Harm Reduction Rise and Fall. The Lessons Learned from the Greek Experience, Challenges and Recommendations
Greece represent a unique case for investigating harm reduction policy since the unprecedented economic recession and the radical austerity programs coupled with the auxiliary effects of an unstable, punitive political environment created social challenges within which norms and community cohesion were undermined. The period 2010 to 2015 is of particular importance in Greece since the incremental devaluation of the social protection mechanisms, fragmentation of the NHS and absence of policy planning, narrowed vision reforms were implemented withholding resources from essential health and harm reduction services, while they were facing increasing demand. This study is part of a larger project investigating harm reduction investment at the EU. A qualitative follow up study was utilised to explore and provide additional insight of the precipitating factors of the HIV epidemic in Greece through the subjective interpretation of the key stakeholders at the time of the crisis. Triangulating data collection tools an explanatory sequential design was adopted in order to incorporate the experience and the views of those affected by the policies and in order to provide additional insight and to build upon the initial HRI quantitative results. Findings indicate that failure to disentangle policy harms is a major obstacle for the development of more effective evidence-based policy responses and sustainable harm reduction funding.
Introduction
During the economic downturn in Greece the cost- containment measures of horizontal cuts for reducing public expenditures combined with lacking strategic planning of resource re-allocation had severe consequences to users, citizens and the health care system. These auxiliary effects were disproportionate to the most vulnerable sector since beyond the direct socioeconomic effects of the crisis, they were also dragged into an unprecedented repressive and over-punitive response against them. The systemic structural weaknesses of NHS created a fertile ground for multiple public health related problems susceptible to exogenous variations and unable to meet the increasing needs of the population [1]. While low threshold harm reduction services were confronted by a sharp increase on demand their response capacity was dramatically decreased. This reverse analogy along with rapid course of disintegration of the basic structures of social protection, Greek society experienced an escalation of excessive and constant violation of drug users’ rights i.e. violence, intimidation and lack of access to essential harm reduction services. The effects of such over-repressive policies were particularly pertinent for the most vulnerable groups, splitting society and fostering a culture of discrimination.
The HIV outbreak, the increased rates of mortality related to accidental overdose from unknown purity and potency from illegal trade of new unknown, at that time, chemical compounds, the overcrowded penitentiary institutions due to massive incarceration of drug offenders with minor offences, the deprived neighborhoods and local communities from acquisitive crime and micro trafficking violence, or offences related to economically support drug consumption, portrait some of the adverse effects that have been attributed to the drug control policy responses. Under this prism, it appears that the costs and harms generated directly from drug control policies and the accompanying law enforcement practices were disproportionately higher than the intended good.
Background
Greece traditionally was tailored towards abstinence- based models, and in comparison, with other EU countries was slower on adopting harm reduction on the national drug policy. Greece belongs to the EU countries with the lowest coverage of needle and syringe provision as well as OST [2, 3], disproportionate lower when considering the drug misuse problem from the general population and the early on start of the disorder.
For many years the insufficient provision of Opioid Substitution Treatment (OST) in Greece was unable to correspond with the demand for services. As indicative in August 2010, more than 5.300 people were on the waiting list for OST; whereas the average waiting time in Athens was more approximately seven years. This combined with lack of programs to supply clean needles and low uptake of antiretroviral therapy for IDUs were predominant factors for the HIV outbreak [4, 5]. The negative societal attitudes and prejudice against harm reduction and lack of political commitment have influenced the development of harm reduction programming. The societal prejudices and opposition from local residents led on 2011 to the closure of four OST units in the centre of Athens resulting in the loss of 1.400 treatment slots, in a red zone area, an area with the highest concentration of IDU’s in Greece.
Part of the resistance and fragmentation of harm reduction development can be attributed to certain relevant stakeholders with different agenda and competitive interests, and strong influential voice in all levels of the political spectrum. Following a more moralistic approach, they were advocating against harm reduction programs and cultivating for years a mistrustful environment. Despite the efforts to raise awareness that the drug policy is not a bipolar, and that abstinence-based models and harm reduction are not competitive approaches but rather compatible and complementary, the drug policy dialog in Greece remained fragmented and polarized relying on outdated rehabilitation concepts and ideological preconceptions. This arbitrary dichotomization and combative climate provided a limited space for investigating policy alternatives and reaching consensus on this controversial policy, hindering in this way, the development of harm reduction legislation and implementation.
Methodology
Choice of Methods
This project aimed to fill a major knowledge gap and increase the capacity of civil society organizations to track national spending and to assess funding shortfalls. The methodology for this review suggests the study design, the data sources and strategies that were used to answer these questions and the analytical tools to analyse the data. Pragmatic rationality implies the choice of the most appropriate approach to data collection and analysis depending upon the research questions [6]. In order to provide additional insight from the HRI quantitative findings, an explanatory sequential design was adopted. This two-phase mixed methods design was utilized in order to build upon the initial HRI quantitative results by using qualitative data from the interviews and the focus group discussions [7, 8].
The follow-up explanations model focuses on a more detailed examination of the results. Since the quantitative analysis in the study was based on HRI protocols and compared data from other countries as well, the researcher was interested to analyze country specific findings, thus the need of additional exploration was required. The second qualitative phase was utilized to collect text data through individual semi-structured interviews, in order to elucidate and supplement the quantitative findings and provide additional insight of the Greek harm reduction contextual reality that may “reveal the story” behind the quantitative associations. Therefore, the grounds for the utilization of qualitative approach in this study refer to: a) Understanding quantitatively the harm reduction landscape in Greece, b) Complementing and questioning the results of the quantitative data, and c) Informing the design of the quantitative research. Thus, the role of the qualitative method in this study was to elucidate and provide additional insight of the precipitating factors of the HIV epidemic in Greece through the subjective interpretation and experience of the key stakeholders at the time of the crisis.
Overall, the practical utility of mixed methods appears to be appropriate in understanding and responding to the public health challenges related to drug policy initiatives. One of the basic advantages of this method refers to reduction of inappropriate certainty and strengthening triangulation and interpretability, corresponding in this way to growing complexity of social and health care issues that demand creative investigation [9].
Research Questions
The study seeks to answer the following overarching evaluation questions: 1) What is the level and source(s) of current financial investments in harm reduction programming within the country? And which interventions are supported by this investment? 2) What are the main funding gaps and challenges? And to what extent does funding go towards priority interventions; 3) Which government departments/ministries currently holds budgets that includes funding for harm reduction programming? And what is the decision-making process on resource allocations for harm reduction at the national and local level? 4) How the information revealed could be used for resourcing advocacy purposes?
Data Sources and Data Collection Instruments
The Data Collection was Based from the Following Sources: Desk based review and documented material.
The review involved relevant documentation from governmental and non-governmental institutions on harm reduction expenditures, investments and programs. In addition, other documentation through literature searches in both the academic and grey literature. For this purpose, a search strategy has been developed.
Stakeholder consultations including the experience and the views of those affected by the policies and involved in their implementation is a valuable tool for transparent and informed policy-making. This was performed in several targeted consultations with diverse stakeholders and service users in order to collect data on the current situation of the financial investments in harm reduction programming and the interventions that are supported with this investment. All relevant stakeholders had the opportunity to express their opinion, have sufficient time for their responses and they were provided with adequate feedback regarding the consultation process, its aims and goals.
Consultation Strategy
Step 1: Objectives of the Consultations based on the stage of the project circle, the objectives of the consultations with the stakeholders were:
- Gather evidence and factual information data and knowledge that will help to estimate the financial investments in harm reduction programming and the interventions that are supported with this investment as well as the potential effects on the performance of the existing harm reduction policy
- Collect views, opinions and gather new ideas of the relevant stakeholders in order to identify funding gaps and challenges, possible policy impact of punitive and repressive policies; explore new ideas and alternatives for harm reduction sustainability.
- Assess existing resource allocations schemes, ideas and analysis; Investigate decision making on resource allocations for harm reduction from diverse stakeholders; cross check and validate existing information or analysis; and explore different harm reduction priority issues on related investments. The Step 2 of this explanatory sequential design was the Stakeholder mapping in order to involve the identification of the target group that will be consulted. The selection criteria for the identification of stakeholders’ categories involve a) those affected by harm reduction policies b) those who formulate and implement harm reduction policies and c) those that have knowledge and expertise and are active in the harm reduction field.
Interviews
The researcher conducted several semi-structural interviews based on topic guide with the relevant stakeholders. Data obtained from the semi-structured interviews with the relevant stakeholders provided a thorough understanding on the harm reduction investment, their capacities, resources, needs and gaps. The predefined questions of the interview protocol were based mainly on the investment tracking tool, but also included thematic areas from the online survey both provided by HRI. The interviews were conducted in the stakeholder premises and lasted approximately two hours. In each interview, the questions were adjusted according to the stakeholder’s expertise. As an example, for OKANA (Organization against Drugs) which is responsible for the substitution treatment in Greece, the questions were targeted on OST, while in the interview with KEELPNO (Hellenic Centre for Disease Control and Prevention), the questions were targeted on ART, etc. Active involvement of the beneficiaries & target groups enabled better understanding of their problems, highlight potential methods of addressing them and set the grounds for the participatory planning process. The structural interviews involved thematic areas that cover: Demographics such as the total number of people received OST; the number of people who inject drugs living with HIV on ART nationwide; national spending on OST, NSP, ART; Programmed spending with breakdowns for OST, NSP, ART; Coverage nationwide OST, NSP, ART and contribution of international funding; Funding allocation and decision making; Funding challenges and gaps; and sustainability of harm reduction.
Focus Group Discussion (FGD)
At the second stage, Focus Group Discussions (FGD) were conducted to gather information on harm reduction, identify potential problems, funding gaps and challenges, as well as explored the distribution of harm reduction funds. The researcher as a facilitator of the group used the topic guide to organise a discussion among participants. The topic guide included a set of structured questions to steer the discussions. A note taker recorded the participants’ comments. The FGD took place at the Greek National Drug Coordination office and lasted approximately two hours. The FGD consisted of 8 staff members from the identified organizations. Participants were notified of the topic in advance and explained how the information will be used. The participation of these individuals was voluntary, based on their consent. The topic guide of the FGD assessed areas related to: Source, allocation and distribution of harm reduction funds; Advocacy for harm reduction investment; Funding gaps and trends; and future funding landscape for harm reduction programmers. The FGD complemented and supplemented the information obtained from the surveys, providing critical information for triangulating survey and interview data from the participating sites. At the second stage, the findings from both stages were validated. This was achieved by creating a ‘map’ of funding gaps ‘hotspots’ and challenges that were prioritized. The list of the interviewees along with their contribution can be found in Table 1. Beyond one organization all invited relevant stakeholders and policy makers responded positively and contributed to both the interviews and the focus group discussions.
| Organization | Topic | Interviews | FGD | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ministry of Health and Social Solidarity | Policy formulation /OST / ART / NSP | Yes | Yes | ||||||||
| National Drug Coordinator Office | Policy formulation /OST / ART / NSP | Yes | Yes | ||||||||
| EMCDDA National Focal Point | OST / ART / NSP | Yes | Yes | ||||||||
| OKANA (Organisation Against Drugs) | OST / NSP/ Advocacy Treatment | Yes | Yes | ||||||||
| KETHEA (Therapy Center for Dependent individuals) (TC) | Advocacy/ Treatment | ||||||||||
| No | No | ||||||||||
| KEELPNO (Hellenic Centre for Disease Control and Prevention) | ART / NSP | ||||||||||
| Yes | Yes | ||||||||||
| Special Infection Units (ΜΕΛ - Μονάδες Ειδικών Λοιμώξεων) | ART | ||||||||||
| Yes | Yes | ||||||||||
| OKANA Service Users Association | Advocacy | Yes | Yes | ||||||||
| NGO Praxis | Advocacy | Yes | Yes | ||||||||
| NGO the Center for Life | Advocacy NSP | Yes | Yes | ||||||||
| NGO Positive Voice | Advocacy NSP | Yes | Yes | ||||||||
| NGO DIOGENIS association | Advocacy NSP | Yes | Yes | ||||||||
| NGO Hellenic Liver Patient Association “Prometheus” | Advocacy NSP | Yes | Yes |
Table 1: Beyond one organization all invited relevant stakeholders and policy makers responded positively and contributed to both
Data Collection Tools
Three data collection tools were used for the study. The first was the Investment Tracking Tool provided by HRI and allowed to capture the investment into harm reduction, the sources of funding and how these funds have been spent (e.g. interventions, geographical area and particular groups reached). The second was the Harm Reduction Works! Also provided by HRI and consists on an online survey that also assisted capturing the source, allocation and distribution of harm reduction funds, funding gaps and trends as well as future funding landscape for harm reduction programs. The first two provided mostly quantitative data and main findings can be found on the HRI report Harm reduction investment in the European Union, Current spending, challenges and successes, 2017.
Data Analysis
Data analysis was conducted in collaboration with HRI researchers from both quantitative and qualitative data and can be found in the above mention report. In addition, content analysis was utilized in order to review the qualitative data and identify themes which emerge from the written data and the information provided on the interviews and the FGD. These themes were analysed in order to answer the main questions of the study and showcase the good practices as well as the harm reduction funding crisis. The application of mixed methods involves knowledge-building based on pragmatic principles, affirming that truth is “what works” [7].
Results
The response to outbreak - Harm reduction’s rise and fall The rapid increase in HIV among people who inject drugs was first highlighted in 2011, when 266 was reported in Athens and increased sharply the following year 551 IDU (Figure 3). This public health emergency came at a time of extreme social instability in Greece, with basic social structures at risk of collapse, a fast, cost- efficient response was required [10].
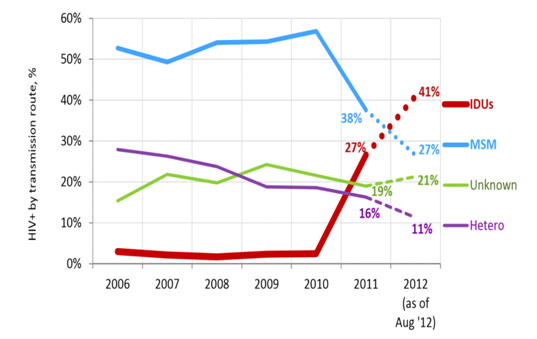
Source: HCDCP, Data presented at the ECDC Technical Mission held in Athens on September 10, 2012.
Following consultation with International and EU expert bodies, a scale up of targeted harm reduction intervention took place, funded mainly from the European funds under the National Strategic Reference Framework (ESPA) [11, 12, 13, 14]. During 2012 the first year of the outbreak, the Organisation against Drugs (OKANA) increased the number of centers providing OST by 132%, opening an additional 33 centres [5]. As a result, the number of patients on OST increased by 45%. This decreased the treatment waiting list by 49% and reduced the waiting time by 52% in Athens (from 90 months to 44 months) and by 99% in Salonica (from 48 months to 2 weeks).
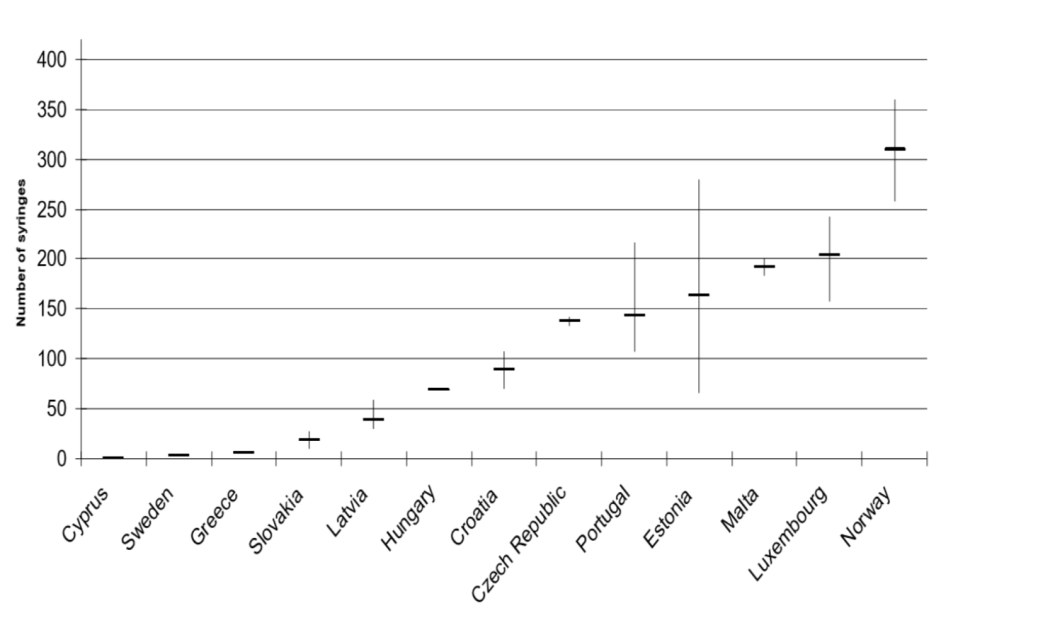
However, even with these vast increases, OST in Greece did not reach UN-recommended coverage levels EKTEPN. When counting total number of syringes per user in Greece for the 2014 were 70 syringes/user (367.258 syringes) which indicates that the NSP levels were very low and that there is a decreasing trend of service provision as well, since for 2013 the number of syringes per IDU were 81 (429.517) [15, 16]. Thus, despite the significant steps that were taken in response to the escalating nature of the outbreak covering the majority of the proposed interventions, the frequency and the intensity were not at the sufficient levels [17]. Also, many of these services did not continue to operate due to lack of financial resources, which had a direct impact in drug users and the health services. The significant expansion of OST program and their integration with the public hospitals, still nowadays cannot meet the current treatment demands, with a waiting list of more than 2.500 people. A pilot drug consumption room, named ULYSSES, opened in Athens in 2013 was closed after 10 months of operation, despite a positive and significant impact on the health of people who inject drugs, due to a lack of political will to put supportive legislation in place.
Furthermore, the greatest achievement was the collaboration and the development of a network between government and non-governmental agencies led by OKANA and consisted initially by treatment organizations and NGOs active in the harm reduction field. Through active inter-agency collaboration initiated a well-designed outreach work with distribution of hygienic kit and other important preventive activities. The network integrated public hospital, emergency drop in centres and other Open Assess Services (OAS). The network scaled up needle and syringe programmes by 180% to increase the meagre coverage of seven syringes per person per annum in 2010, to 45 in 2012 [10]. This service expansion was reflected in a substantial downward trend in new HIV cases among injecting drug users, from 213 in 2011 and 514 in 2012 to 239 in 2013 and 84 in 2014 HCDCP,. Therefore, since the HIV outbreak there was a rapid response that increased harm reduction coverage despite the severe budget cuts. Concurrently, the ARISTOTLE programme was initiated with the aim to identify IDUs, to examine and refer them to the Infectious Diseases Units in case they were found HIV positive. By combining laboratory testing with education and linkage to treatment, the ARISTOTLE programme successfully reduced incidence of infection in this population and demonstrated the cost-effectiveness of harm reduction strategies. The model raised awareness of harm reduction efficacy and cost-effectiveness and promoted community networking and the concept of shared care. But above all increased community and relevant stakeholders’ readiness to accept, adopt and implement contemporary evidence-based harm reduction interventions. This was a significant achievement considering that the main challenge was the resistance and the negative attitudes towards harm reduction [18].
This community-based harm reduction approach influenced the national drug policy and provided a platform to move from the short-sighted drug policy responses to more coherent, well-designed comprehensive package of harm reduction interventions. HCDCP conducted a mapping of relevant national bio- behavioural surveillance data in close collaboration with main national stakeholders including NGOs, Greek Reitox Focal Points, Drug Treatment Services, Academia and Ε.Υ.τ.Υ.Κ.Α responsible for NSRF of Health Sector. HCDCP drafted a protocol for Data Submission of relevant bio- behavioural data necessary for monitoring and evaluation purposes in close consultation with national stakeholders, European team of experts and ECDC. The protocol focuses on improving the comparability, timeliness, quality and coverage of the data collected in Greece and harmonizing with data collection procedures on key indicators under the European and international requirements.
Regrettably, this form of harm reduction emancipation based on an integrative community based inter-sectoral response ended with the first indications of the downward in HIV. Seeking for answers and potential explanation, it may be that this was a spontaneous movement developed by the need to respond to a direct threat to society, while ended its mission after having served its purpose. From this perspective, as a crisis intervention, its temporality is justified as the aim was to restore equilibrium and stabilization. What makes the difference between a crisis intervention and a sustainable organized community-based harm reduction system is that the latter requires the organizational structure and the coordinating mechanisms in place in order to be sustainable and effective. The small increase of governmental funds as a response to the outbreak, lasted only for a year, since with the first indicators of HIV reduction, authorities initiated financial cutbacks reducing at a great extend the intensity and frequency of the harm reduction interventions and threatening their sustainability. The Greek authorities should serious consider the recommendations to provisionally exclude harm reduction programmes and ART treatment from public spending cuts in order to prevent another outbreak and protect IDUs and the public health EKTEPN. Furthermore, study findings indicated that the transparency of spending data was from the weakest elements in the Greek drug policy as shown in the Table 2. a traffic light system categorises the national situation as poor (red), mediocre (amber) or good (green) on the
| Harm reduction coverage | Transparency of spending data | Government investment in harm reduction | Civil society view on the sustainability of funding | |
|---|---|---|---|---|
| Bulgaria | ||||
| Romania | ||||
| Poland | ||||
| Hungary | ||||
| Greece | ||||
| Lithuania | ||||
| Italy | ||||
| Sweden | ||||
| Czech Republic | ||||
| Portugal | ||||
| Finland | ||||
| Estonia | ||||
| UK | ||||
| Ireland | ||||
| Belgium | ||||
| France | ||||
| Germany | ||||
| The Netherlands |
Table 2: Harm Reduction funding in the European Union at a Glance.

Lessons Learned and Future Steps
Recommendations Based on Study Findings: The socio economic conditions in Greece and the pressure from donors, required cost-effective responses, in order to improve quality and raise standards of care with the use of limited available resources. An integrative community- based harm reduction approach would provide several advantages. An inter-sectoral approach beyond its cost effectiveness, the common use of existing infrastructures and local resources, would improve also the quality of services within existing programs as it provides a more comprehensive package of care and it is designed to correspond to the diverse needs by matching individuals to the appropriate levels of care.
Maximized efficiency in the use of limited resources and facilitate the integration of harm reduction into existing community services. Fostering harm reduction accessibility making services more accessible and offers services in a neutral site and Open Access Services-OAS (e.g. mobile units; street agencies). This will increase service efficiency and reduce costs, since it will offer more comprehensive array of service responses aligned with true service user needs. Acknowledging individuals exhibit different problems in terms of severity, intensity and frequency that require different levels of care, this system will be designed to correspond to this diversity by matching individuals to the appropriate levels of care.
Secured response specificity through Drug Referral Schemes (DRS) and a placement system model. Providing structured, multi-disciplinary, and task-oriented enable users to be placed on the most appropriate service to meet their needs. Beyond the cost effectiveness, integrated care pathways improve effectiveness and the quality of care, since individuals may have multiple problems that require effective coordination among services or may have continuous care needs requiring referral to a different level of service over time.
The socioeconomic crisis and the HIV outbreak as catalysts of change generated reforms and facilitated the acceptance and implementation of harm reduction, which until then it was a highly controversial, stigmatized and purposefully neglected. However, there is a long way and many obstacles to overcome in order to reach the desirable levels of political consensus for an evidence based resource allocation in the drug policy arena. Beyond the relevant policy makers (un)readiness, it is the right the time and the appropriate contextual conditions for the implementation of contemporary evidence based and impact oriented drug policies in Greece. The lifesaving preventative interventions and their positive impact to the community contributed on reducing the longstanding resistance and prejudices toward harm reduction and on gaining widespread recognition and support. The most validating and restorative for the harm reduction field, is the fact that those who for years were opposing and propagating against harm reduction in Greece, during the outbreak and the fragile contextual environment, were active participants investing a significant amount of their resources on harm reduction outreach interventions. This is an important lesson learnt for policy makers, relevant stakeholders, potential donors and the community.
From Punitive and Repressive Justice System towards Health-Based Community Policing and Therapeutic Jurisprudence
This shift in attitudes about harm reduction and a compassionate, human rights approach is emerging at a time when law enforcement and policy makers had orchestrated an unprecedented repressive and over- punitive approach towards the vulnerable sector. Constant violation of human rights and systematic use of violence, over-repressive and punitive interventions including sweep operations with arbitrary massive arrests, forced medical examinations, detention camps and preventing access to harm reduction services was the ‘new Greek law enforcement model’. The effects of such over-repressive policies and the punitive, discriminatory attitude of the Greek authorities towards to most vulnerable sector, split society, foster a culture of discrimination and threaten the achieved progress made so far on respect of human rights and the rule of law. Several scientific communities, NGOs and international agencies such as the UNAIDS and the Human Rights Watch have expressed strong reactions, condemning the interventions made by the Greek authorities.
In Greece, despite the new Law on drugs that introduces effective alternative measures and other crime prevention policies, its implementation is lacking, in practice there is a significant proportion of pretrial detention and mandatory minimum sentences for drug users with non-violent minor offences. Another interesting and compelling finding of this study is current inhuman and degrading conditions of the Greek penitentiary institutions. The disproportional incarceration of drug users, as well as lack of imprisonment alternatives for drug depended individuals causes significant overload for the criminal justice system and undermine the notion of proportionality and fairness of the law. This is reflected by the fact that Greece has one of the highest levels of incarceration for minor non- violent drug related offence, with 1/3 of the prisoners is serving terms for drug offenses. Also, Greece has the fourth most overcrowded prisons in Europe, with 121 inmates for every 100 available places compared to a European average of 94 per 100. The lack of access and availability of health care and harm reduction services in prisons raise serious ethical and moral concerns.
Furthermore, the study findings also indicated that there are significant legislative barriers such as lengthy bureaucratic procedures and the unwillingness and reluctance of the prison administration to adopt and implement harm reduction interventions in prisons. These findings are in line with the alarming report of the European Committee (EC, 2015), indicating that the situation in the Greek prisons has become critical and that urgent action is required for their recovery, starting with tackling the excessive overcrowding, the excessive use of power, corruption and malpractices from all prison personnel from top down and the widespread deficiencies regarding access to health care and health-care policy regarding drug misuse. The threat for expansion of another HIV outbreak potentially within prisons is considerable and the need for harm reduction measures very apparent. Under this prism, it is imperative to develop efficient policy evaluation framework to assess the potential adverse effects and associated costs of drug control policies. This could provide the basis for mobilizing the efforts to encourage policy reform and the implementation of contemporary approaches in the penal system based on the principles of restorative justice and therapeutic jurisprudence. Economic downturn in Greece created an evolving stance and an opportunity to act towards innovative initiatives and contemporary, organized and impact-oriented drug policies.
There is a pressing need to further expand and empower this inter-sect oral collaboration by involving all relevant sectors of the society, especially the law enforcement. Harm reduction advocates and relevant stakeholders should use this ‘harm reduction momentum’ to convert the spontaneous crisis intervention that temporary arise in Greece as a response to the HIV outbreak to a sustainable best practice harm reduction model. A strategic framework that through inter-sectoral coordination mechanisms, evidence-based and community-based assets make efficacious use of multiple partnerships to meet identified needs within a framework that promotes sustainable and place-specific harm reduction interventions [19]. Secondly, police involvement in harm reduction activities will not only terminate the series of unintended related harms i.e. Hindering harm reduction services; poorly violation of users rights; harassment, extortion, torture and ill treatment, judicial corporal punishment for drug offenders, arbitrary detention, and denial of basic health services, but it will also provide a cost effective model that utilizes the available community resources wisely and efficiently. This model will complement public health and harm reduction goals and will be an additional positive component on addressing the health and social needs of vulnerable populations. The development of good practice guidelines for police will facilitate the transitional phase from punitive adversarial law enforcement towards harm reduction-based approaches to law enforcement.
Overall, it is evident that legislative gaps concerning harm reduction in Greece generates major problems in practice (closure of supervised consumption rooms, police confronting users and street workers hindering service delivery). Moreover, implementation of punitive adversarial laws in a form of legal action towards practitioners (prosecuting, harassing frontline workers) for providing harm reduction preventive services, may lead to “defensive practices” and further alienate this already overburdened section of professionals in the drug prevention field. The punitive stance adopted by the Greek authorities with the swiping operations, destroying injecting equipment, police arrests and confiscation; preventing drug users access to health; and penal- centered practices i.e. criminalization of HIV lead to further degradation of NHS, devaluate harm reduction street work, and influence professional liability in the addiction field [20]. Taking into consideration the significant staff turn-over, lack of carrier paths and absence of reinforcement for new practitioners to engage in harm reduction in Greece, this approach could seriously damage the provision and quality of the services, distancing new practitioners due to risk of unclear professional liability.
It must be highly prioritized to implement community based policing and foster police role as a health promotion agents with participation in preventive harm reduction programs i.e. overdose reversal, street work with psychoeducation and targeted referrals. This will also facilitate the resource relocation process from law enforcement repressive operations towards prevention and other social welfare initiatives [21].
Concluding Remarks
Another important parameter is that the side-effects of certain measures have not been taken into account adequately. Many of the policy interventions created unintended effects. Failure to disaggregate these drug control policy harms is a major obstacle for the development of more effective evidence-based policy responses and sustainable harm reduction funding. Further research is needed that focuses on cost-benefit analysis, this beyond a valuable research tool for accurate policy mapping, monitoring and demonstrating the cost effectiveness of the successful harm reduction initiatives, but also as a warning mechanism of the unintended consequences of hindering such interventions. This will improve the knowledge base and understanding of how different policies have various effects and consequences at a macro and micro level as well as the extent to which the current drug control measures respond to the vulnerable groups. Considering the lack of research and evidence-based advocacy in Greece, a research/advocacy platform will enable to build mutually beneficial innovative synergies that bridge the gap between policy, research and practice through collaborative planning process and foster co-production of research and knowledge.
References
-
Karanikolos M, Mladovsky P, Cylus J, Thomson S, Basu S, et al. (2013) Financial crisis, austerity, and health in Europe. The Lancet 381(9874): 1323-1331.
-
EMCDDA and ECDC (2012) Joint EMCDDA and ECDC Rapid Risk Assessment HIV in Injecting Drug Users in the EU/EEA, Following a Reported Increase of Cases in Greece and Romania. European Monitoring Centre for Drugs and Drug Addiction, pp: 1-16.
-
EMCDDA (2011) ECDC and EMCDDA guidance Prevention and control of infectious diseases among people who inject drugs. ECDC, Stockholm.
-
Malliori M, Golna C, Souliotis K, Hatzakis A (2013) Managing opioid dependence treatment and controlling for HIV incidence among injecting drug users in Greece: a case study of optimism in the face of adversity. Addiction 108(6): 1174-1175.
-
Malliori M (2011) Early-warning message to EMCDDA, EMCDDA early-warning system report.
-
Hanson WE, Creswell JW, Plano Clark VL, Petska KP, Creswell JD (2005) Mixed methods research designs in counseling psychology. Journal of Counseling Psychology 52(2): 224-235.
-
Creswell JW (2002) Educational research: Planning, conducting, and evaluating quantitative and qualitative research. 4th(Edn.), Upper Saddle River, NJ: Merrill/Pearson Education, pp: 1-673.
-
Tashakkori A, Teddlie C (2003) Handbook of mixed methods in the behavioral and social sciences. Thousand Oaks, CA: Sage Publications.
-
Robson C (2002) Real World Research. 2nd (Edn), Oxford: Blackwell.
-
Papamalis EF (2017) Harm reduction investment in the European Union Current spending, challenges and successes. London: Harm Reduction International, pp: 25-28.
-
European Centre for Disease Prevention and Control (2013) Joint technical mission: HIV in Greece 28-29 May 2012. Stockholm: ECDC;
-
European Monitoring Centre for Drugs and Drug Addiction (2011) Data: statistical bulletin 2011. Lisbon: EMCDDA.
-
WHO, UNODC, UNAIDS (2009) ‘Technical guide for countries to set targets for universal access to HIV prevention, treatment and care for injecting drug users’, WHO, Geneva.
-
WHO, UNODC, UNAIDS (2007) Interventions to address HIV in prisons: drug dependence treatments. Evidence for Action Technical Papers, Geneva.
-
Paraskevis D, Hatzakis A (2011) An ongoing HIV outbreak among intravenous drug users in Greece: preliminary summary of surveillance and molecular epidemiology data’, EMCDDA early-warning system report.
-
Fotiou A, Micha K, Paraskevis D, Terzidou M, Malliori M, et al. (2012) HIV outbreak among injecting drug users in Greece: An updated report for the EMCDDA on the recent outbreak of HIV infection among drug injectors in Greece, Athens, pp: 1-51.
-
Paraskevis D, Nikolopoulos G, Tsiara C, Paraskeva D, Antoniadou A, et al. (2011) Hiv-1 outbreak among injecting drug users in Greece, 2011: a preliminary report. Euro Surveill 16(36): 19962.
-
Paraskevis D, Nikolopoulos G, Fotiou A, Tsiara C, Paraskeva D, et al. (2013) Economic Recession and Emergence of an HIV-1 Outbreak among Drug Injectors in Athens Metropolitan Area: A Longitudinal Study. PLOS ONE 8(11): e78941.
-
Papamalis EF (2012) Economic recession and treatment of substance misuse: The need for community resource-driven approach. In 6th Adriatic Drug Addiction Treatment Conference, Tirana, Albania
-
Greek Centre for Disease Prevention and Control (2014) HIV infection: recent epidemiological data.
-
MacDonald MA (2005) Study of health care provision, existing drug services and strategies operating in prisons in ten countries from central and eastern Europe. The European Institute for Crime Prevention and Control Helsinki, Heuni, pp: 1-23.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis