiatric disorder→ | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Depression | Dysthymia | PTSD | Alcohol abuse | Alcohol dependence | GAD | |||||||||||||||
| Response↓ | ||||||||||||||||||||
| Yes No Total (144) | 81(56.3%) 63(43.7%) 100.0% | 16(11.1%) 128(88.9%) 100.0% | 75(52.1%) 69(47.9%) 100.0% | 28(19.4%) 116(80.6%) 100.0% | 12(8.3%) 132(91.7%) 100.0% | 70(48.6%) 74(51.4%) 100.0% |
Table 2: Prevalence of psychiatric disorders among respondents.
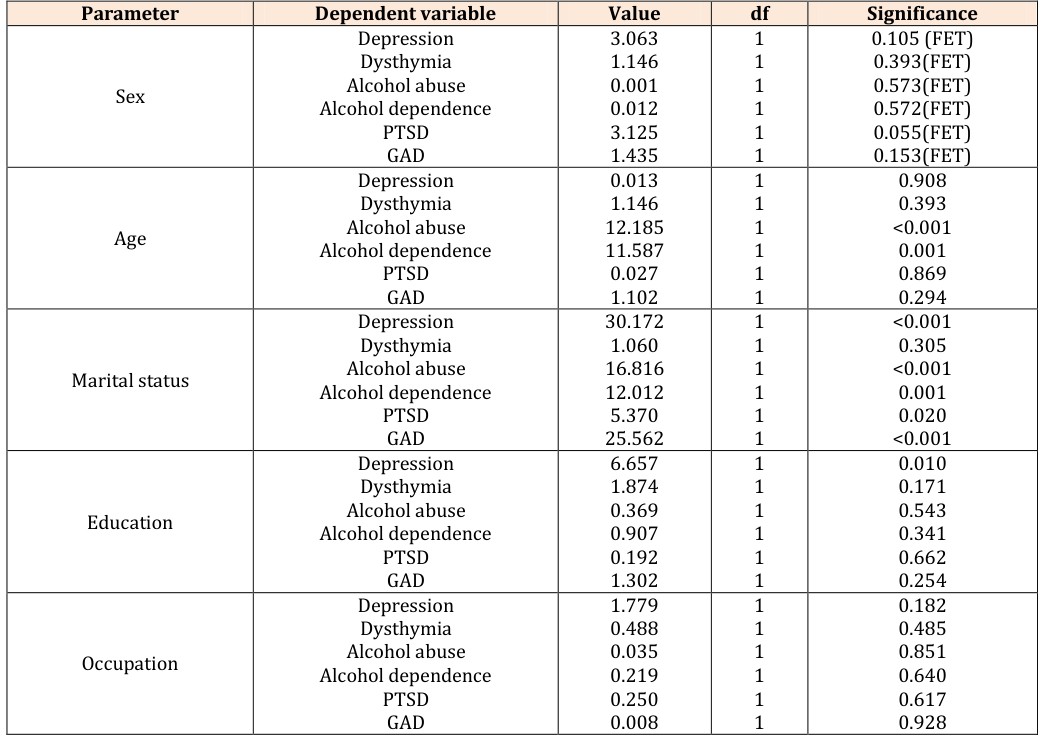
- FET = Fisher’s Exact Test
Table 3: linear (Association) Relationship between psychiatric disorders and sociodemographic variables.
A total of 144 respondents were interviewed, comprising of 46(31.9%) males and 98(68.1%) females with mean age of 41.2±2.9years. The age range for the studied population was 40 years. 38.8% of the subjects were less than 40 years as at the time of this study, while 43.8% were within the 40-59 years group. Those who are 60 years and above completed the picture with 17.4%. As many as 61.7% were married, 15.3% single, 2.8% divorced, 18.8% widowed and 1.4% were separated. Overall, those who did not acquire any form of formal education were 70.7%, primary education which had 18.1% was the most acquired level of formal education with secondary and tertiary education constituting 6.3% and 4.9% respectively. None of our subjects was in the professional class (group I) in terms of occupation. The distribution of the subjects based on occupational groups yielded 2.1% for those in occupational group II, 2.8% in group III and an unprecedented 83.3% for those in group IV (masons, drivers, small scale farmers, gas station attendants, traders etc). Group V had 7.6% representation and group VI, 4.2%. All the subjects were of the Berom ethnic group and Christians. (The write up is too much, let’s make it brief as it will be seen on the table. This is like repeating the table in writing). Majority of the respondents were females (68.1%), married (61.7%), with no formal education (70.7%), in occupational group IV (83.3%) and with a mean age of 41.2±2.9 years (Table 1).
Table 2
Our study also sought to assess the prevalence of some psychiatric disorders among victims of violent crises. The result obtained showed a prevalence of 56.3% for depression, 11.1% for dysthymia, and 52.1% for PTSD. Other includes alcohol abuse 19.4%, alcohol dependence 8.3 % and GAD, 48.6%. (Same here). Depression was the commonest psychiatric disorder found in the study followed by PTSD and the least was alcohol dependence (Table 2).
Table 3
Regarding the influence of sociodemographic factors, gender was not found to have a significant main effect on psychiatric morbidities among the subjects. Age was significantly associated with alcohol abuse (<0.001) and alcohol dependence (0.001). No such association was found with depression (0.908), dysthymia (0.393), PTSD (0.869) and GAD (0.294). Marital status was statistically associated with depression (<0.001), and to alcohol abuse (<0.001), alcohol dependence (0.001), PTSD (0.020) and GAD (<0.001). Only depression related to education (0.010). Occupation was not significantly related to any of the psychiatric morbidities studied. (The same applies here please). Marital status was significantly associated with Depression, PTSD, alcohol abuse/alcohol dependence and GAD (Table 3).
Discussion
This study assessed the prevalence of psychiatric morbidities and the effect of sociodemographic factors among victims of Ethno-Religious conflicts in Barkin Ladi Local government Area of Plateau State, five years post- conflict. From the study, majority of the respondents were females. This is consistent with previous studies were females predominated war victims. Results by Agbir, et al. [12], Maigari, et al. [13], Roberts, et al. [16] all predicted similar outcomes.
There is a convincing evidence of a strong association between trauma experience and risk of psychiatric disorders. The prevalence of Psychiatric disorders was increased among the respondents. Depression was found in more than half of the respondents. This is a remarkable increase from the 15% prevalence of depression among the general population as reported by the World Health Organization (WHO) [17]. Similar studies in the past have also revealed an increase prevalence of depression among victims of violent conflicts [9, 10, 12, 13]. The factors that could be responsible here would include loss of loved ones, sources of livelihood and properties putting the victims in a state of helplessness and hopelessness [18]. About one tenth of our subjects had dysthymia. This figure is about 3 times the 3.7% prevalence of dysthymia in the general population [19]. Persisting low level of depressive symptoms could be adduced to a state of pervasive socio-economic decline, increased household strain faced by victims, loss of a family member or property that usually accompanies violent conflicts [18]. The report of the study conducted by Agbir and colleagues [12] also yielded a similar result. From our study, more than half of the respondents met the criteria for PTSD. Studies in the general population from randomly selected samples reported a prevalence rate of 7.8% with the disorder occurring in 10.4% of women and 5.0% of men [20]. In a similar study by Breslau and Colleagues, the prevalence of PTSD was 8.3% [21]. Our finding concurred with several other studies in the past. Agbir and colleagues [12] reported a prevalence of 58.7%, Maigari, et al. [13] revealed a 55.5% prevalence of PTSD among victims of armed conflicts. In a community based study in Rwanda, 24.8% met symptom criteria for PTSD [22] while a similar result among Afghan war victims was 42.0% [10]. This wide difference between our study population and the general population could be explained by multiplier effect of repeated violence faced by our respondents. Facing life threatening events has been linked to increased risk of PTSD by several studies in the past [8, 9, 10, 11, 12, 13]. The poor living condition of the victims, increasing level of poverty and lack of responsiveness of the government to the emotional needs of victims all contribute to perpetuate the symptoms of PTSD. Anxiety is a normal response to an unpleasant emotional stimuli or perceived threat. While up to about 30% of the population has experienced anxiety symptoms in their lifetime, generalized anxiety disorder affects about 12.5% of the general population [23, 24]. From our study close to about half of the respondents had symptoms of generalized anxiety disorders (GAD). Uncertainty about the future, repeated exposure to violence, worry about safety, rumination over impending poverty due to loss of properties could all contribute to persistence of symptoms. Increased use of alcohol and other psychoactive substances among war victims or veterans has been reported in many studies [25, 26, 27]. Alcohol abuse was found in about 2 out of 10 of our respondents while about 1 in 9 was dependent on alcohol. Published studies of military personnel deployed to Iraq and Afghanistan confirm the association between stress related to combat and adverse mental health outcomes. The study also reported significantly higher rates of alcohol misuse [28, 29, 30, 31, 32]. War creates acute and long-lasting health problems in men and women, however, many aspects of war affect the health of women disproportionately. Many women may in war situations be faced with the main responsibility of becoming household heads especially when the destiny of their husbands is unknown. The woman’s capacity to cope may become overloaded if the household is facing disaster [18]. An alternate explanation for this could be due to the tendency of women to express emotional symptoms compared to their male counterpart who conceal their symptoms to avoid being tagged a weakling and thus resort to the use of alcohol and other substances to mask their symptoms [33]. Despite several reported cases of women suffering from psychiatric disorders following violent conflicts, our study could not find an association between psychiatric morbidities and gender. This is in contrast to that reported by Maigari, et al. [13], Kessler, et al. [20], and Breslau, et al. [21] where gender was associated with depression and PTSD. The possible reason for the difference could be adduced to the fact that most of the victims in our study area were still married (61.7%) with only a few being widowed by the conflicts. Thus, most of the women were enjoying some form of social support from their spouses. Our study found a linear association between age with alcohol abuse and alcohol dependence. Studies conducted by several authors have revealed that adolescents exposed to high levels of violent conflicts are more likely to endorse maladaptive coping strategies such as saying “mean” things to other people, and using alcohol and drugs [34, 35]. Marital status correlated with depression, alcohol abuse, alcohol dependence, PTSD and GAD. The association could be due to additional familial demands that married individuals may face post-conflict. Loss of family resources and the difficulties involved in reorganizing the family life and values may contribute as well. In a study conducted among Canadian Military personnel returning from Afghanistan, an association was noted between marital status and deteriorating mental health (especially for PTSD and depression) by Watkins et al [36]. They observed that this association was stronger for married personnel than it was for singles. Our study failed to show an association between occupation and psychiatric morbidities among our respondents. This does not concur with reports by Kessler et al [20] and Breslau et al [21] who both revealed a correlation between occupation and depression and PTSD. The homogeneity of the occupations of our respondents could explain why we were unable to find such association. Among all the variables studied, only depression was significantly associated with educational status (0.010). Education provides opportunity for employment, income [37], problem solving ability, supports healthy lifestyle and promotes sound mental health [38, 39]. Since over two- thirds of our subjects had no formal education, and involved in menial jobs, they are more likely to face hardships due to poor finances, poor coping strategies, and difficulties in rebuilding back their lives. These increases their stress and feeling of hopelessness, thus, their proneness to depression. This position was also the outcome of a study by Bjelland et al [40].
Conclusion
In conclusion, we studied the prevalence and sociodemographic correlates of psychiatric morbidities in victims of Ethno-Religious conflicts in Barkin Ladi LGA in North-Central Nigeria. Our study found that ethno- religious conflicts was significantly associated with poor mental health outcomes. The prevalence of Depression, Dysthymia, PTSD, Anxiety, Alcohol abuse and dependence were all high. Sociodemographic variables such as age, gender, marital status, education and occupation which the study show to affect mental health outcome either positively or otherwise should form a focus for effective intervention. If some conditions remain unaddressed, it will be hard to effectively reduce the prevalence of psychiatric disorders among victims.
Recommendation
Ethno-religious crisis is a known predisposing factor for poor mental health. Government at all levels most be more proactive in preventing these crises and providing psychological care to victims. Interventions should focus on strategies that will improve the mental health of post- conflict victims. A deliberate effort and or policy should be drawn to highlight the various levels of intervention (psychological, social, religious and physical) that will reduce stress and suffering of victims.
Limitation of the study
The study was carried out in a community with ethnic and religious homogeneity and therefore may not permit generalization of the outcome. Furthermore, the study only considered adults population excluding children. No consideration was given to persons with previous histories of mental illness. Considering the low education level of our respondents, it was difficult for some respondents to remember the events five years after the conflict. Future studies on similar areas may consider additive effect of ethno-religious conflicts on existing mental illness among victims. Other researchers may also want to evaluate the differences in response to violent conflicts between younger population and the elderly. Conflict of interest: None to declare
References
-
Gleditsch NP, Wallensteen P, Eriksson M, Sollenberg Strand H (2002) Armed Conflict 1946–2001: A New Dataset, Journal of Peace Research 39(5): 615-637.
-
Baingana F, Bannon I, Thomas R (2005) Mental Health and Conflicts: Conceptual Framework and Approaches. The World Bank.
-
De Jong Joop (ed) (2002) Trauma, war and violence: public mental health in socio-cultural context. Psychology.
-
World Health Organization (1991) World health report - Mental health: new understanding, new hope. Geneva: Switzerland, impairment in wake of disaster; the disaster psychopathology relationship Psychological Bulletin 104: 384-399.
-
Rubonls AV, Bichman R (1991) Psychological impairment in wake of disaster; the disaster psychopathology relationship. Psychological Bulletin 109(3): 384-399.
-
Salawu B (2010) Ethno-religious conflicts in Nigeria: Causal analysis and proposal for new management strategies. Eur J Soc Sci 13: 345-353.
-
Onuaha FC, Gaiya B, Namji R (2010) Jos crisis and National Security: A Reflection. Nigeria Forum 3: 81- 103.
-
Lopes Cardozo B, Vergara A, Agani F, Gotway CA (2000) Mental health, social functioning, and attitudes of Kosovar Albanians following the war in Kosovo. JAMA 284(5): 569-577.
-
Agbir TM, Audu MD, Obindo JT, Davou FJ, Gyang BA, et al. (2016) Depression among Internally Displaced Pesons in Riyom, Plateau State, North-Central Nigeria. J Medical Res and Pract 4(1): 13-17.
-
Cardozo BL, Bilukha OO, Crawford CA, Shaikh I, Wolfe MI, et al. (2004) Mental health, social functioning, and disability in postwar Afghanistan. JAMA 292(5): 575- 584.
-
Somasundaram D, Jamunanatha CS (2002) Psychosocial consequences of war: northern Sri Lankan experience. In: de Jong JTVM (ed). Trauma, war and violence: public mental health in socio- cultural context. New York: Plenum 205-258.
-
Robert B, Damundu EY, Lomoro O, Sondorp E (2009) Post-conflict mental health needs: a cross-sectional survey of trauma, depression, and associated factors in Juba, Southern Sudan. BMC Psychiatry 9: 7.
-
Maigari YT, Moses DA, Tungchama FP, Davou FJ, Go’ar GS, et al. (2017) Sociodemographic predictors of depression among survivors of armed conflict with posttraumatic stress disorder in Dogon na Hawa, North-Central Nigeria. Jos J Med 11(1): 8-16.
-
Goldberg D (1978) Manual of General Health Questionnaire. Windsor: National Foundation for Educational Research.
-
Sheehan DV, Lecrubier Y, Harnett SK, Amorin P, Janavs J, et al. (1998) Mini International Neuropsychiatric Interview: The Development nad Validation of a Structured Diagnostic Psychiatric Interview for DSM-IV and ICD-10. J Clin Psychiatry 59: 22-23.
-
Roberts B, Ochaka KF, Browne J, Oyok T, Sondorp E (2008) Factors associated posst-traumatic stress disorder and depression among internally displaced persons in Northern Uganda. BMC Psychiatry 8(38): 1-9.
-
Ormel J, Tiemens B (1997) Depression in primary care. In: Honig A, van Praag HM, eds. Depression: Neurobiological, Psychopathological and Therapeutic Advances. Chichester, UK: John Wiley 151(7): 979- 986.
-
Arcel LT, Kastrup M (2004) War, women and health. Nordic Journal of Women’s Studies 12(1): 40-47.
-
Balwin DS (2000) Dysthymia: options in pharmacotherapy. In: Palmer KJ. Managing depressive disorders. Philadelphia: Lippincott, Williams and Wilkins 17-28.
-
Kessler RC, Sonnege A, Bromet E, Hughes M, Nelson CB (1995) Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry 52(12): 1048-1060.
-
Breslau N, Kessler RC, Chilcoat HD, Schultz LR, Davis GC, (1998) trauma and post-traumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Archives of General Psychiatry 55(7): 626- 632.
-
Pham PN, Weinstein HM, Longman T (2004) Trauma and PTSD symptoms in Rwanda: implications for attitudes toward justice and reconciliation. JAMA 292(5): 602-612.
-
Dopheide J, BCPP, Park S (2002) The Psychopharmacology of Anxiety. Psychiatric Times 19(3).
-
World Health Organization. The World Health Report 2004. Changing History. Annex Table3: Burden of disease in DALYs by cause, sex and stratum in WHO regions, estimates for 2002.
-
Demmel R, Hagen J (2004) the structure of positive alcohol expectancies in alcohol dependent inpatients. Add Res The 12(2): 125-140.
-
Kozaric-KD, Ljubin T, Grappe M (2000) Comorbidity of posttraumatic stress disorder and alcohol dependence in displaced persons. Croat Med J 41(2): 173-178.
-
Schuckit MA, Smith TL, Chacko Y (2006) Evaluation of a depression-related model of alcohol problems in 430 probands from the San Diego prospective study. Drug Alcohol Depend 82(3): 194-203.
-
Hoge CW, Auchterlonie JL, Milliken CS (2006) Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. JAMA 295(9): 1023-1032.
-
Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI, et al. (2004) Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N Engl J Med 351(1): 13-22.
-
Milliken CS, Auchterlonie JL, Hoge CW (2007) Longitudinal assessment of mental health problems among active and reserve component soldiers returning from the Iraq war. JAMA 298(18): 2141- 2148.
-
Smith TC, Ryan MA, Wingard DL, Donald JS, James FS, et al. (2008) New onset and persistent symptoms of post-traumatic stress disorder self reported after deployment and combat exposures: prospective population based US military cohort study. BMJ 336(7640): 366-371.
-
Smith TC, Wingard DL, Ryan MA, Kritz-Silverstein D, Slymen DJ, et al. (2008) Prior assault and posttraumatic stress disorder after combat deployment. Epidemiology 19(3): 505-512.
-
Shipherd JC, Stafford J, Tanner LR (2005) Predicting alcohol and drug abuse in Persian Gulf War veterans: what role do PTSD symptoms play? Addict Behav 30(3): 595-599.
-
Plancherel B, Bolognini M (1995) Coping and mental health in early adolescence. Journal of Adolescence 18(4): 459-474.
-
Flannery DJ, Singer M, Williams L, Castro P (1998) Adolescent violence exposure and victimization at home: Coping and psychological trauma symptoms. Int Rev Victimol 98: 29-48.
-
Watkins K, Lee JEC, Zamorski MA (2017) Moderating effect of marital status on the association between combat exposure and post-deployment mental health in Canadian military personnel. Military Psychology 29(3): 177-188.
-
Cockerham WC (2005) Healthy Lifestyle Theory and the Convergence of Agency and Structure. J Health Soc Behav 46(1): 51-67.
-
Link BG, Mary CL, Bruce PD (1993) Socioeconomic Status and Depression: The Role of Occupations Involving Direction, Control and Planning. Am J Soc 98(6): 1351-1387.
-
Zimmerman FJ, Christakis DA, Stoep AN (2004) Tinker, Tailor, Soldier, Patient: Work Attitudes and Depression Disparities among Young Adults, Soc Sci Med 58(10): 1889-1901.
-
Bjelland I, Krokstad S, Mykletun A , Alv AD, Tell GS, et al. (2008) Does Higher Educational Level Protect Against Anxiety and Depression? The HUNT Study. Soc Sci Med 66(6): 1334-1345.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis