"Mad Lives too Matter": Assessing the Factors that Account for Poor Mental Health Intervention Programmes in the Western Region of Ghana
The study was conducted to assess the factors that account for poor mental health intervention programs in the Western Region of Ghana. A survey design was adopted for the study, using purposive and simple random techniques with a sample size of 200 respondents. The data were gathered using structured questionnaire and interview guide. Quantitative data analysis methods were used with the aid of SPSS version 23.0. The study found out the economic, sociocultural and institutional challenges that impact negatively on mental health intervention programmes in Ghana. It was recommended that Ghana Health Service and other health delivery agencies such as the Christian Health Association of Ghana should collaborate with the Ministry of Health to promote timely access to effective treatment of mental health conditions, including mild-to-moderate mental illnesses, in both community mental health and primary care settings and through co-location of health professionals to facilitate the referral to specialist mental health care, while ensuring the involvement of people living with mental health conditions in decisions about the appropriate care and treatment plan.
Introduction
Study Background
Back to the theoretical background of mental health, the definition of the WHO [1] includes three categories: well-being, effective functioning of an individual, and effective functioning for a community. In accordance with these categories, Keyes [2] says that mental health is a combination of emotional, social and psychological wellbeing, where emotional wellbeing is the realization of well-being, social well-being the realization of effective functioning within a community and psychological well-being the effective individual functioning. Approximately one of every four people suffers from poor mental health, making it a leading cause of disability around the globe [3]. Poor mental health increases susceptibility to both infectious and chronic diseases and accounts for more than 30% of years of life lost worldwide [4].
Problem Statement
Psychiatry in Ghana is neglected in health care and research. The enormity of the problem made Adomakoh exclaimed, ‘There is a dearth of detailed knowledge of psychiatric illness in this country’ [5]. Mental health constitutes the most neglected sector in Ghana. In fact, in no time has there ever been an intentional neglect of a field as relevant as mental health. Perhaps many policy makers and implementers feel that ‘mad lives don’t matter’. But it will be very unfortunate if this is the feeling because there can be no health without mental health [6]. As a result, the problem of failed mental health interventions points in many directions – intentional neglect, unattractive nature of the mental health sector, lack of motivation, inadequate health workforce to implement mental health intervention programs, lack of government support, lack of credible data, among others. Although, the mental health bill has been passed, provisions made have not been implemented. The Board formed to address issues concerning mental illness has not been able to do what is expected of them apparently because the government has still not provided enough structures for them to function. It is against this backdrop that the study was conducted to assess the factors accounting for poor mental health programs in the Western Region of Ghana.
General Objective
The principal objective of this study is to assess the factors that account for poor mental health programs in the Western Region of Ghana.
Specific Objectives
The specific objectives constitute the following;
- To identify the socio-economic factors influencing mental health programs in the Western Region of Ghana.
- To identify the socio-cultural factors influencing mental health programs in the Western Region of Ghana.
- To find out available mental health intervention programs in the Western Region of Ghana.
- To identify the institutional challenges that impede successful implementation of mental health intervention programs in the Western Region of Ghana.
The Mental Health System in Ghana
In Ghana, there are three publicly acknowledged psychiatric hospitals, namely the Accra, Pantang and Ankaful Psychiatric hospitals, with a host of private centers helping to manage mental disorders. Regrettably, the country can boast of very few specialists and professional nurses to manage the heavy load of mental healthcare. The mental health service in Ghana is available at most levels of care. However, the majority of care is provided through specialized psychiatric hospitals, with relatively less government provision and funding for general hospital and primary healthcare-based services. The few community-based services being provided are private. In summary, most treatment and care is being provided by the specialized hospital, close to the capital, Accra, and servicing a small proportion of the population in need.
Socio-Economic Factors Influencing Mental Health Programs
Mental health influences physical health through its influence on health behaviour, which is socially patterned and deeply embedded in people’s social, cultural and material circumstances The relative contribution of individual characteristics (affect, cognitive and social skills), social context (peers, social networks, relationships) and material factors (income, access to healthy products) is difficult to untangle and interventions to improve health behaviour through improving mental health (in schools for example) often attempt to address all three areas [7].
It is already well established that mental illness, across the spectrum of disorders, is both a direct cause of mortality and morbidity and a significant risk factor for poorer economic, health and social outcomes, although these adverse outcomes vary by type of disorder and socioeconomic status [8]. However, it is now becoming clear that the presence or absence of positive mental health or ‘wellbeing’ also influences outcomes across a wide range of domains. These include healthier lifestyles, better physical health, improved recovery, fewer limitations in daily living, higher educational attainment, greater productivity, employment and earnings, better relationships, greater social cohesion and engagement and improved quality of life [7].
There are still attitudes within most societies that view symptoms of psychopathology as threatening and uncomfortable, and these attitudes frequently foster stigma and discrimination towards people with mental health problems. Such reactions are common when people are brave enough to admit they have a mental health problem, and they can often lead on to various forms of exclusion or discrimination either within social circles or within the workplace. Tackling this public health burden is a global challenge, for mental health systems in many countries remain seriously under- resourced and under-developed [9]. It has been calculated that almost 90% of global health expenditure occurs in high-income countries which have only 16% of the world population [10]. This disparity in expenditure is likely to be worse in the area of mental health because one-third of countries do not have a specific mental health budget, while 36% of those countries that do, allocate less than 1% of their public health budget to mental health [9]. There is a widespread view that mental health problems in low-income countries could and should be tackled at the primary care level [11], but on the basis of the current functioning of primary health care, there is only limited evidence to support such an approach, and there are almost no economic data.
Socio-Cultural Factors Influencing Mental Health Programs
According to Mark R, et al. (2013) [12] cultural factors exert an influence on many aspects of mental health care, from the initial seeking of professional help, through the procedures of diagnosis and treatment, to after care and social reintegration, including the organization of mental health services. What becomes clear is that culture and social contexts, while not the only determinants, shape the mental health of minorities and alter the types of mental health services they use. Cultural misunderstandings between patient and clinician, clinician bias, and the fragmentation of mental health services deter minorities from accessing and utilizing care and prevent them from receiving appropriate care [8].
The culture of the patient, also known as the consumer of mental health services, influences many aspects of mental health, mental illness, and patterns of health care utilization. One important cautionary note, however, is that general statements about cultural characteristics of a given group may invite stereotyping of individuals based on their appearance or affiliation. Because there is usually more diversity within a population than there is between populations (e.g., in terms of level of acculturation, age, income, health status, and social class), information in the following sections should not be treated as stereotypes to be broadly applied to any individual member of a racial, ethnic, or cultural group [8].
Availability of Mental Health Intervention Programs
There are programs that only target to reduce the incidence of mental programs among healthy people. Others also target full grown mental persons in their quest to take them off the street. The unfortunate event here is that little is achieved for all these targets. For instance, programs that target to take mental persons off the street readily. Mental health services in Ghana are available at most levels of care. However, the majority of care is provided through specialized psychiatric hospitals (close to the capital and servicing only small proportion of the population), with relatively less government provision and funding for general hospital and primary health care based services. The few community-based services being provided are private [9].
In 2011, there was a mental health policy in place dated 1996. Unfortunately, it did not cover the integration of mental health into primary care nor the protection of human rights of the users, but it did include the following components: organization of services, developing community_, mental health services, human resources, involvement of patients and families, advocacy and promotion, equity of access to mental health services across different groups, financing, quality improvement,_ and monitoring system [13]. Mental health programs are behind schedule in terms of comparing the rate of increase in mental health cases on street canyons and the impact of the programs thereof. The implementation of mental health programs in itself is a challenge and many mental health program implementers miss a crucial point in their quest to address the mental health challenge.
Institutional Challenges Facing Mental Health Intervention Programs
It is well known that low- and middle-income countries allocate lower proportions of their national resources to health care, but the global disparity is much more marked when we look at expenditure on mental health services and treatments. A recent estimate put the percentage of the total health budget spent on mental health as 1.5% in low-income countries, 2.8% in middle- income countries and 6.9% in high-income countries [14]. Figures such as these do not tell the whole picture, because some mental health treatment and support will be provided from generic health budgets such as those allocated to primary care. It is highly unlikely, however, that the mental health funding proportion from these generic sources will greatly alter the overall picture of a very low provision in low-income countries. In addition, there is very poor integration of mental health services into general health care in most countries of which Ghana is not an exception.
The National Health Insurance Scheme (NHIS) passed in parliament in 2003, ensured universal healthcare services for all residents in Ghana [15]. However, while it says mental illness is exempt from the Insurance Scheme, it implies that patients with mental illness do not qualify to register with the Insurance Scheme [16]. The World Health Organization (WHO) estimates that 1.18 million additional mental health workers are needed to close the mental health treatment gap in low- and middle-income countries [17]. The WHO’s Mental Health Gap Action Program (mhGAP) and a number of research priority- setting exercises, including the Lancet global mental health group and the Grand Challenges in Global Mental Health Initiative, have identified mental health workforce expansion as a key component for improving mental health worldwide [18].
According to Brink H (2006) [19] Mental health nurses at the Accra Psychiatric Hospital have embarked on what they call ‘Run from danger’ strike. The nurses claim the numerous challenges faced by the health facility, including lack of hospital supplies and consumables, have put their lives at risk because they could be harmed by the patients. A statement by the Psychiatric Nurses Group (PNG) to the hospital’s management on behalf of the nurses stated, “Staff at Accra Psychiatric Hospital (APH) face numerous challenges which bother on the shortage of medication, inadequate food for patients and lack of basic logistics to carry out our professional duties.
Again, the Regional coordinators of Mental Health Services in Ghana Dr Akwasi Osei have lamented the severe and persistent shortage of essential psychiatric medicines and supplies for mental health patients in the country in the whole of 2015. The shortage reported, had in many ways affected mental healthcare delivery of the already lackadaisically supported Mental Health Services of the Ghana Health Service (GHS). To this end, patients and facilities had no option than to resort to the open market where prices of such medications were very expensive. The situation also forced most patients and their caregivers to refuse review visits since they could not afford their medications and in some cases not get it at all. The discussions at the review meeting indicated that the shortage was mainly due to the lack of funds which was not forthcoming from the government and some bureaucratic procurement processes [19].
Methodology
Profile of Study Area
The Western Region of Ghana is situated in the south- western part of Ghana. It is bordered on the east by Central Region, to the west by the Ivory. The region occupies a total land area of 23,760 sq. km, which makes it the fourth largest among the regions in terms of land size. It has a population density of 99.3 people per sq. km. The region is 42.4% urban with an annual urban growth rate of 3.5%. The region experiences more inflows from people to other parts of the country than people moving into the region, this therefore gave the region a net migration value of 282,119 in 2010. With regards to the economy, the labour force participation rate for population aged 15 - 64 is almost 71.4%. he population of the region grew from 1,924,577 in 2000 to 2,376,021 in 2010.
Study Design and Type
A range of methods were used to arrive at the research findings. This study adopted a survey study design. A survey according to Tariq (2009) is a method of gathering information from a number of individuals, known as a sample, in order to learn something about the larger population from which the sample is drawn. This study uses the survey method because it involves a statistical study of a sample population by asking questions on the socio-economic factors that influence mental health programmes, socio-cultural practice that influence mental health, the available mental health intervention programmes, and the institutional challenges facing mental health. The study was based on questionnaire and interview guide. The study was descriptive because it describes the views of respondents on mental health. The study sought to describe events as they were at the time of interview and questionnaire administration.
Study Population
Patel V, et al. (2003) Defines study population as “an entire group or persons or objects that are of interest to the researcher”. Therefore, the population of the study will constitute mental health officers, medical directors, medical superintendents, family members of people with mental health conditions. It is believed that these categories of respondents were in the right position to respond to the research questions appropriate hence the main reason this population was chosen [20].
Sampling Techniques and Sample Size
The study employed two sampling techniques thus; the probability and the non-probability sampling techniques. Under the non-probability sampling technique, purposive sampling technique was used to select key informants. The purposive sampling technique was used because the researchers have a particular target in mind that could provide the needed information to satisfy the study objectives. Under the probability sampling technique simple random sampling was used. Moving to the selection of respondents for the study, the researcher used simple random sampling technique to select one region out of the ten (10) regions in the Ghana through balloting. All the names of the ten (10) regions districts were written on pieces of papers and shuffled. One paper was selected at random which happened to be Western region. The simple random sampling technique was used by the researcher for the study to ensure that all students have equal and independent opportunity to participate. A sample size of 200 respondents was used for the study including key informants and families of people with mental health conditions in the selected districts.
Data Collection Techniques
Both secondary and primary data collection methods are used during the research. Secondary data sources are used to access information from books, journals, magazines, reports and the Internet. Under the primary data collection method, both quantitative (survey structured questionnaire) and qualitative methods (in- depth interviews and participant observation) are used through well-structured questionnaire.
Data Processing and Analysis
The data collected was examined and analyzed objectively to capture and present an excellent insight into the research topic. Quantitative data analysis method was used with the aid of Statistical Package for Social Sciences (SPSS) version 23.0 in the analysis of the data. By the use of this software, appropriate tables, frequencies and charts were generated which aided in easy understanding of the research results.
Limitations of Study
The study was limited to selected districts in the western region but could not collect data from the entire population understudy due to lack of sufficient funds. The sampling procedure used for the respondents might have excluded some respondents for the study. Time did not also permit the researcher to include larger sample size to ensure more appropriate results since the larger the sample size the more accurate the outcome of the study. However, with the use of systematic sampling technique in selecting the respondents, the researcher believed that the error of sampling bias was minimized and inference could made to the general population.
Presentation and Interpretation of Data
Socio-Economic Factors Influencing Mental Health Programs
Response Frequency
Percentage
(N) (%) Stigma and Discrimination 90 50.0 Influence on health behavior 14 7.50 Poverty 34 18.8 Trust and social capital 5 2.5 Insecurity and hopelessness 18 10 Rapid social change and risks of violence 16 8.70 Peer influence 4 2.5 Total 180 100 Source: Field Survey, 2017 Table 1: Social Factors Influencing Mental Health Programs.
Table 1 above depicts some of the social factors that influence mental health programs. The results obtained revealed that half (50%) of the respondents state stigmatization and discrimination, poverty was 18.8% while between 2-10% of the respondents affirmed insecurity and hopelessness, rapid social change and risks of violence, influence on health behavior, trust and social capital, and peer influence.
| Statement | Response | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | T | otal | ||||||||||||||
| Poor mental health programs are a consequence of social, economic and environmental inequalities | 0.00 | 3.70 | 15.0 | 37.5 | 43.8 | 100.0 | ||||||||||||||
| Poor mental health programs are consistently associated with unemployment. | 2.50 | 3.70 | 41.3 | 35.0 | 17.5 | 100.0 | ||||||||||||||
| Poor mental health is associated, less education, low income or material standard of living. | 0.00 | 0.00 | 12.5 | 62.5 | 25.0 | 100.0 |
Table 1: Statements on Socio-Economic Issues Influencing Mental Health Programs.
| Higher national levels of income inequality are linked to a higher prevalence of mental illness and low intervention programs | 18.7 | 2.50 | 17.5 | 32.5 | 28.8 | 100.0 |
|---|---|---|---|---|---|---|
| Mental health problems have considerable negative consequences for quality of life in low- and middle-income countries | 6.30 | 8.70 | 26.3 | 25.0 | 33.7 | 100.0 |
| The country is under-resourced and under-developed to finance mental health intervention programs. | 10.0 | 13.8 | 23.7 | 27.5 | 25.0 | 100.0 |
Table 2: Statements on Socio-Economic Issues Influencing Mental Health Programs.
Source: Field Data, 2017 KEY: 1=Strongly Disagree, 2= Disagree, 3= Fairly Agree, 4=Agree and 5= Strongly Agree Scale 1+2=Disagree and 3+4+5=Agree Table 2: Statements on Socio-Economic Issues Influencing Mental Health Programs.
Table 2 illustrates the socio-economic factors that influence mental health programs. Findings as per above table indicated that the high scores of 3+4+5 of 50% and above is an indication that majority of the respondents agreed that poor mental health programs are a consequence of social, economic and environmental inequalities, mental health consistently associated with unemployment, poor mental health is consistently associated with less education, low income or material standard of living, poor mental health is consistently associated, higher national levels of income inequality are linked to a higher prevalence of mental illness and low intervention programs, mental health problems have considerable negative consequences for quality of life in Figure 2 indicated some of the social factors that influence mental health conditions. Higher proportion (30%) of the respondents stated homelessness, this was immediately followed by 25% who said is due to poor conditions, 16.3% of the respondents stated unequal distribution of amenities, (12.5%) ethnic disharmony, while the remaining (10%) and (6.3%) affirmed demolition of housing and migration and displacement respectively.
low- and middle-income countries and the country is under-resourced and under-developed to finance mental health intervention programs. Socio-Cultural Factors Influencing Mental Health Programs.
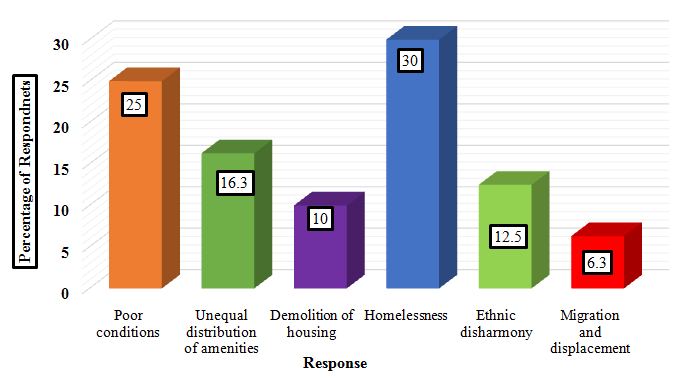
Source: Field Data, 2017 Figure 1: Factors that influence Mental Health Conditions.
Statement Response Frequency (N) Percentage (%)
Mental illness is caused by curses from the gods and ancestors Agree 151 83.7 Disagree 29 16.3 Total 180 100.0 Agree 124 68.7 Disagree 56 31.3 My Culture shapes the mental health programs and alter the types of services used.
Total 180 100.0
Agree 153 85.0 Disagree 27 15.0 Total 180 100.0
The attitude of some mental health practitioner deters us to seek for services.
Racial prejudice is the cause of differential treatment of illness.
Agree 155 86.3 Disagree 25 13.7 Total 180 100.0
Agree 135 75.0 Disagree 45 25.0 Total 180 100.0
It is often possible to identify cultural values directly concerned with the essential features of mental health.
Mental health is in manyways undervalued in our societies. Agree 167 93.7 Disagree 13 7.20 Total 180 100.0 Agree 180 100.0 Disagree 0 0.00 Total 180 100.0 Mental illness is associated with societal stigma and negative attitudes Agree 158 87.5 Disagree 22 12.5 Total 180 100.0 Mental health for a person is affected by social interaction, societal structures and resources and cultural values.
- Source: Field Data, 2017
Table 3: Issues on Socio-Cultural Factors Influencing Mental Health Programs.
Findings per the above table 4 illustrate some of the socio-cultural issues surrounding mental health programs. The study revealed that majority of the respondents between 70-100% all agreed that mental illness is caused by curses from the gods and ancestors, their culture can shape the mental health programs and alter the types of services used, the attitude of some mental health practitioner deters them to seek for services, racial prejudice is the cause of differential treatment of illness, it is often possible to identify cultural values directly concerned with the essential features of mental health, mental health is in many ways undervalued in their society, mental illness is associated with societal stigma and negative attitudes, and Mental health for a person is affected by social interaction, societal structures and resources and cultural value
Availability of Mental Health Intervention Programs
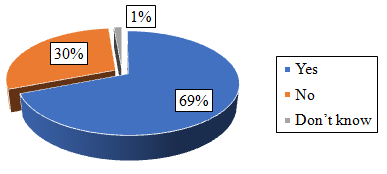
Source: Field Data, 2017 Figure 2: The Availability of Mental Health Intervention Programs in the Facilities.
time of the study; whiles (30%) of the respondents said there were mental health facilities.
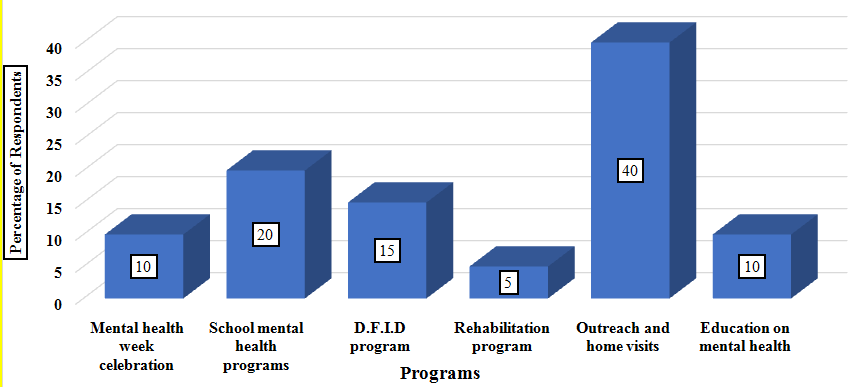
Source: Field Data, 2017 Figure 3: Mental Health Programs.
When respondents were asked to state the mental health intervention programs, (40%) of the respondents embarked on outreach and home visits, (20%) undertook school mental health programs, (15%) organized D.F.I.D (Department for International Development) program, whereas (10%) and (5%) indicated mental health week celebration, education on mental health, and rehabilitation program.
Programs Frequency (N) Percentage (%) National programs 2 10.0 Regional programs 1 5.0 District programs 3 15.0 Donors programs 2 10.0 Facility programs 12 60.0 Total 20 100
- Source: Field Data, 2017
Table 4: Nature/Type of Program.
Table 5 illustrates the type of health intervention programs. The study found that higher number (65%) of the respondents affirmed their programs were from the facility level, (15%) of the respondents indicated district programs, (10%) of the respondents indicated national and donor programs simultaneously, whiles only (5%) of the respondent stated regional programs.
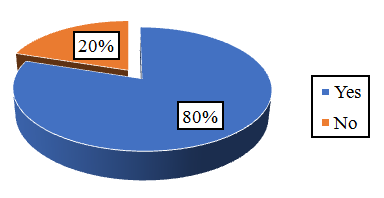
Findings as per above figure indicated that majority (80%) of the respondents attested the above- programs from figure 5 were not successfully executed while (20%) of the respondents affirmed that these programs were successfully executed.
| Source: Field Data, 2017Table 5: Challenges Affecting Mental Health Programs. | The study again concentrated on the socio-economic factors that influence mental health programs. The issues. It, therefore, implies that people have varied views on mental health issues in our society. |
| Data gathered from table 6 portrays the institutional issues. |
Table 5: Challenges Affecting Mental Health Programs.
Data gathered from table 6 portrays the institutional challenges that affect the mental health programs. When respondents were asked whether there were challenges affecting mental programs, all (100%) of the respondents unanimously affirmed there are challenges affecting mental health programs in their respective facilities. Among the challenges were, lack of financial support from the government (45%), inadequate infrastructure and logistics (25%), inadequate human resource (15%), Stigmatization and discrimination (10%) and lack of support from family members (5%).
Discussion of Results
Socio-Economic Factors Influencing Mental Health Programs
The study found some of the social factors that influence mental health programs. From the results, half (50%) of the respondents stated stigmatization and discrimination, poverty, insecurity and hopelessness, rapid social change and risks of violence, influence on health behavior, trust and social capital, and peer influence are socio-economic factors that influence mental health programs. It can be deduced from the findings above that there are social factors that affect mental health intervention programs. These social issues include internal and external variables that have implications for mental health and its corresponding intervention programs in Ghana. It is for this reason that [21] contended that the association between poverty and mental disorders appears to be universal, occurring in all societies irrespective of their levels of development. The study further elucidated that factors such as insecurity and hopelessness, rapid social change and the risks of violence and physical ill-health may explain greater vulnerability.
Participants commonly believed that people with mental illness are hard to talk to because of the changes in their emotional and physical appearance, when they open up, society will discriminate against them, they sometimes use words which does not make sense, interpretation between two parties becomes difficult, they can't communicate properly, they do not think the way normal people think, they don't know whether the person understands you or not and they seems not serious when you are talking to them about an important issues. It, therefore, implies that people have varied views on mental health issues in our society.
The study again concentrated on the socio-economic factors that influence mental health programs. The findings showed the high scores of 3+4+5 of 50% and above is an indication that majority of the respondents agreed that poor mental health programs are as a consequence of social, economic and environmental inequalities, mental health consistently associated with unemployment, poor mental health is consistently associated with less education, low income or material standard of living, higher national levels of income inequality are linked to a higher prevalence of mental illness and low intervention programs, mental health problems have considerable negative consequences for quality of life in low- and middle-income countries, and the country is under-resourced and under-developed to finance mental health intervention programs. It is therefore deduced from the study that respondents agreed on the socio-economic factors that influence mental health programs [3]. Indicated in a survey that mental health systems in many countries remain seriously under-resourced and under-developed. For this reason [22] argued that it is well established that mental illness, across the spectrum of disorders, is both a direct cause of mortality and morbidity and a significant risk factor for poorer economic, health and social outcomes, although these adverse outcomes vary by type of disorder and socioeconomic status. In the same vain evidence also indicates that mental ill-health is more common among people with relative social disadvantage [23]. This finding is consistent with [24] that stated the global burden of mental ill-health is well beyond the treatment capacities of developed and developing countries, and the social and economic costs associated with this growing burden will not be reduced by the treatment of mental disorders alone.
Socio-Cultural Factors Influencing Mental Health Programs
The study also uncovered some of the social factors that influence mental health conditions. It turned out that a higher proportion of the respondents stated homelessness, poor conditions, unequal distribution of amenities, ethnic disharmony, demolition of housing and migration and displacement.
On the availability of mental health facilities in the study area, the study found that majority of the respondents affirmed that there were no mental health facilities in their communities. This means that there is lack of mental health units for easy accessibility by mental health patients. It implies that the supply of community mental health facilities (e.g. office and clinic space) and resources (e.g. medication supplies and transport) to support community mental health practice is very insufficient_._ This therefore explains why most family members have no option than to consult people who have no skills in delivering mental health services. This study is consistent with [8] who argued that cultural misunderstandings between patient and clinician, clinician bias, and the fragmentation of mental health services deter minorities from accessing and utilizing care and prevent them from receiving appropriate care.
Data gathered from the study indicated that respondents consulted the spiritualist, pastor, herbalist, while just few consulted the mental health practitioner. Their option for consulting these people could be attributed to the fact that there were few mental health facilities within their location and also Ghanaians in general are spiritually minded when they are confronted with any eventuality. By the time the person is sent to the mental health officer/practitioner the condition might have been worse. Few of the respondents reported that they would like to go to a psychiatrist when they or their family members are suffering from mental illness.
Findings revealed the socio-cultural issues surrounding mental health programs. The study revealed that majority of the respondents, between 70-100%, all agreed that mental illness is caused by curses from the gods and ancestors, their culture can shape the mental health programs and alter the types of services used, the attitude of some mental health practitioner deters them to seek for services, racial prejudice is the cause of differential treatment of illness, it is often possible to identify cultural values directly concerned with the essential features of mental health, mental health is in many ways undervalued in their society, mental illness is associated with societal stigma and negative attitudes, and mental health for a person is affected by social interaction, societal structures and resources and cultural values. This findings is in line with [8] who contended that culture of the patient, also known as the consumer of mental health services, influences many aspects of mental health intervention programs, mental illness, and patterns of health care utilization. Also a survey by WHO [25] opined that there exist many misconceptions among the general public, politicians and even professionals regarding the concept of mental health. This is due to the fact that mental health is in many ways undervalued in our societies.
Availability of Mental Health Intervention Programs
The study found that majority of respondents affirmed that there were no mental health intervention programs at time of the study. When respondents were asked to state the mental health intervention programs, the following programs were stated: outreach and home visits, school mental programs, Department for International Development (D.F.I.D) program, mental health week celebration, education on mental health and rehabilitation program. It is deduced from the study that these programs stated by respondents were key activities that are undertaken by these facilities aside the mental week celebration. Thus, key mental health interventions are unavailable let alone looking at their effectiveness. Mental health officers therefore termed these activities as interventions but in reality there were no intervention program of these natures to help people with mental conditions.
Soliciting respondent’s views on the nature of these supposed programs outlined by respondents, majority of respondents indicated these were facility programs, while the rest were district, national, donors and regional programs. But unfortunately, the study found that vast majority of the respondents did indicate that these programs were not successfully executed partly due to inadequate funds, lack of psychiatric unit and nurses, and inadequate psychotropic drugs. This finding is therefore in congruent with [26] which argued that mental health services in Ghana are available at most levels of care. However, the majority of care is provided through specialized psychiatric hospitals (close to the capital and servicing only small proportion of the population), with relatively less government provision and funding for general hospital and primary health care based services with few community based services being provided are private. For this reason [16] opined that the scarcity of psychosocial interventions, psychotropic medication is the mainstay of treatment and has been the topic for further discussion.
Institutional Challenges Facing Mental Health Programs
This section looks at some of the institutional challenges that affect mental health programs. When respondents were asked whether there were challenges affecting mental programs, all (100%) of the respondents unanimously affirmed there are challenges affecting mental health programs in their respective facilities. It means that all the facilities providing mental health service have challenges in one way or the other. Among the challenges were, lack of financial support from government, inadequate infrastructure and logistics, inadequate human resource-thus World Health Organization (WHO) estimates that 1.18 million additional mental health workers are needed to close the mental health treatment gap in low- and middle-income countries [17]. Stigmatization and discrimination, and lack of support from family members. It can be noted that mental health challenges are documented worldwide: It is against this background that [26] argued that low- and middle-income countries allocate lower proportions of their national resources to health care, but the global disparity is much more marked when we look at expenditure on mental health services and treatments. This is consistent with Ghana Health Service report [22] which noted that the National Health Insurance Scheme (NHIS) which was passed in parliament in 2003 ensured universal healthcare services for all residents in Ghana. However, while it says mental illness is exempt from the insurance Scheme, it implies that patients with mental illness do not qualify to register with the Insurance Scheme. In fact, these challenges are not quite different from report by Ghana News Agency [27] where nurses from Accra Psychiatric Hospital decried the numerous challenges faced by the health facility, including lack of hospital supplies and consumables. These for them is risky because they could be harmed by the patients. Recent data collected by WHO demonstrates the large gap that exists between the burden caused by mental health problems and the resources available in countries to prevent and treat them [28].
Conclusion
The study found some of the social factors that influence mental health programs. The study found revealed that half 50% of the respondents indicated few of the socials factors such as; stigmatization and discrimination, poverty, insecurity and hopelessness, rapid social change and risks of violence, influence on health behavior, trust and social capital, and peer influence. The study revealed the socio-economic factors that influence mental health programs. Some of these economic factors were; economic and environmental inequalities, unemployment, less education, low income or material standard of living, higher national levels of income inequality, negative consequences for quality of life in low- and middle-income. Findings found the socio- cultural issues surrounding mental health programs. The study revealed that majority of the respondents between 70-100% all agreed that, mental illness is caused by curses from the gods and ancestors, culture can shape the mental health programs and alter the types of services used, the attitude of some mental health practitioner deters them to seek for services, racial prejudice is the cause of differential treatment of illness, mental health is in many ways undervalued, and societal stigma and negative attitudes, The study found that majority (69%) of the respondents affirmed that there were no mental health intervention programs at time of the study; respondents however indicated activities they undertake at their facilities level as mental health programmes. These were, outreach and home visits, school mental health , Department for International Development, (D.F.I.D) program, mental health week celebration, education on mental health, and rehabilitation program. It was thus explained that these activities were not successfully executed because of institutional key challenges.
All (100%) of the respondents unanimously affirmed there are challenges affecting mental health programs in their respective facilities. Notable among these challenges were lack of financial support from the government, inadequate infrastructure and logistics, inadequate human resource, Stigmatization and discrimination, and lack of support from family members. Mental health challenges can affect anyone regardless of race, gender, education, religion, age, intelligence or income. They are not the result of personal weakness, lack of character, poor upbringing, or lack of faith. It is imperative to recognize people with mental conditions as human beings for they also deserve a decent life. Thus the principle of the Human Dignity must be observed as far as health delivery is a concern.
In conclusion, to improve access to mental health care in Ghana, the scaling up of mental health care services must be closely monitored, sensitive to cultural and social context, accompanied by extensive research, and supported by adequate funding.
Recommendations
Base on the findings the study recommends that: 1. Ghana Health Service and other health delivery agencies such as the Christian Health Association of Ghana should collaborate with the Ministry of Health to promote timely access to effective treatment of mental health conditions, including mild-to-moderate mental illnesses, in both community mental health and primary care settings and through co-location of health professionals to facilitate the referral to specialist mental health care, while ensuring the involvement of people living with mental health conditions in decisions about the appropriate care and treatment plan. References
1. World Health Organization (2014) Mental Health: a State of Well-being.
2. Keyes CLM (2002) The mental health continuum:
From languishing to flourishing in life. Journal of Health and Social Behavior 43(2): 207-222.
3. World Health Organization (2001a) Mental Health:
New Understanding, NewHope. In World Health Report.
4. Prince M, Patel V, Saxena S, Maj M, Maselko J, Philllips
M, Rahman A (2007) No health without mental health. Lancet 370(9590): 859-877.
5. Adomakoh CC (1972) Mental hospital patients: A
Castle Road profile. Ghana Medical. Journal 2: 65-71.
6. Barry MM, Jenkins R (2007) Implementing Mental
Health Promotion Oxford, Churchill Livingstone, Elsevier, pp: 376.
7. Brown ER, Ojeda VD, Wyn R, Levan R (2000) Racial
and ethnic disparities in access to health insurance and health care. , Los Angeles UCLA Center for Health Policy Research and The Henry J. Kaiser Family Foundation.
8. WHO (2001b) Basic documents, 43rd edn. Geneva,
World Health Organization.
9. Schieber G, Maeda (1997) A curmudgeon’s guide to financing health care in developing countries. Innovations in Health Care Financing, World Bank Discussion Paper No. 365.Washington, DC: World Bank.
10. Institute of Medicine (2000) Neurological, psychiatric and developmental disorders: meeting the challenge of the developing world, Committee on Nervous System Disorders in Developing Countries Institute of Medicine. National Academy Press
11. Florence I (2004) Cultural Issues in Mental Health
Care. Treatments in psychiatry: an update. The public health impact of mental disorders. Toronto, Hogrefe& Huber.
12. Mark R, Asare JB, Mogan C, Adjase ET, Akwasi O
(2013) The mental health system in Ghana. The Kintampo Project-Ministry of Health.
13. World Health Organization (2003d) Investing in mental health, Geneva World Health Organization.
14. Ghana health service (2014) Ghana health service
2014 Annual Report.
15. UNESCO (2006) Country profile: Ghana. Montreal:
UNESCO Institute for Statistics.
16. Fulton B, Scheffler RS, Auh E, Vujicic M, Soucat A
(2011) Health workforce skill mix and task shifting in low income countries: a review of recent evidence. Human Resources for Health 9: 1.
17. Mental Health Gap Global Action Program (2008)
Scaling Up Care for Mental, Neurological and Substance Use Disorders.
18. Ghana News Agency (2016). No Medicines for Mental
Health Patients.
19. Brink H (2006) Fundamental of research methodology for health care professionals. 2nd edition. Juta & Company LTD. Cape town, South Africa
20. Patel V, Kleinman A (2003) Poverty and common mental disorders in developing countries. Bulletin of the World Health Organization 81(8): 609-615.
21. The world health report (2005_)._ Changing history.
Geneva, World Health Organization.
22. Desjarlais R, Eisenberg L, Good B, Kleinman A et a., (1995) World mental health: problems and priorities in low income countries. New York, Oxford University Press.
23. World Health Organization (2003) Mental health in emergencies: mental and social aspects of health of populations exposed to extreme stressors. Geneva: World Health Organization.
24. Vaillant G (2003) Mental health. American Journal of Psychiatry 160(8): 1373-1384.
25. WHO (2013) Comprehensive mental health action plan 2013–2020.
26. Ghana News Agency (2016) Psychiatric nurses begin ‘run from danger’ strike.
27. Keyes CLM (2008) Promoting and Protecting Mental
Health as Flourishing, a complementary strategy for improving national mental health. Am Psychol 62(2): 95-108.
28. World Health Organization (2017) World Health
Assembly Endorses Global Action on Dementia.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis