Randomized Controlled Trial of Acceptance and Commitment Therapy for Posttraumatic Stress Disorder Symptoms in Afghan Adolescent Girls
This study is a randomized controlled trial to investigate the effectiveness of acceptance and commitment therapy (ACT) on posttraumatic stress (PTSD) symptoms in adolescent girls in the aftermath of suicide attacks in Afghanistan. The participants (n = 43) were students at a private school in Kabul. The Children’s Revised Impact of Event Scale (CRIES-13) was completed by all participants after meeting the inclusion criteria. Participants were randomly assigned to experimental and control (waiting list) groups. There were 20 participants in the experimental group and 23 participants in the waiting list group. The experimental group received three ACT sessions a week for eight total intervention sessions. Four weeks after baseline, the ACT and control groups completed the CRIES-13 again. Multivariate analysis of covariance showed a significant difference between the ACT group and the waitlist control group in CRIES-13 total scores and subscales of arousal, intrusion, and avoidance at the post-test phase. We conclude that ACT resulted in an effective reduction in PTSD symptoms for adolescent Afghan girls. This success suggests that the intervention could be used in other treatment centers to reduce the symptoms of PTSD.
Introduction
Although the mental health of children and adolescents has received much attention from international public health programs [1], continued global conflict and traumatic events have especially extreme effects on children and adolescents. Violent conflicts result in famine and homelessness of minors, as well as in long-term economic impact [2]. In some studies, more than two-thirds of children and adolescents in the United States reported experiencing trauma at least once before the age of 16, with 13.4% developing posttraumatic stress symptoms (PTSS) [3]. A meta-analysis of 72 articles found that 15.9%
of trauma-exposed children and adolescents developed PTSD [4]. Rates of trauma are extremely high for children in Afghanistan. In studies of adolescents after terror attacks in Kabul, it has been observed that the rate of posttraumatic stress disorder (PTSD) was 52.5% [5] to 64.2% [6]. In a study conducted on 1,011 adolescents in several provinces of Afghanistan, two-thirds of them reported that they had experienced traumatic events, with PTSS more likely with increased exposure [7].
Given these high rates of trauma exposure and PTSS in children and adolescents, identifying adequate treatment methods is vital. Drug treatments may be effective in some situations; individual and group psychotherapies such as trauma-focused cognitive-behavioral therapy [8] and eye movement desensitization and reprocessing (EMDR) are commonly used non-pharmacological interventions [9]. Techniques such as writing for recovery [10], psychological debriefing [11], written exposure therapy [12], and memory specific therapy (MEST) [11, 8, 13] also have evidence for their effectiveness in some situations. Such treatments have common features as cognitive-focused psychotherapies. Additionally, third-wave behavioral treatments such as acceptance and commitment therapy (ACT) may also show promise in treating PTSS.
ACT is a functional contextual therapy and considers human suffering and problems because of psychological inflexibility [14]. Based on the Relational Frame Theory, ACT focuses on identifying modes of action in line with one’s deeply held values [15]. Research shows that the growth and persistence of PTSS over time is related to experiential avoidance [16]. ACT has been hypothesized to be particularly effective in addressing avoidance in PTSD [17], and preliminary evidence suggests that ACT may be effective in treating PTSD [18], including in work with adolescents [19]. Other evidence shows that ACT has been effective in reducing PTSS in the parents of children with incurable diseases [20], in war veterans [21, 22, 23] and in traumatized adults [24].
This treatment model assumes that the main symptoms of PTSFD, such as experiential avoidance of trauma-related stimuli, result from the constant efforts to escape from the thoughts, emotions, and memories related to the trauma [14]. Thus, the ACT model may posit the avoidance of stimuli that remind the injured person of the traumatic incident to be the cause of the primary symptoms of PTSD. Basic ACT strategies such as mindfulness or commitment help patients to reduce avoidance. Other strategies include teaching patients to focus on the present moment, acceptance of inner experiences, and improvement of psychological flexibility [14, 17].
The ACT approach to reduce PTSS has increased [18], but less research has focused on children and adolescents with PTSD. In cases of PTSD caused by the repercussions of war, no ACT-based intervention work has been published.
This study thus aims to investigate the effectiveness of an ACT group intervention on PTSD in Afghan adolescent girls affected by suicide attacks.
Methods
Design
The present study was conducted as semi-experimental with a pre-test and post-test design with a waitlist control group (WCG). Participants were divided into two groups of active and WCG based on their baseline score on PTSD symptoms on the CRIES-13. These two groups were designed to have approximate equivalence in terms of average baseline scores.
Twenty students in the experimental group received ACT in eight sessions of group intervention in a single group. Sessions were held every other weekday for two weeks, and twice in the third week. All sessions lasted approximately 75 minutes and were led by the first author in Persian. The facilitator received 20 hours of training and was supervised by the second and third authors.
Twenty-three students in the WCG were on the intervention waiting list. All waiting list participants were provided ACT group therapy at the post-test.
At the end of four weeks, both groups were evaluated based on the CRIES-13. All intervention sessions were conducted inside the students’ school.
Participants
Participants in the study included 43 female adolescent students from a private school in western Kabul. The school was near a military building initially destroyed by the Taliban with a car bomb in 2019. A terrible sound and gunshots were heard in the school. The windows of the school were broken, and some students received superficial wounds. The study was conducted three months after the incident.
Participants were students between grades 7–12. Inclusion criteria included PTSD symptoms above 26 on the CRIES-13 and no use of psychoactive medications or drugs. The age range of these students ranged from 12 to 18 years (experimental group M = 14.8 [SD = 1.93]; WCG M = 15.47 [SD = 1.75]). Other demographic information can be found in Table 1.
2356/Measures
CRIES-13 The Children’s Revised Impact of Event Scale (CRIES-13) is a 13-point PTSS self-assessment questionnaire that measures subscales of intrusion, avoidance, and arousal over the last seven days [25]. This measure is designed for children and adolescents over 8 years of age and has high validity [26]. Previous work has used a cut-off point of 26 for the diagnosis of PTSD [8, 27]. Past work has shown a reliability coefficient in Afghan adolescents of 0.82 to 0.91 based on Cronbach’s alpha [8, 28].
Procedure
The proposal was evaluated and approved by the Ethical Committee of the Afghanistan Ministry of Public Health (#0419-0015). Researchers identified areas that had been attacked by suicide bombers in Kabul and identified a school near this attack. From this school, 120 female adolescent students were administered the CRIES-13; 63 were found to have PTSD symptoms over the cutoff. A consent form for participating in the program was sent through the school to participants’ families. Both families and participants provided consent.
Groups were created by partial randomization to ensure similar CRIES-13 scores across both groups. The intervention began in the experimental group after the group assignment. According to the intervention protocol, each week three 75-minute sessions were conducted each day by the first author.
After the final group meeting, the CRIES-13 was readministered to all participants.
Intervention
The researchers designed an acceptance and commitment intervention protocol appropriate for adolescents. Pre-existing resources were used to develop eight sessions [29, 30].
In this protocol, objectives included familiarity with kinds of pains; mindfulness training; acceptance and desire; familiarity with values; and commitment to values. In each session, these elements were presented; participants practiced exercises in the session and then were given homework assignments. At the beginning of each subsequent session, the facilitator reviewed assignments and a summary of the previous meetings.
The intervention program was implemented by the first author as described above.
Statistical Analysis Plan
Given the pretest-posttest design with two groups, a multivariate analysis of covariance (MANCOVA) was used to determine differences between experimental and control groups. Data were analyzed using SPSS 27 software.
Results
As shown in Table 1, after eight sessions of intervention, the mean post-test scores of PTSDS were 20.9 (SD = 11.76) in the experimental group and 38.17 (7.36) in the control group. Therefore, there was an 18.3 difference in mean scores between the baseline and the posttest in the total score.
| ACT | Control | |
|---|---|---|
| Demographics | ||
| Age (years) | 14.80 (1.93) | 15.47 (1.75) |
| Baseline | ||
| PTSD (Total Score) | 37.80 (9.30) | 39.20 (9.8) |
| Intrusion | 9.70 (4.85) | 10.60 (4.18) |
| Avoidance | 13.20 (4.57) | 13.50 (5.59) |
| Arousal | 14.90 (4.83) | 15.17 (4.50) |
| Post-Intervention | ||
| PTSD (Total Score) | 20.90(11.76) | 38.17 (7.36) |
| Intrusion | 5.60 (5.07) | 11.60 (3.83) |
| Avoidance | 7.20 (5.48) | 13.08 (5.99) |
| Arousal | 8.10 (5.48) | 13.47 (5.99) |
Table 1: A MANCOVA showed (Table 2) a significant difference between ACT and control on the combined symptoms of PTSD scores, int
Note: PTSD = posttraumatic stress disorder. ACT= acceptance and commitment therapy. Intrusion, avoidance, and arousal are subscales on the CRIES-13. Table 1: Group Characteristics.
The results of covariance analysis of groups in dependent variable of total PTSD score after control of pretest interventionist variable were presented in posttest stage in Table 2.
A MANCOVA showed (Table 2) a significant difference between ACT and control on the combined symptoms of PTSD scores, intrusion, avoidance, and arousal. These results indicate that the ACT intervention showed a greater reduction in total PTSS, intrusion, avoidance and arousal scores compared to the WCG.
- Dependent Variables
- Source df
- F
- Sig.
- Eta Squared
- Observed Power
- Baseline
- 1
- 31.8
- 0
- 0.44
- 1
- Groups
- 1
- 27.7
- 0
- 0.41
- 1
- Intrusion
- Error
- 40
- Baseline
- 1
- 21.2
- 0
- 0.27
- 0.99
- Groups
- 1
- 14.7
- 0
- 0.27
- 0.96
- Avoidance
- Error
- 40
- Baseline
- 1
- 21.8
- 0
- 0.35
- .0.99
- Groups
- 1
- 19.4
- 0
- 0.33
- 0.99
- Arousal
- Error
- 40
- Baseline
- 1
- 13.7
- 0
- 0.26
- 0.95
- Groups
- 1
- 40.1
- 0
- 0.5
- 1
- Total Score of PTSD
- Error
- 40
Table 2: Results of MANCOVA.
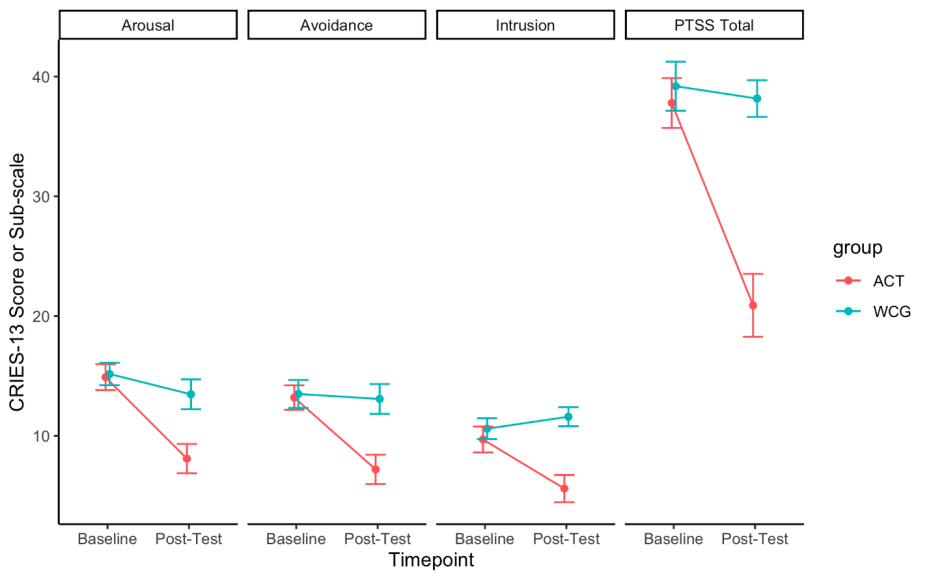
Figure1: PTSS Comparison of Groups Across Timepoints.
Discussion
The aim of this study was to investigate the effectiveness of acceptance and commitment therapy on symptoms of posttraumatic stress disorder in Afghan female adolescents in the aftermath of suicide attacks in Afghanistan. First, we found at the post-intervention assessment that the ACT group had significantly lower PTSD symptom severity than the control group. Second, when considering PTSD symptom clusters at post-intervention, the ACT group and Control group differed significantly on intrusion, arousal, and avoidance symptoms. Also, both adolescent participants and facilitator indicated that ACT would be a useful intervention for reducing PTSS.
This finding is promising. ACT appears to be an acceptable intervention that can reduce PTSD symptoms. Results showed that this intervention was effective in reducing PTSS following a suicide bombing attack. ACT as used in this study challenges the effects of experience avoidance using experimental exercises. It also encouraged the adolescent participants to increase flexibility over their current experiences and to change or adapt their values. Participants learned to focus on the present and to not judge internal and external experiences. They were encouraged to become more aware of themselves and to commit to actions in accordance with their values and goals.
The participants were referring to a common concept in Afghanistan. They used to say that we have a word called the word “fate” (( .ریدقتThat is, disasters may be easier to accept for the Afghan people. Because Afghan people believe in Islamic structure [31] and this word is one of the Islamic concepts. Therefore, ACT’s focus on acceptance and commitment may be particularly acceptable to the people of Afghanistan and to the participants in the current study.
ACT may also be attractive to adolescents, who can become engaged and active in this program. This may be due to ACT’s focus on metaphors and stories. This communication easily discusses concepts in a way that is appropriate for a teenage audience, in line with the results of Twohig [32].
This study was conducted in Afghanistan and focused on war-related trauma. Therefore, it should be approached with caution in generalizing it to situations and other traumas. A limitation also concerns the sample. Although this study was conducted with female adolescents, this method could be used in other age, education, and gender groups and compared with other treatment methods. Future work may demonstrate its efficacy in alternative environments and with other populations.
In general, this study shows ACT to be an effective intervention for adolescent girls affected by traumatic events. ACT may appropriately be used in counseling centers or schools individually or in a group.
References
-
Patel V, Fisher AJ, Hetrick S, McGorry (2007) The mental health of young people: A global public-health challenge. The Lancet 369(9569): 1302-1313.
-
Boyden J, de Berry J (2004) Children and youth on the front line: Ethnography, armed conflict, and displacement Berghahn Books 14: 304.
-
Copeland WE, Keeler G, Angold A, Costello EJ (2007) Traumatic events and posttraumatic stress in childhood. Arch Gen Psychiatry 64: 577-584.
-
Alisic E, Zalta AK, Van Wesel F, Larsen SE, Hafstad GS, et al. (2014) Rates of post-traumatic stress disorder in trauma-exposed children and adolescents: Meta- analysis. Br J Psychiatry 204(5): 335-340.
-
Ahmadi SJ, Jobson L, Earnest A, McAvoy D, Musavi Z, et al. (2022) Prevalence of poor mental health among adolescents in Kabul, Afghanistan, as of November 2021. JAMA Network Open 5(6): e2218981.
-
Ahmadi SJ, Musavi Z, Samim N, Sarwary SAA, Sarwary AA (2022) Prevalence of posttraumatic stress disorder in Abdol Rahim Shaheed School after the explosions [Unpublished manuscript]. Kabul: Behrawan Research and Psychology Services Organization.
-
Panter Brick C, Eggerman M, Gonzalez V, Safdar S (2009) Violence, suffering, and mental health in Afghanistan: A school-based survey. The Lancet 374(9692): 807-816.
-
Ahmadi SJ, Kajbaf MB, Neshat Doost HT, Dalgleish T, Jobson L, et al. (2018) The efficacy of memory specificity training in improving symptoms of post-traumatic stress disorder in bereaved Afghan adolescents. Intervention 16(3): 243-248.
-
Zhang Y, Zhou X, Yang L, Hetrick HE, Weisz JR (2018) Comparative efficacy and acceptability of psychotherapies for post-traumatic stress disorder in children and adolescents: Study protocol for a systematic review and network meta-analysis. Evid Based Ment Health 24(4): 153-160.
-
Kalantari M, Yule W, Dyregrov A, Neshat-Doost H, Ahmadi SJ (2012) Efficacy of writing for recovery on traumatic grief symptoms of Afghani refugee bereaved adolescents: A randomized control trial. Omega (Westport) 65(2): 139-150.
-
Ahmadi SJ, Kajbaf MB, Neshat Doost HT (2012) A comparative study: Efficacy of Trauma-Focused- Cognitive-Behavior Therapy, Psychological Debriefing, Specific Recall Training and Writing for Recovery on symptoms of post-traumatic stress disorder (PTSD) and mood in Afghan adolescents [Unpublished manuscript]. University of Isfahan.
-
Ahmadi SJ, Musavi Z, Samim N, Sadeqi M, Jobson L (2022) Investigating the feasibility, acceptability, and efficacy of using Modified-Written Exposure Therapy in the aftermath of a terrorist attack on symptoms of posttraumatic stress disorder among Afghan adolescent girls. Front Psychiatry 13: 826633.
-
Moradi AR, Moshirpanahi S, Parhon H, Mirzaei J, Dalgleish T, et al. (2014) A pilot randomized controlled trial investigating the efficacy of memory specificity training in improving symptoms of posttraumatic stress disorder. Behav Res Ther 56: 68-74.
-
Hayes SC, Strosahl KD, Wilson KG (2012) Acceptance and Commitment Therapy, Second Edition: The process and practice of mindful change. pp: 402.
-
Hayes SC, Barnes Holmes D, Roche B (2001) Relational frame theory: A post-Skinnerian account of human language and cognition. Adv Child Dev Behav 28: 101- 138.
-
Smith BM, Smith GS, Dymond S (2020) Relapse of anxiety‐related fear and avoidance: Conceptual analysis of treatment with acceptance and commitment therapy. J Exp Anal Behav 113(1): 87-104.
-
Bean RC, Ong CW, Lee J, Twohig MP (2017) Acceptance and Commitment Therapy for PTSD and trauma: An empirical review. The Behavior Therapist 40: 145-150.
-
Wharton E, Edwards KS, Juhasz K, Walser RD (2019) Acceptance-based interventions in the treatment of PTSD: Group and individual pilot data using Acceptance and Commitment Therapy. Journal of Contextual Behavioral Science 14: 55-64.
-
Woidneck MR, Morrison KL, Twohig MP (2013) Acceptance and Commitment Therapy for the treatment of post-traumatic stress (PTSD) among adolescents. Behav Modif 38(4): 451-476.
-
Muscara F, McCarthy MC, Rayner M, Nicholson JM, Dimovski A, et al. (2020) Effect of a videoconference- based online group intervention for traumatic stress in parents of children with life-threatening illness: A randomized clinical trial. JAMA Netw Open 3(7): e208507.
-
Dindo L, Johnson AL, Lang B, Rodrigues M, Martin L, et al. (2020) Development and evaluation of an 1-day Acceptance and Commitment Therapy workshop for veterans with comorbid chronic pain, TBI, and psychological distress: Outcomes from a pilot study. Contemp Clin Trials 90: 105954.
-
Gobin RL, Strauss JL, Golshan S, Allard CB, Bomyea J, et al. (2019) Gender differences in response to Acceptance and Commitment Therapy among Operation Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn veterans. Womens Health Issues 29(3): 267-273.
-
Kelly MM, Reilly ED, Ameral V, Richter S, Fukuda SA (2022) Randomized pilot study of Acceptance and Commitment Therapy to prove social support for Veterans with PTSD. J Clin Med 11(12): 3482.
-
Boals A, Murrell AR (2016) I am > trauma: Experimentally reducing event centrality and PTSD symptoms in a clinical trial. Journal of Loss and Trauma 21(6): 471-483.
-
Children and War Foundation (2005). Children’s revised impact of event scale (CRIES-13).
-
Perrin S, Meiser-Stedman R, Smith P (2005) The Children’s Revised Impact of Event Scale (CRIES): Validity as a screening instrument for PTSD. Behavioural and Cognitive Psychotherapy 33(4): 487-498.
-
Neshat-Doost HT, Dalgleish T, Yule W, Kalantari M, Ahmadi SJ, et al. (2013) Enhancing autobiographical memory specificity through cognitive training: An intervention for depression translated from basic science. Clinical Psychological Science 1(1): 84-92.
-
Ahmadi SJ, Kajbaf MB, Neshat Doost HT (2012) Efficacy of Trauma Focused-Cognitive-Behaviour Therapy on symptoms of post-traumatic stress disorder (PTSD) in displaced war-exposed adolescents in Afghanistan: A comparison study of TF-CBT with psychological debriefing. Interdisciplinary Journal of Contemporary Research in Business 4(5): 1084-1089.
-
Settles R, Morris B, Bratkovich K (2019) Acceptance and Commitment Therapy for PTSD, Veteran manual, mental illness research. Education and Clinical Center (MIRECC).
-
Raja S (2012) Overcoming trauma and PTSD. Oakland: New Harbinger Publications Inc pp: 200.
-
Bragin M, Akesson B, Ahmady M, Akbari S, Ayubi B, et al. (2021) Peace, love, and justice: A participatory phenomenological study of psychosocial well-being in Afghanistan. International Social Work 65(3): 457-479.
-
Twohig MP (2009) Acceptance and Commitment Therapy for treatment-resistant posttraumatic stress disorder: A case study. Cognitive and Behavioral Practice 16(3): 243-252.
- Occupational Stress and Mental Health Outcomes Among Police Officers: A Mini Review
- The Experience of Counterproductive Leadership on Mental Health and Impact on Retention in U.S. Marines: A Phenomenological Study
- Nomophobia in the Digital Age: A Study on College and University Students
- Emotional Regulation in Children with Autism and Learning Disabilities
- Antisemitism on American College Campuses and Its Impact on Jewish Students
- Exploring the Role of Empathy in the Associations of Family Functioning and Purpose in Life with Attitude towards Abortion among Undergraduates: A Moderation Analysis