Influenza-Associated Neurological Complications - Clinical Course and Prognostic Factors
Acute influenza-associated encephalopathy/encephalitis (IAE) in children and adults is not so common but very serious and sometimes fatal neurological complication. The purpose was to show clinical and laboratorial peculiarities in this condition and to indicate some prognostic factors. Materials and methods: In a period of three years (2014-2017) through the Clinic of Infectious diseases at the University Hospital in Stara Zagora, Bulgaria 7 patients with this neuroinfection were passed. They were aged between 3 and 42 years. Clinical, epidemiological, laboratorial and instrumental investigations were accomplished in all patients. The results were processed with statistical program SPSS for Windows, v. 14. Results and discussion: Clinical manifestations appeared in 5 patients with an initial convulsion usually within 24-72 hours after the acute onset of the disease and quantitative changes in consciousness to coma in 3. Clinical manifestations of meningeal irritation were detected in only two patients Laboratory blood tests showed in 3 patients’ elevated levels of leucocytes and amino transferases, high urea, glucose and creatinin. The findings of cerebrospinal fluid in them indicated albumin values from 1,0 to 6,0 g/l and increased glucose from 4,5 to 21 mmol/l. All of these three patients ended up with a fatal outcome. Their pathological outcomes detected necrotizing encephalopathy. The remaining 4 patients were fully recovered except for one in which there is a 7 cranial-brain nerve paresis as a residual symptom. The diagnosis was confirmed by clinical and epidemiological data, but also by serological (ELISA) in blood investigations and virological (PCR) in nasal swabs and also in autopsy material. In all but one influenza A virus was detected. Influenza virus B strain Victoria was detected with him. All patients were treated with Oseltamivir in appropriate doses. None of them were vaccinated against influenza. Conclusion: IAE had a well-known clinical course. Some extremely elevated laboratorial changes as amino transferases, blood sugar and urea may predict a lethal outcome. IAE was a complication which could be avoid by specific vaccine use.
Introduction
Encephalitis / encephalitis caused by Influenza virus is not as common a neurological complication but it is associated with high mortality and subsequent consequences. It is usually defined as a changed mental status lasting more than 24 hours, but its clinical spectrum may range from mild confusion to behavioral changes, delirium / hallucinations, meaningless speech, mutism / aphasia, lethargy, drowsiness and coma [1]. Isolated cases of neuro infections caused by the influenza virus do not allow for more detailed summaries. Recently, reports of influenza-related encephalopathy have grown globally [2]. Influenza virus belongs to a family of Orthomixoviridae. There are four types of influenza viruses: A, B, C and D. Human influenza A and B viruses cause seasonal epidemics of disease almost every winter all over the world [3]. It is considered that CNS is affected more often with serotype A, less with B [4]. The purpose of this investigation is to show clinical and laboratorial peculiarities in Influenza virus neuro infections as well as to indicate some prognostic factors which influenced their outcome.
Materials and Methods
In a period of three epidemic out breaks during 2014- 2017 through the Clinic of Infectious diseases at the University Hospital in Stara Zagora, Bulgaria 7 patients with this neuro infection were passed. They were aged between 3 and 42 years, 5 of them were men, 2 - women. Clinical, epidemiological, laboratorial and instrumental investigations were accomplished in all patients. The diagnosis was established serologically by rises in specific antibody titers in serum or nasal swabs and virologically by rapid diagnostic tests (RT-PCR), demonstration of viral genetic material in clinical specimens, or autopsy tissue section. Viral nucleic acids were extracted automatically from respiratory specimens using aExiPrepDx Viral DNA/RNA kit. Detection and typing/sub typing of Influenza viruses were carried out by a RT-PCR method and the Super Script III Platinum. Primers, probes and positive controls were provided by the International Reagent Resource (IRR), USA. Amplification was performed using a Chromo 4 thermal cycler. Samples with a cycle threshold (ct) value < 38 were considered positive. The results were processed with statistical program SPSS for Windows, v. 14. Ten variables were analyzed to formulate a predictive model for death caused by influenza-associated encephalopathy (IAE). The variables identified as significant at P< 0.05 using univariate logistic regression analysis were entered into a multi variate logistic regression model, and the least significant variables were sequentially removed. In the multi variate logistic regression analysis, the model was adjusted by age, sex, virus type, indeces of haemostatic status, renal and hepatic function, as leucocyte and thrombocyte count, urea, creatinine, fibrinogen, protrombine time, ALAT, ASAT. In the multi variate logistic regression analysis, a value of P< 0.05 was considered statistically significant. A P value between 0.05 and 0.10 was considered to show a tendency toward being a factor for poor prognosis because a risk existed of eliminating important prognostic factors in the logistic regression if the P values were restricted to <0.05. Odds ratios with 95% confidence intervals were also estimated.
Results
An acute, sudden onset with fever, high fatigue, headache and muscle aches was established in all our 7 patients. The temperature varied from 38.1 to 41ºC (mean 39, 40C±1,6). Catarrhal syndrome was demonstrated with coughing, runny nose, and flushed throat. In 3youngest patients there were dyspeptic Pekova L, et al. Influenza-Associated Neurological Complications - Clinical Course and Prognostic Factors. Vaccines Vacccin 2018, 3(2): 000124.
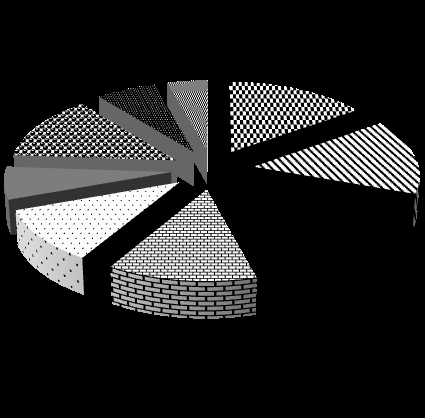
syndrome with vomiting, abdominal pain and diarrhea (Figure 1).
$$ = 1 0 0 $$
T˚C
7 6 5 3 Muscle pain $$ \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \cdot \ $$
= \frac {1}{2} \times 1 0 ^ {4}
$$ Runny nose Vomiting $$
P = \frac {1}{2} \pi r ^ {2}
$$ $$
\mathrm {C O} {2} + \mathrm {H} {2} \mathrm {O} = \mathrm {H C O} {3} + \mathrm {H} {2} \mathrm {O}
$$ Abdominal pain Diarrhoes $$
\mathrm {C O} {2} + \mathrm {H} {2} \mathrm {O} = \mathrm {H C O} {3} + \mathrm {H} {2} \mathrm {O}
$$ Figure 1: Clinical manifestations of Influenza encephalopathy. In 5 of our patients the neurological complications began within the first 24 hours of the disease. In 2 cases CNS involvement was demonstrated within 7-10 days after initiation. Initial seizures were followed with changes in consciousness, paralysis of cerebral and peripheral nerves, disturbed gait (Table 1).
| Enhanced tendon reflexes | 6 |
| Neck stiffness | 2 |
| Kernig | 2 |
| Upper Brudzinski | 1 |
| Convulsion | 4 |
| Disturbed consciousness | 7 |
| Cranial-brainnerves'paralysis (VI, VII) | 2 |
| Peripheralparalysis | 2 |
| Babinski'sreflex | 4 |
| Vertigo | 2 |
| Disturbed gate | 2 |
Table 1: Changes in neurological status. Of particular importance was the premorbid background. Four of our patients had pre-exis
Table 1: Changes in neurological status. Of particular importance was the premorbid background. Four of our patients had pre-existing illnesses – arterial hypertonia, chronic pyelonephritis, Wilson-Konovalov’s disease, chronic obstructive pulmonary disease. Lumbar puncture was performed at all patients in the first hours after admission to the clinic of Infectious diseases, University hospital, Stara Zagora. The CSF profile showed normal protein in 4 and mildly elevated in 3. Pleocytosis consisted of a mono nuclear cells was observed only in 2 adult patients. The level of glucosis was high (8,41, 8,34 and 21,7 mmol/l) in 3. Computerized tomography (except for two patients who had generalized cerebral edema), as well as magnetic resonance imaging, and electro encephalography in all were normal influenza virus A (H1N1) in 3 patients, A (H3N2) also in 3 and B (Victoria) in1 were confirmed. The identification and serological determination of the influenza virus for the Republic of Bulgaria and in particular for the Stara Zagora region is presented in Figure 2.
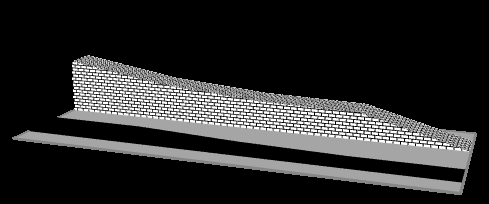
Figure 2: Sero typing of isolated Influenza viruses. In all cases with Influenza neuro infections Oseltamivir as the only one etiological agent was applied immediately after the admission. Antibiotics were applied in 3 patients. Bio products such as fresh frozen plasma were used in all. The outcome of the disease was healing at 3, residual palsy of 7 cranial-brain nerve in 1. In 3 there was a fatal outcome. Three fatal cases where the histological examination of brain tissue preparations from the autopsy material showed necrotizing encephalopathy were presented bellow.
Case 1
GKG, a 3 year old girl from a second pregnancy normally born in the term per viasnaturalis. She was not immunized against Influenza, because she was not frequently ill child. She had been in contact with her sister, who had been feverish and catarrhal for several days. The disease started sharply on January 19th, 2016 with temperature up to 38.5˚C, runny nose, dry cough, multiple vomiting and diarrhea. On the next morning, against a background of a temperature of 39˚C, she made Pekova L, et al. Influenza-Associated Neurological Complications - Clinical Course and Prognostic Factors. Vaccines Vacccin 2018, 3(2): 000124.
a tonic-clonic convulsion with cyanosis. Emergency was called and the child was admitted to the Clinic of Infectious diseases with marked drowsiness, believed to be due to the used Diazepam. A few hours later a change of her consciousness was established – spoor. She had a dysrhythmic breathing, too. The lumbar puncture showed a clear effluent flowing out of the jet. Biochemical studies of CSF had high protein level, in blood there were normal leucocyte count but with demonstrative neutrophilia, elevated sodium levels, as well as amino transferases (both ACAT and ALAT), blood sugar, urea and creatinine. At the end of the day of admission to the hospital her condition was getting worse – coma with 3-5 points on the GCS. Increased spleen and liver had evolved. The patient remained in a severe comatose condition, with paresis of VI cranial-brain nerve. The pupils had a permanent mydriasis, no light reaction. On January 24th the patient made a cardiac arrest, which despite the resuscitation procedures could not be overcome and she died. The histological finding of brain tissues showed focal necrosis, spotting bleeding, blood-filled vessels, scarring lymphocyte infiltrate, extreme swelling (Photo 1)
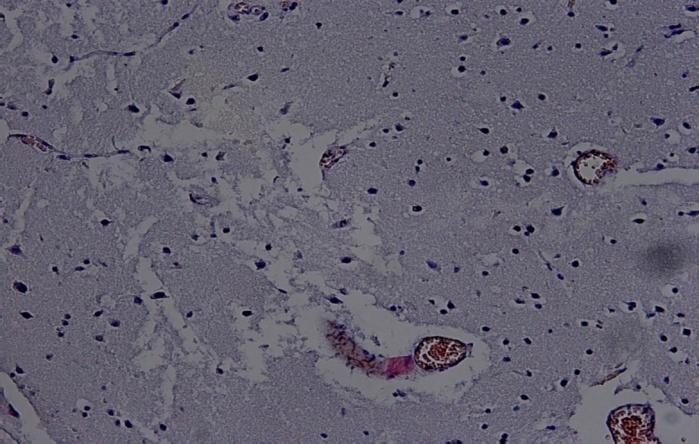
Photo 1: Brain and meninges - focal necroses, spotting bleeding, blood-filled vessels, scarring lymphocyte infiltrate, extreme swelling.
Case 2
IYI, a 42 year old man. He had a bad premorbid background with Wilson-Konovalov’s disease, chronic pyelonephritis and hypertonic disease. The illness began acutely 5 days ago with typical catarrhal manifestations with a fever up to 38, 4°C, runny nose, coughing and increasing fatigue. He had been in contact with his relatives, who were sick with flu. He was admitted at the Clinic of Infectious diseases due to drowsiness, bradypsychia and bradilalia, which occurred a little earlier in the day. He was somnolent, febrile to 41°C. On the second day, patient fell into a coma and was placed on mechanical ventilation, due to disturbed spontaneous breathing. Data of X-ray showed massive bilateral pneumonia. Lumbar puncture showed an inflammation of the meninges. Death occurred as a result of immediate cardiac arrest on the 10th day.
Case 3
IZD, a 36 year old woman who had chronic pyelonepfritis and bronchial asthma. Two days after the sharp onset with catarrhal syndrome and temperature up to 39.8°C, she made a status epilepticus from which it was difficult to get. She was brought to the Clinic of Infectious diseases in somnolent status. Neurological examination was established signs of meningeal irritation, double- sided Babinski, lesion of 7 cranial-brain nerve, and left- sided hemiparesis. Not with standing of immediately taken adequate therapeutic measures, its condition progressively deteriorated. On the next day three consecutive generalized seizures followed, after that the patient had fallen into a coma and was placed on apparatus ventilation because of the respiratory failure. Laboratory tests from the CSF on the admission day showed slight pleocytosis and elevated protein. Biochemical parameters in the blood showed the same trend as in the previous two cases - elevated amino transferases, blood sugar, and nitro genous bodies. In this patient, the lethal outcome occurred on the fifth day.
Discussion
The number of cases of neuro infections caused by Influenza virus for the cited period for Bulgaria as a whole was 81 and in particular for Stara Zagora region they were 21. Of all these 21 registered cases, only 7 met the definition of encephalitis / encephalopathy caused by the Influenza virus: a) Presence of high fever, b) Severe clinical course with neurological manifestations such as paralysis of the cranial-brain and/or peripheral nerves, c) Seizures d) Quantitative disturbances of consciousness to coma e) Relevant Laboratory changes in the CSF [5].
Pekova L, et al. Influenza-Associated Neurological Complications - Clinical Course and Prognostic Factors. Vaccines Vacccin 2018, 3(2): 000124.
Although influenza-associated encephalopathy was observed more frequently in young children with a peak incidence between 6 and 18 months of age [5], our patients were aged from 3 to 42 years. Influenza neuro infections occurred more frequently in males than females and tended to be more severe in them [6]. The cases reported confirm the male gender prevalence, but as far as the fatal outcome is concerned, only 1 of 3 died was a man. Meningeal irritation was not a common occurrence in Influenza-associated Encephalopathy [7]. We observed partial meningeal syndrome in 2 patients. Literally, influenza-associated encephalopathy is more often caused by serotype A than B [6]. In our study only one case of Neuro infection was caused by serotype B. According to Steininger C, et al. Influenzal encephalopathy (i.e., acute encephalopathy occurring in the course of the acute respiratory illness) and post Influenzal encephalopathy (i.e., acute encephalopathy occurring within 3 days to 3 weeks after resolution of the influenza-related respiratory symptoms) [6]. In our patients more often influenza encephalopathy was seen – in 5 patients. The remaining 2 had a post Influenzal one. Influenzal encephalopathy was frequently associated with metabolic disturbances. A severely elevated ALAT and ASAT, thrombocytopenia, and hematuria or proteinuria may be associated with disseminated intravascular coagulopathy, multi pleorgan failure, and hemophago cytosis [6]. We observed a reduced hemoglobin and platelets in all, leucopenia – in 6. Elevated levels of creatinine, urea and ASAT were seen in 3 (Table 2).
| Hb | Leuc. | Plt. | Gluc. | Creat. | Na | ALAT | Fibr. | PT | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient/age | |||||||||||||||||||||||||||||
| g/l | .109/l | .109/l | mmol/l | | mmol/l | U/l | g/l | % | |||||||||||||||||||||
| GKG, 3 | 80 | 2,0 | 16 | 71,6 | 164 | 192 | 1327 | 2,5 | 33 | ||||||||||||||||||||
| IYI, 42 | 80 | 2,0 | 24 | 21,4 | 664 | 183 | 573 | 3,0 | 41,7 | ||||||||||||||||||||
| IZD, 37 | 80 | 1,8 | 38 | 21,2 | 364 | 167 | 389 | 1,5 | 33 | ||||||||||||||||||||
| MAM,9 | 92 | 3,8 | 98 | 7,4 | 122 | 154 | 19 | 3,8 | 54,0 | ||||||||||||||||||||
| KRD, 12 | 90 | 4,0 | 109 | 5,4 | 87 | 149 | 16 | 4,0 | 64,2 | ||||||||||||||||||||
| OKT, 29 | 101 | 3,4 | 123 | 6,2 | 52 | 139 | 22 | 3,8 | 67 | ||||||||||||||||||||
| RID, 41 | 96 | 3,6 | 111 | 4,2 | 119 | 164 | 41 | 4,2 | 76 |
Table 2: Blood laboratory tests. There had been attempts to separate encephalopathy from encephalitis based on the presence of ce
Table 2: Blood laboratory tests. There had been attempts to separate encephalopathy from encephalitis based on the presence of central nervous system (CNS) inflammation. For instance, only a few patients with influenza-associated encephalopathy had elevated protein or mild Pleocytosis in the CSF; in most cases CSF is normal [8]. Influenza encephalitis according to literature data was suspected if the CSF shows pleocytosis [9, 10]. Only two of our patients had a mild to moderate pleocytosis – 160-960.106/l. We observed elevated protein in 3 patients, but they all had a pleocytosis, too (Table 3).
| Leuc. | Eryth. | Alb. | Glucose | K | Na | Chl. | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patients/age | Pandy | ||||||||||||||||||||||||
| .106/l | .106/l | g/l | mmol/l | mmol/l | mmol/l | mmol/l | |||||||||||||||||||
| GKG, 3 | 9 | 80 | + | 6,02 | 21,4 | 2,0 | 183 | 98 | |||||||||||||||||
| IYI, 42 | 960 | 300 | + | 1,06 | 2,8 | 2,0 | 165 | 104 | |||||||||||||||||
| IZD, 37 | 160 | 144 | + | 1,98 | 7,4 | 3,1 | 155 | 110 | |||||||||||||||||
| MAM,9 | 15 | 21 | ± | 0,42 | 3,5 | 3,7 | 128 | 115 | |||||||||||||||||
| KRD, 12 | 32 | 12 | - | 0,18 | 3,0 | 4,0 | 135 | 87 | |||||||||||||||||
| OKT, 29 | 0 | 4 | - | 0,15 | 4,1 | 3,9 | 133 | 121 | |||||||||||||||||
| RID, 41 | 12 | 3 | - | 0,24 | 3,2 | 5,1 | 148 | 111 |
Table 3: Laboratory tests of cerebral-spinal fluid. Moreover, histological abnormalities of the brain were often absent in patien
Pekova L, et al. Influenza-Associated Neurological Complications - Clinical Course and Prognostic Factors. Vaccines Vacccin 2018, 3(2): 000124.
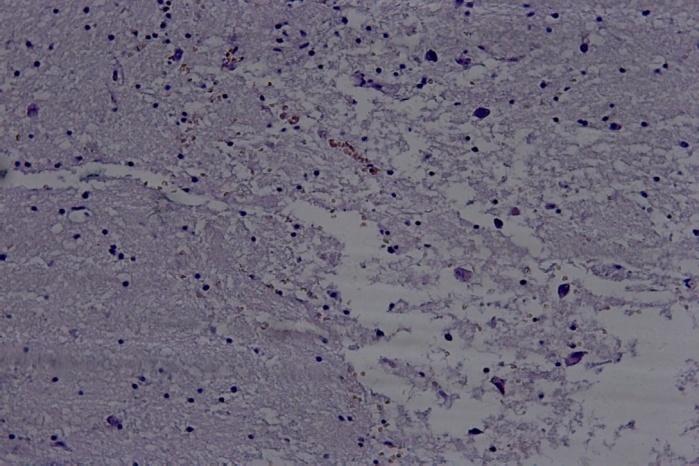
Photo 2: Severe cerebral edema. In clinical practice, rapid diagnostic confirmation of viral neuro infections was advantageous, and avoids sun necessary treatment with antibiotics, reduces the length of hospitalization, and ultimately reduces costs [12]. But we applied antibacterials concomitantly with Oseltamivir in 3 patients, due to the severe course and evidence of concomitant pneumonia. It was well known that influenza virus was associated with various CNS lesions that had poor prognoses, including Reye syndrome, acute necrotizing encephalopathy, and other types of IAE [13]. By literary data approximate lyone third of the children with Influenza encephalopathy died. Death usually occurred within two days of the onset of neurological symptoms and in approximately half was caused by multi‐organ failure [14, 15]. Our study confirmed this - 1/3 children died of multi- organ failure on the 4-th day after admission. Although acute Influenzal encephalitis/encephalopathy was observed more often in child age, mortality was higher in adults [14]. Two of our 4 adult patients died – 1 with brain stem failure and the other with multi-organ failure. The incidence of lethality in influenza encephalopathy without adequate therapy was 30% [5]. A study of Nagao T, et al. showed four prognostic factors for death in the course of influenza-associated encephalopathy by multivariate analysis: elevation of as part at amino transferase, hyperglycemia, the presence of hematuria or proteinuria, and use of diclofenac sodium [2]. In our study uniquivity analysis was applied to 10 variables. Of these, 5 were statistically significant (p <0.05) – ASAT, blood sugar, urea, creatinin and consciousness. They were included in multi variate analysis. Logistic regression was applied to assess the impact of a number of patient deaths. Two significant prognostic predictors were used: blood sugar> = 7 mmol/land urea> = 10 mmol/l.
Conclusion
Influenza neuro infections had a severe course, long hospital stay, and an unfavorable outcome with death in 3 of our patients. The neurological signs of meningradicular irritation were not so pronounced in Influenza neuro infections, we noticed them only in 2. In multi variate analysis two significant prognostic predictors for a bad exit were used: blood sugar> = 7 mmol/land urea> = 10 mmol/l. During influenza out breaks in the community, physicians should consider influenza in the differential diagnosis of patients with seizures and altered mental status, especially if patients developed catharral symptoms shortly before the onset of neurologic manifestations and even if a rapid influenza diagnostic test is negative. Effective measures against influenza A and B diseases included prevention of infection by either vaccination with inactivated or live attenuated vaccines, or administration of antiviral drugs prophylaxy. Regular administration of the specific influenza vaccine can prevent or make the disease with a milder clinical course and can reduce the risk of complications. Therefore, annual influenza vaccination and early recognition of influenza virus infection by rapid and sensitive assays seemed all the more important, especially in patients who had pre existing chronic liver or kidney disease.
References
-
Wang GF, Li W, Li K (2010) Acute encephalopathy and encephalitis caused by influenza virus infection Acute encephalopathy and encephalitis caused by influenza virus infection. Curr Opin Neurol 23(3): 305-311.
-
Nagao T, Morishima T, Kimura H, Yokota S, Yamashita N, et al. (2008) Prognostic Factors in Influenza- Associated Encephalopathy. Pediatr Infect Dis J 27(5): 384-389. Pekova L, et al. Influenza-Associated Neurological Complications - Clinical Course and Prognostic Factors. Vaccines Vacccin 2018, 3(2): 000124.
-
Cox NJ, Subbarao K (2000) Global epidemiology of influenza: past and present. Annu Rev Med 51: 407- 421.
-
Newland JG, Laurich VM, Rosenquist AW, Heydon K, Licht DJ, et al. (2007) Neurologic complications in children hospitalized with influenza: characteristics, incidence, and risk factors. J Pediatr 150(3): 306-310.
-
Morishima T, Togashi T, Yokota S, Okuno Y, Miyazaki C, et al. (2002) Encephalitis and encephalopathy associated with an influenza epidemic in Japan. Clin Infect Dis 35(5): 512-517.
-
Steininger C, Popow Kraupp T, Laferl H, Seiser A, Godl I, et al. (2003) Acute Encephalopathy Associated with Influenza A Virus Infection. Clin Infect Dis 36(5): 567- 574.
-
Flewett TH, Hoult JG (1958) Influenza encephalopathy and post influenza encephalitis. Lancet 2: 11-15.
-
Fujimoto S, Kobayashi M, Uemura O, Iwasa M, Ando T, et al. (1998) PCR on cerebrospinal fluid to show influenza-associated acute encephalopathy or encephalitis. Lancet 352 (9131): 873-875.
-
Studahl M (2003) Influenza virus and CNS manifestations. J Clin Virol 28(3): 225-232.
-
Takanashia J, Barkovich AJ, Yamaguchia K, Kohnoa Y (2004) Influenza-Associated Encephalitis /Encephalopathy with a Reversible Lesion in the Splenium of the Corpus Callosum: A Case Report and Literature Review. AJNR Am J Neuroradiol 25(5): 798-802.
-
Hoult JG, Flewett TH (1958) Influenzal encephalopathy and post-influenzal encephalitis: histological and other observations. Br Med J 1: 1847- 1850.
-
Coffin SE, Leckerman K, Keren R, Hall M, Localio R, et al. (2011) Oseltamivir shortens hospital stays of critically ill children hospitalized with seasonal influenza: a retrospective cohort study. Pediatr Infect Dis J 30(11): 962-966.
-
Fiore AE, Shay DK, Broder K (2009) Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 58(8): 1-52.
-
Bhat N, Wright JG, Broder KR, Murray EL, Greenberg ME, et al. (2005) Influenza-associated deaths among children in the United States, 2003-2004. N Engl J Med 353: 2559-2567.
-
Ohmit SE, Monto AS (2006) Symptomatic predictors of influenza virus positivity in children during the influenza season. Clin Infect Dis 43(5): 564-568. Pekova L, et al. Influenza-Associated Neurological Complications - Clinical Course and Prognostic Factors. Vaccines Vacccin 2018, 3(2): 000124.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future