Body Image and Adaptation Strategies in Breast Cancer Patients at Selected Stages of the Disease
Objectives: The aim of this study was to demonstrate how body image and coping strategies change at certain stages of breast cancer. Research Approach: longitudinal study Sample/Participants: The study group consisted of 100 breast cancer patients. Half of them qualified for mastectomy and the other half for breast conserving therapy. Methods: The study was conducted using the following tools: the mini-Mental Adjustment to Cancer (mini-MAC) scale, the Multidimensional Body Self-Regulation Questionnaire (MBSRQ), and a sociodemographic survey. Findings/Conclusions/Interpretation: The obtained results suggest that the type of the procedure does not affect the body image of breast cancer patients—what matters is the fact of undergoing surgery and facing a life-threatening situation. In addition, we found that disease coping strategies and body image change in subsequent stages of the disease. Implications for Psychosocial Providers or Policy: The longitudinal nature of the study broadens the overview of issues concerning body image and strategies for coping with disease adopted by patients. Our conclusions can help develop appropriate therapeutic plans for certain groups of patients
Introduction
The number of women diagnosed with breast cancer has been consistently growing [1]. Each patient perceives the disease in their own way, depending on the resources they have and the coping strategies they adopt [2]. Subsequent stages of the disease involve severe stress, a variety of emotions, and behavioural changes [3, 4]. These reactions may vary throughout the course of the disease, depending on the medical procedures used and the nature there of Conley et al., Hopwood et al., [5, 6]. The attitude of patients towards particular forms of medical treatment is of utmost importance when making decisions about starting the therapy [7]. Each type of therapy has certain psychological consequences which are often more difficult for the patient than the symptoms of the disease itself [8, 9]. Patients emphasize the importance of accepting their diagnosis, seeking social and emotional support, and getting involved in physical activity [10]. Finding positive meaning in the disease helps a patient cope better. This can broaden the spectrum of positive disease coping strategies [11, 12]. Coping with a disease is a significant individual regulatory process of an individual. This is related to health resources, which help restore the distorted inner balance and allow both short-term and long-term adaptation to disease-related problems and difficulties [13, 14, 15]. In these terms, it is also worth analysing the impact of body image on coping with breast cancer. The effects of the disease on one’s body may evoke a great sense of shame and decrease one’s sense of being attractive, leading to the formation of a negative image of one’s own body [16]. All medical interventions may cause physical and mental changes that affect body image in women suffering from breast cancer. Surgical procedures may influence a woman’s perception of her own attractiveness and quality of life [17], because any such intervention is associated with burdensome biological and emotional side effects, and changes to one’s body can be particularly traumatic when they interfere with its functioning [18]. The loss of significant feminine attributes such as hair or breasts is highly important in these terms. Patients may be left with a sense of inadequacy, exclusion, and uncertainty about their place in contemporary society, which presents itself as a group of beautiful and healthy people [19, 20, 21]. The literature on the subject contains research results that indicate the impact of surgical interventions on body image. Undergoing surgery is associated with great stress, shame, and difficulties with experiencing one’s own attractiveness [22, 23, 24]. Surgical procedures may have many emotional consequences, such as reduced self-esteem, lack of acceptance of one’s body, and perceived loss of femininity, attractiveness, sexual appeal, and relations with friends and family [21, 25, 26, 27, 28, 29]. Studies have shown that before and immediately after direct surgical procedures, patients can activate strong defence mechanisms to reduce negative emotions and create a sense of ease. Patients can utilize constructive strategies for coping with the disease. In the long run and after treatment, the strength of the defensive mechanisms weaken, which may cause the patient’s emotional state to deteriorate. Women with breast cancer, regardless of the stage of the disease, more often use constructive strategies (such as fighting spirit and positive revaluation) however, their degree of intensity varies throughout the course of the disease [30]. Taking into account the current research findings, an attempt has been made to broaden the knowledge about the long-term body image of women with breast cancer and their adaptation to the disease in the case of two types of surgical procedures: breast conserving therapy (BCT) and mastectomy. Selected studies on this subject in Polish and other languages provided inspiration to explore this matter in more depth and to investigate the impact of the type of surgery and the time elapsed after the procedure on the above-mentioned psychological aspects.
Procedure
The measurements were taken one week before BCT and mastectomy, and then three months and one year after the surgery.
Research Hypotheses
Based on the literature, the following hypotheses were formulated:
- Women with breast cancer assess their body worse after the surgical intervention than before.
- Women with breast cancer adopt different styles of coping at different stages of the disease.
- Independent of the type of surgery, patients most often use constructive coping strategies, rather than destructive ones.
Study Group
The study group consisted of 100 women with breast cancer who had known about their disease for at least one month. None of the women had ever suffered from a different type of cancer and each of them had a healthy BMI. All women were medically supervised by the same oncological surgeon who performed the surgical procedure on them. A total of 50 patients underwent BCT, and the 50 other women underwent mastectomy. The following inclusion criteria that had been taken in to the account, on choosing a particular treatment method: the stage of the cancer according to the TNM classification, the type of prognostic factors, patient’s general health state, the presence of comorbidities and prior treatment [31, 32, 33]. The following contraindications to qualify patients for sparing treatment had been also considered: a cancer focus larger than 3 - 4 centimeters in diameter, signs of skin and chest infiltration, multifocal cancer, presence of extensive intraductal component around the tumor, bilateral carcinoma, bariatric localization, inability to achieve a good cosmetic result, local recurrence after sparing treatment, extensive microcalcifications visible on mammography, presence of a BRCA1 or BRCA2 mutation or p previous history of breast radiation therapy [32, 34]. Moreover, the patients included in the presented study no had previously reported mental disorders or mood disorders in their medical history (conducted by a surgical oncologist), and described their mental state as stable (the group was homogeneous in this regard).
The age of BCT patients ranged from 28 to 80 years. The mean age in this group was M = 59.7 (SD = 10.9). Mastectomy patients were between 34 and 81 years old (M = 59.9; SD = 11.9). An independent sample t-test did not reveal any significant differences between the ages of the different groups [t =0.088; p = 0.930]. The study group was not differentiated by the mean number of children [t =0.00; p =1.00]. BCT patients had from 1 to 5 children (M = 2.1; SD = 0.86), while mastectomy patients had from 0 to 4 children (M = 2.1; SD = 0.81). Most of the women in both groups were married, with 35 married in the BCT group and 27 in the mastectomy group. In addition, in the BCT group there were
3 single women, 5 divorced, and 7 widows. In the group of women who underwent mastectomy, there were 8 divorced women, 1 single, and 14 widows.
Methods
- The mini-Mental Adjustment to Cancer (mini-MAC) scale, designed by Watson, Law, dos Santos, Greer, Baruch and Blis (1988, 1989; after [35]), in its Polish adaptation [35], was used. The scale consists of 29 statements to which the participant responds on a four point scale from definitely yes to definitely no. The scale measures four strategies for coping with a disease and its consequences: anxious preoccupation, fighting spirit, helplessness–hopelessness, and positive reevaluation. Positive reevaluation and fighting spirit constitute the constructive disease coping style, while helplessness– hopelessness and anxious preoccupation constitute the destructive style of coping with cancer. The Cronbach alpha coefficient for the Polish version of the mini- MAC scale is 0.92 for helplessness–hopelessness, 0.90 for fighting spirit, 0.89 for anxious preoccupation, and 0.87 for positive reevaluation. In the studied population, the Cronbach alpha coefficient is 0.85 for helplessness– hopelessness, 0.69 for fighting spirit, 0.87 for anxious preoccupation, and 0.50 for positive reevaluation.
- The Multidimensional Body Self-Regulation Questionnaire (MBSRQ), designed by Cash TH [36], in its Polish adaptation [37], was used. It consists of 69 statements to which the participant responds on a five- point scale from completely agree to completely disagree. The aim of this tool is to investigate the body image of the respondent. The questionnaire consists of seven sub-scales, but only one—appearance assessment—was included in our study, as only this scale examines sense of physical attractiveness, which was the main object of interest in this research project. High results on this scale indicate that one has a positive image of one’s body and high satisfaction with its appearance [36]. Reliability in the study population was measured using the Alpha Cronbach Index and was 0.90 for MBSRQ Appearance Evaluation and 0.72 for MBSRQ Appearance Orientation.
- We also used a personal survey containing questions about sociodemographic data: age, number of children, marital status, education, professional status, financial situation, and place of residence.
In addition, it included questions about the disease, such as: date of diagnosis, course of treatment, experienced support, comorbidities, and cases of cancer in the patient’s family.
Results
In order to verify the hypothesis concerning the influence of breast surgery on the body image of women with cancer, a two-factor analysis of variance was conducted, taking into consideration the following factors: measurement time (one week before the procedure, three months after the procedure, one year after the procedure) and the type of procedure (BCT or mastectomy). The dependent variable was how respondents assessed their body image. The main effect of the measurement time turned out to be statistically significant [
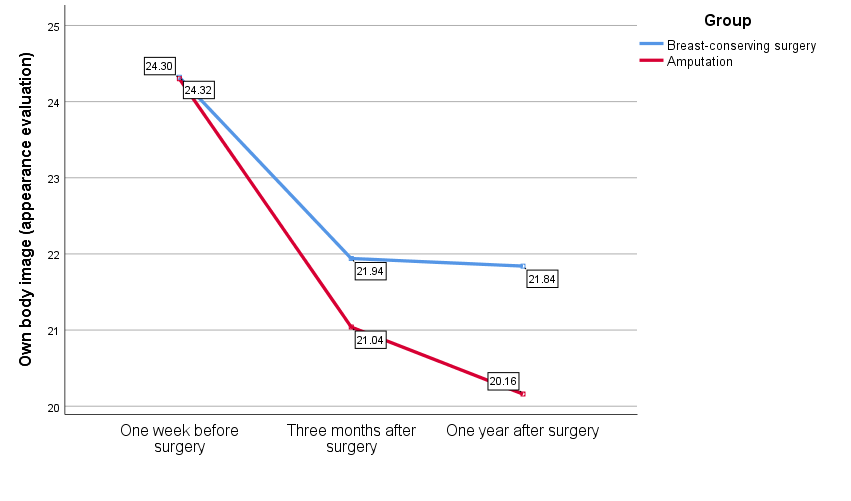
39.94; 0.001 F p = < ; 2 0.45 p η = ]. The analysis did not reveal any significant differences in the assessment of their body between women undergoing BCT and women undergoing mastectomy[ 0.561; 0.456] F p = = . The interaction effect also turned out to be insignificant [ 2.35; 0.101 F p = = ]. Contrast analysis showed that the women with breast cancer evaluated their own appearance worse three months after the surgery [ 58.63; 0.001 F p = < ; 2 0.37] η = and one year after the surgery [ 73.82; 0.001 F p = < ; 2 0.43 η = ] than before the procedure. No difference was found between the measurements taken three months after surgery and one year after surgery in the evaluation of the body image in women with breast cancer [ 2.48; 0.118] F p = = . Additionally, the analysis of simple effects turned out to be statistically insignificant, indicating that women who underwent BCT did not differ from women who underwent mastectomy in terms of the assessment of their own appearance in any of the three measurements. Detailed statistics performed with the use of trend analysis showed a significant linear trend in patients undergoing mastectomy[ ] 13.79; 0.001 F p = < , which indicates a decrease in satisfaction with body image in measurements after the surgery. In women who underwent BCT, the trend analysis turned out to be statistically insignificant [ 3.47; 0.065] F p = = . The following figure presents the mean body image in the study groups one week before the procedure, three months after the procedure, and one year after the surgery.
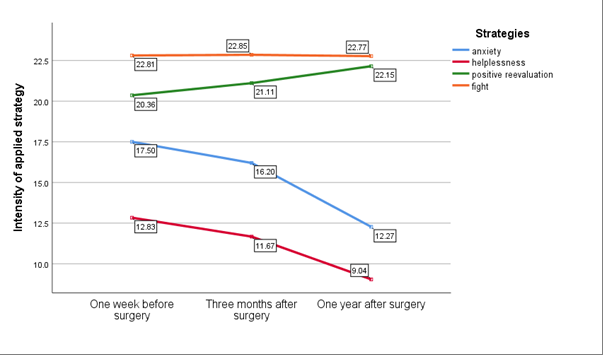
Another hypothesis we investigated assumed that breast cancer patients adopt different coping strategies depending on the stage of the disease. In order to verify this, a two- factor analysis of variance was performed. The factors were the strategies for coping with cancer (anxious preoccupation, helplessness–hopelessness, positive revaluation, fighting spirit) and the time of measurement (one week before the procedure, three months after the procedure, and one year after the procedure). The results showed that the respondents used strategies for coping with cancer with different frequencies ( ) 2 [ 3;97 291.86; 0.001; 0.90] F p η = < = . Analysis of the simple effects shows that the patients used four of the analysed strategies to a different extent before the surgery ( ) 2 [ 3;97 121.513; 0.001; 0.79] F p η = < = , three months after the surgery [ ( ) 2 3;97 174.52; 0.001 ; 0.84 F p η = < = ], and one year after the surgery [ ( ) 2 3;97 505.97; 0.001; 0.94 F p η = < = ]. The significant effect of the measurement time factor ( ) 2 2;98 40.09; 0.001; 0.45 F p η = < = indicates that at different stages of the fight with cancer, the examined patients used different strategies for coping with the disease. Trend analysis showed a linear decrease in the intensity of anxious preoccupation [ 69.93; 0.001] F p = < and helplessness–hopelessness[ 51.01; 0.001] F p = < strategies and an increase in the intensity of the positive revaluation strategy [ 15.37; 0.001] F p = < alongside exacerbation of the disease. No significant change over time in the intensity of the fighting spirit strategy was found. The interaction effect between factors time and strategies for coping with the disease proved to be statistically significant ( ) 2 [ 6;94 20.78; 0.001; 0.57] F p η = < = , which indicates that at different stages of coping with cancer the patients used different strategies—specifically, the intensity of destructive strategies (anxious preoccupation and helplessness– hopelessness) decreases and the intensity of the constructive strategy of positive revaluation increases.
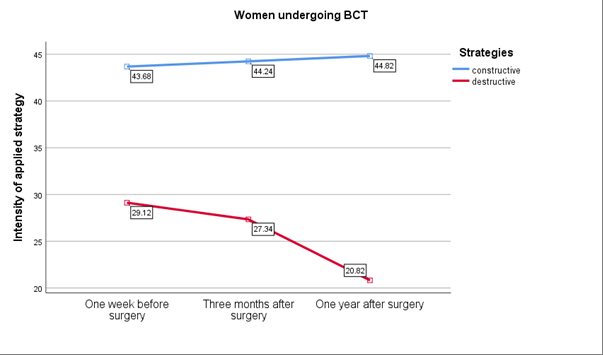
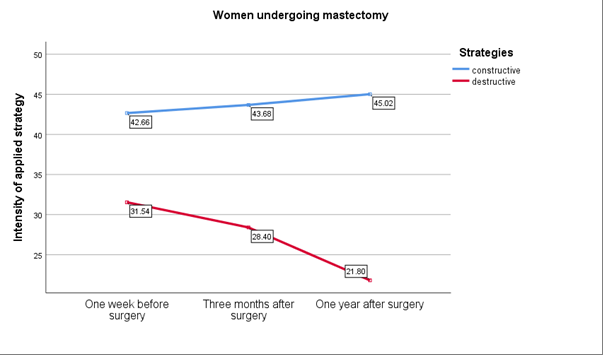
A multivariable variance analysis model was performed in order to verify the hypothesis that patients who underwent breast amputation and BCT patients will use more constructive than destructive strategies for coping with cancer. The intra-objective factors were measurement time (one week before the procedure, 3 months after the procedure, one year after the procedure) and disease coping strategies which, in order to simplify the model and obtain clearer results, were divided into constructive and destructive. The inter-objective factor was the type of surgical procedure performed. The results of the statistical analysis indicated that the respondents used constructive coping strategies significantly more often [ 389.35; 0,001 F p = < ; 2 0.80 η = ] than destructive strategies. The effect of the measurement time factor [ 39.70; 0.001 F p = < ; 2 0.45 η = ] was also statistically significant, which indicates that the intensity of the strategies used to deal with cancer changed over time. The insignificant effect of the group factor indicates that BCT and mastectomy patients did not differ in terms of their coping strategies at different stages of the disease [ 0.53; 0.468 F p = = ]. The statistical analysis showed an insignificant interaction between the type of treatment and the disease coping strategies [ 1.20; 0.275 F p = = ] and between the time of measurement and the type of treatment applied [ 0.30; 0.745]. F p = = The interaction between the disease coping strategies used by the women and the measurement time turned out to be statistically significant [
51.99; 0.001 F p = < ; 2 0.517 η = ]. Detailed statistical results based on trend analysis showed that women who underwent BCT used fewer destructive strategies for coping with the disease as time went on [ 29.43; 0.001 F p = < ]. In the group of mastectomy patients, the intensity of constructive disease coping strategies increased significantly with each subsequent measurement [ 4.98; 0.027 F p = < ], while the intensity of destructive strategies decreased significantly [
43.19; 0.001 F p = < ]. The figures below present the mean levels of constructive and destructive strategies for coping with cancer in BCT and mastectomy patients at the three time points.
Discussion of Results
The empirical evidence gathered during this study confirmed that the body image of women undergoing breast surgery changes. A significant decrease in satisfaction with body image was observed three months after the surgery, but between the third month and a year after the surgery, subjective assessment of appearance did not change. Grogan and Mechan [38] found that in breast cancer patients, the aesthetic aspect is initially less important than the emotional experience of the course of the disease. According to Brandt-Salmeri and Basist [39], patients’ perceptions of post-surgical changes are dynamic—initially, the changes seem to be less important, but with time the effects of treatments become more acute. There appear feelings of shame, a sense of discrepancy between one’s own body and cultural beauty ideals, reluctance to look in the mirror, self-depreciation, and rejection of one’s entire corporeality [16]. Over time, this may lead to an additional decrease in the sense of attractiveness, and consequently to a negative body image [40]. Another difficult element that appears over time is the sense of the lack of control over changes to one’s body due to treatment and surgical procedures. This can cause a significant loss of confidence in one’s image, and struggling with the disease turns into struggling with one’s own body [18]. Long-term studies show that after six months of surgical procedures, patients’ satisfaction with their own bodies decreases and the emotion of shame intensifies. This is because at the time of diagnosis, appearance is not the most important aspect of the disease, and bodily changes become psychologically significant only with time; this can last for quite a while [41, 42]. In addition, our own research has shown that patients undergoing a breast-saving procedure and mastectomy do not differ in terms of body image at any of the stages of treatment. Research by Jabłoński et al., [43] has shown that there is a similar risk of a decrease in level of body acceptance and worsening of sexual relationships in women with breast cancer, regardless of the type of surgery. Breast cancer patients are generally characterized by low acceptance of their own body and critical assessment of their appearance and figure. They also experience difficulties with everyday life caused by their body [43, 44]. Changes in body image are important for women regardless of the surgery, because the very fact of experiencing medical procedures that violate one’s body damages one’s self-image and evokes anxiety-depressive syndromes [39, 45, 46, 47, 48]. Patients who experience greater distress and present lower self-esteem after surgery [22, 49, 50]. The results found in this study differ from some of these presented in the literature on the subject. Some results suggested that differences in body image in women depend on the type of surgery undergone. Some studies suggest a more positive body image in BCT patients compared to these after the mastectomy procedure [29, 50]. BCT patients declare higher satisfaction with their physical appearance and sexual life than women who have undergone breast amputation surgery. The more extensive and advanced the treatment, the worse the women’s evaluation [51]. The lack of differences between the study groups in our research may be explained by the fact that the disease is treated by the patients mainly as a traumatic life-threatening situation [52]. Such an approach may cause difficulties in the integration of sensations and regulation of bodily experience. This is connected with other unpleasant bodily sensations, reduction or increase in the intensity of sensory stimuli, or the inability to integrate the experience of emotions with the experience of bodily sensations [53]. The disease is then treated as an existential problem, rather than an aesthetic one, and it seems that women with breast cancer at first focus more on the question of threat to life than on their own body [23, 50]. Our results show that breast cancer patients use different coping strategies at different stages of the disease, which is in-line with our hypothesis. The helplessness-hopelessness and anxious preoccupation strategies weakened with time. The positive revaluation strategy became stronger, and the only strategy that remained at the same level throughout the three stages was fighting spirit. It has been suggested in the literature that important factors in the acceptance of breast cancer is the time elapsed since the diagnosis and duration of the treatment process. The longer this period, the greater the chance of more complete acceptance of cancer-related difficulties. Studies have shown that almost no patients accept their disease at the time of diagnosis. However, after half a year, some partially accept their condition. Complete acceptance is observed from two to five years after the diagnosis [54]. Our own research has revealed that the levels of anxious preoccupation and helplessness–hopelessness vary during the course of the disease. The moment of diagnosis and process of preparing for surgery may induce a lot of anxiety and cause depressive disorders [55, 56, 57]. High levels of anxiety may have a destructive impact on the patients and lead to difficulties with the development of solutions. Depending on the stage of the disease, the state of dejectedness may be characterized by loss of purpose and sense of meaning, helplessness and hopelessness, inability to cope with the feeling of sadness, resignation, sense of abandonment, incompetence, or self-depreciation [58, 59]. Studies have shown that the most common causes of depression in women with cancer are: sense of threat to one’s life, uncertainty about the near future, loss of control over one’s own life, and insufficient information about the disease and treatment [60, 61].
The obtained results confirmed the hypotheses that both the patients who underwent breast amputation and BCT will apply more constructive disease coping strategies than destructive ones. The literature includes results which confirm that women with breast cancer use constructive disease coping strategies more often [35]. Patients who prefer constructive coping strategies report higher quality of life, fewer nervous breakdowns, better prognosis for recovery, more effective stress management, and better cooperation with medical personnel than patients with destructive coping strategies. Research has shown that the intensity of difficult emotions changes throughout the course of the disease and treatment. This can be due to the disease adaptation process. Depending on the stage of the disease and assessment of the situation, it can be characterized by more or less intense coping strategies. In the first stage of the disease, during diagnosis and the pre- treatment period, the patient experiences higher levels of anxiety, depression, restlessness, tension, and helplessness. However, in the second stage, after the treatment, the patient may undertake more activities that express belief in their ability to fight cancer. Moreover, express more optimism about recovery and returning to everyday life. This, in turn, brings greater disease acceptance and cooperation in the treatment process [62]. Patients activate strong defensive mechanisms and constructive coping strategies to reduce negative emotions and create a sense of ease before and right after surgical interventions [27]. Seeing positive changes in emotions and ways of thinking is a significant stage of adapting to the disease. Hope and willingness to regain health are evoked, accompanied by putting things in perspective and encouraging friends and family to provide support [62]. Some cancer patients may continue the revaluation of their life and try to function in a more satisfying and healthy way once the disease is in remission [7]. Cross-sectional research reveals that, in the long run, after medical procedures, patients experience post-traumatic development and, thus, a better perception of their life situation. The constructive coping strategies are sustained throughout the rest of their life [63].
One of the limitation of the presented study is wide age range of the participants. The aspects studied are complex variables that may be influenced by additional factors like age span. It may affect the perception of the current life situation, coping with stress, as well as self-image in relation to breast cancer, however, the author has so far found no article that confirms the above relationship in cancer. The longitudinal nature of the study provides an opportunity to see what the level of the variables studied was in all patients regardless of age before and after medical procedures [64].
These studies depict only part of reality of breast cancer patients, so it is worthwhile to continue research projects on this subject, touching and expanding upon further psychological aspects unique to women with breast cancer. Broadening our knowledge about important aspects of cancer such as disease coping strategies and body image in women with breast cancer leads to a more complete understanding of the processes that take place during different stages of the disease. This creates the opportunity to develop psychological and psychotherapeutic interventions which are better adjusted to individual needs. Depending on the stage of the disease, patients may need therapeutic help from a team consisting of many specialists, including psychologists, physicians, nurses, and physiotherapists.
References
-
Kori S (2018) An Overview: Several Causes of Breast Cancer. Epidemol Int J 2(1): 000107.
-
Dorfmüller M, Dietzfelbinger H (2011) Psychoonkologie: Diagnostik – Methoden – Therapieverfahren. Edra Urban & Partner.
-
de Walden-Gałuszko K (2011) Psychoonkologia w praktyce klinicznej. PZWL Wydawnictwo Lekarskie.
-
Kissane D, White K, Cooper K, Vitetta L (2004) Psychosocial impact in the areas of body image and sexuality for women with breast cancer. The National Breast Cancer Centre, Camperdown NSW.
-
Conley CC, Bishop BT, Andersen BL (2016) Emotions and Emotion Regulation in Breast Cancer Survivorship. Healthcare 4(3): 56.
-
Hopwood P, Tarry J, Jones B, Maguire P (1993) The assessment of body image in women treated for cancer of the breast. The Breast 2(3): 196-197.
-
Grodecka-Gazdecka S, Zaborek P, Didkowska J, Walden Galuszko K De, Handschuh P, et al. (2014) System-related delays in diagnosis and treatment of breast cancer in Poland. Nowotwory 64(6): 483-490.
-
Bates G, Taub RN, West H (2016) Intimacy, body image, and cancer. JAMA Oncology 2(12): 1667.
-
Kozaka J (2015) The clinical course of cancer and mental adjustment. Current Gynecologic Oncology, 13(1): 27- 43.
-
Lashbrook MP, Valery PC, Knott V, Kirshbaum MN, Bernardes CM (2018) Coping Strategies Used by Breast, Prostate, and Colorectal Cancer Survivors: A Literature Review. Cancer Nursing 41(5): E23-E39.
-
Hamama-Raz Y, Pat-Horenczyk R, Roziner I, Perry S, Stemmer SM (2019) Can posttraumatic growth after breast cancer promote positive coping?—A cross-lagged study. Psycho-Oncology 28(4): 767-774.
-
Paek MS, Ip EH, Levine B, Avis NE (2016) Longitudinal Reciprocal Relationships Between Quality of Life and Coping Strategies Among Women with Breast Cancer. Annals of Behavioral Medicine 50(5): 775-783.
-
Basińska MA, Sołtys M (2020) Personal resources and flexibility in coping with stress depending on perceived stress in a group of cancer patients. Health Psychology Report 8(2): 107-119.
-
Rogala D, Sobieralska-Michalak K, Deja E (2016) Choroby cywilizacyjne i społeczne XXI w.-przegląd i badania. Maciąg M, Nowak BA (Eds.). Wydawnictwo Naukowe Tygiel.
-
Unger C, Weis J (2008) Onkologie. Arends J, Iwona Z (Eds.) 1st (Edn.). MedPharm Polska.
-
Thomas C, Thomas P (2002) Body Image: A Handbook of Theory, Research, and Clinical Practice. American Journal of Clinical Hypnosis. Guilford Press.
-
Izydorczyk B, Kwapniewska A, Lizińczyk S, Sitnik- Warchulska K (2019) Characteristics of psychological resilience and body image in women in the early and late periods after mastectomy. Health Psychology Report 7(1): 32-47.
-
Tomasiewicz A (2015) Body image and self-esteem of patients with onco-hematological diseases after chemotherapy. Psychoterapia 172(1): 73-84.
-
Derbis R, Machnik-Czerwik A (2016) Adaptation of the Body Image after Breast Cancer Questionnaire in the Polish context: Factorial structure and validity of the scale. Health Psychology Report 2(2): 170-187.
-
Lipowska M, Lipowski M (2013) Polish normalization of the Body Esteem Scale. Health Psychology Report 1(1): 72-81.
-
Orzoł A, Orzoł J (2017) Body and cancer. Pielegniarstwo w Opiece Długoterminowej 1(6): 53–56.
-
Brandt-Salmeri A, Przybyla-Basista H (2019) Depression and marital satisfaction: The mediating role of sexual satisfaction and perceived partner acceptance in women after mastectomy. Health Psychology Report 7(2): 121- 132.
-
Mazurek E (2012) The self-image of women after breast reconstruction. Nowiny Lekarskie 81(3): 281-287.
-
Słowik AJ, Jabłoński MJ, Michałowska-Kaczmarczyk AM, Jach R (2017) Evaluation of quality of life in women with breast cancer, with particular emphasis on sexual satisfaction, future perspectives and body image, depending on the method of surgery. Psychiatria Polska 51(5): 871-888.
-
Bai L, Arver B, Johansson H, Sandelin K, Wickman M, et al. (2019) Body image problems in women with and without breast cancer 6-20 years after bilateral risk- reducing surgery - A prospective follow-up study. Breas 44: 120-127.
-
Izdebski P (2007) Psychologiczne aspekty przebiegu choroby nowotworowej piersi. Wydawnictwo Uniwersytetu Kazimierza Wielkiego.
-
Malicka I, Szczepańska J, Anioł K, Rymaszewska J, Woźniewski M (2009a) The evaluation of mood and identification of the patterns of dealing with a disease in women surgically treated for breast cancer or tumour of female reproductive organ. Contemporary Oncology/ Współczesna Onkologia 13(1): 41-46.
-
Marsh S, Borges VF, Coons HL, Afghahi A (2020) Sexual health after a breast cancer diagnosis in young women: Clinical implications for patients and providers. Breast Cancer Research and Treatment 184(3): 655-663.
-
Mazurek E (2014) Amazonian dilemmas. Reasons for women’s refusal to undergo breast reconstructive surgery after surgical treatment of breast cancer. Psychoonkologia 18(3): 97-105.
-
Malicka I, Szczepańska J, Anioł K, Rymaszewska J, Woźniewski M (2009a) The evaluation of mood and identification of the patterns of dealing with a disease in women surgically treated for breast cancer or tumour of female reproductive organ. Contemporary Oncology/ Współczesna Onkologia 13(1): 41-46.
-
Frączek M (2003) Chirurgia nowotworów. Alfa Medica Press.
-
Rutkowski P, Jezierski A, Wysocki WM (2019) Chirurgia onkologiczna. PZWL.
-
Wysocki PJ, Krzakowski M (2013) Systemic treatment for early breast cancer based on St. Gallen Guidelines 2013. Oncology in Clinical Practice 9(5): 167-171.
-
Miller KD, Siegel RL, Lin CC, Mariotto AB, Kramer JL, et al. (2016) Cancer treatment and survivorship statistics, 2016. CA: A Cancer Journal for Clinicians 66(4): 271-289.
-
Juczyński Z (2001) Measurement tools in health promotion and psychology. Pracownia Testów Psychologicznych PTP, pp: 112-122.
-
Cash TF (2017) Multidimensional Body–Self Relations Questionnaire (MBSRQ). In: Encyclopedia of Feeding and Eating Disorders. Springer Singapore, pp: 551-555.
-
Brytek-Matera A, Rogoza R (2015) Validation of the Polish version of the Multidimensional Body-Self Relations Questionnaire among women. Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity 20(1): 109-117.
-
Grogan S, Mechan J (2016) Body image after mastectomy: A thematic analysis of younger women’s written accounts. Journal of Health Psychology 22(11): 1480- 1490.
-
Brandt-salmeri A, Przybyła-basista H (2018) Body image and self-esteem in women with breast cancer – the role of body acceptance. Psychoonkologia 22(1): 1-10.
-
Rezaei M, Elyasi F, Janbabai G, Moosazadeh M, Hamzehgardeshi Z (2016) Factors influencing body image in women with breast cancer: A comprehensive literature review. Iranian Red Crescent Medical Journal 18(10): e39465.
-
Moreira H, Canavarro MC (2010) A longitudinal study about the body image and psychosocial adjustment of breast cancer patients during the course of the disease. Eur J Oncol Nurs 14(4): 263-270.
-
Prates ACL, Freitas-Junior R, Prates MFO, Veloso M de F, Barros N de M (2017) Influence of Body Image in Women Undergoing Treatment for Breast Cancer. Revista Brasileira de Ginecologia e Obstetricia : Revista Da Federacao Brasileira Das Sociedades de Ginecologia e Obstetricia 39(4): 175-183.
-
Jabłoński MJ, Kozaka J, Rachel W (2015) The questions about the differences of psychotherapy and supervision in psycho-oncology. Psychoonkologia 19(3): 97-103.
-
Goula I, Alikari V, Charalampous G, Tzavella F, Zyga S, et al. (2020) Social support and quality of life in Greek women with breast cancer during chemotherapy and two years later. Health Psychology Report 8(2): 97-106.
-
Bahrami M, Mohamadirizi M, Mohamadirizi S, Hosseini S (2017) Evaluation of body image in cancer patients and its association with clinical variables. Journal of Education and Health Promotion 6(1): 81.
-
Den Oudsten B, Steeg A, Roukema J, De Vries J (2012) Changes in Body Image in Women with Early Stage Breast Cancer. In: Ravinder M (Ed.), Topics in Cancer Survivorship.
-
Fang SY, Shu BC, Chang YJ (2013) The effect of breast reconstruction surgery on body image among women after mastectomy: A meta-analysis. Breast Cancer Research and Treatment 137(1): 13-21.
-
Malik AA (2013) Psychological Problems in Breast Cancer Patients: A Review. Chemotherapy: Open Access 2(2).
-
Bagheri M, Mazaheri M (2015) Body Image and Quality of Life in Female Patients with Breast Cancer and Healthy Women. Journal of Midwifery & Reproductive Health 3(1): 285-292.
-
Brandt A, Przybyła-Basista H (2016) Decision on breast reconstruction in women after mastectomy – motivation, concerns, effects’ perception. Psychoonkologia 20(1): 17-26.
-
Białek K, Bolek K, Kowalczyk R, Lew-Starowicz Z (2015) The sexuality and the quality of life of women examined to 18 months and 5 years after the surgery on the mastectomy – comparative analysis. Państwo i Społeczeństwo 15(4): 121-129.
-
John B, Catherine S (2010) Principles of Trauma Therapy: A Guide to Symptoms, Evaluation, and Treatment. Instytut Psychologii Zdrowia.
-
Mirucka B, Sakson-Obada O (2013) Ja cielesne. 1st (Edn.). GWP.
-
Pawlik M, Karczmarek-Borowska B (2013) Acceptance of cancer by women after mastectomy in Western Pomerania region – preliminary studies. Medical Review 2: 203-211.
-
Janiszewska J (2000) Some factors determining level of anxiety at patients with breast lump waiting on surgery. Psychoonkologia 7: 49-54.
-
Łuczyk M, Pietraszek A, Łuczyk R, Stanisławek A, Szadowska-Szlachetka Z, et al. (2015) Incidence and intensification of anxiety and depressive disorders at women with breast cancer prepared for the surgical treatment. Journal of Education, Health and Sport 5(5): 52-66.
-
Ho SS, So WK, Leung DY, Lai ET, Chan CW (2013) Anxiety, depression and quality of life in Chinese women with breast cancer during and after treatment: a comparative evaluation. Eur J Oncol Nurs 17(6): 877-882.
-
Kieszkowska-Grudny A (2012) Distress and depression in cancer patients – diagnosis and treatment. OncoReview 2(4): 246-252.
-
Mausbach BT, Yeung P, Bos T, Irwin SA (2018) Health care costs of depression in patients diagnosed with cancer. Psychooncology 27(7): 1735-1741.
-
Car J, Zycińska J, Lasota W (2012) Assessment of psychological distress and depression in cancer patients. Przeglad Epidemiologiczny 66(4): 689-695.
-
Naik H, Leung B, Laskin J, McDonald M, Srikanthan A, et al. (2020) Emotional distress and psychosocial needs in patients with breast cancer in British Columbia: younger versus older adults. Breast Cancer Res Treat 179(2): 471-477.
-
Dryhinicz M, Rzepa T (2018) The Level of Anxiety, Acceptance of Disease and Strategy of Coping with Stress in Patients Oncological and Non-oncological. Annales Universitatis Mariae Curie-Skłodowska, Sectio J, Paedagogia-Psychologia 31(1): 7-21.
-
Lelorain S, Bonnaud-Antignac A, Florin A (2010) Long Term Posttraumatic Growth After Breast Cancer: Prevalence, Predictors and Relationships with Psychological Health. Journal of Clinical Psychology in Medical Settings 17(1): 14-22.
-
Terelak JF, Krzesicka E, Małkiewicz M (2009) The locus of control and sense of coherence and coping stress strategies at women of cancer patients of breast. Studia Psychologica: Theoria et Praxis 9: 21-44.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis