A Unique Case of Severe Morganella Morganii Meningitis in Patient with Spina Bifida Oculta and Dermal Sinus
This case report is about a 13-year-old male patient who had spina bifida oculta at L5-S1, combined with dermal sinus. He was admitted in the Clinic of Infectious Diseases of a University Hospital in Stara Zagora with typical clinical signs of acute meningitis. Based on the anamnestic, clinical, laboratory, microbiological, virological and imaging methods, bacterial meningitis caused by Morganella morganii was diagnosed. The disease had a prolonged, severe course requiring rehospitalisation and prolonged treatment. The causative agent was only cultivated in CSF, while blood, urine and copro cultures were negative. Antibacterial treatment, despite the wide range of susceptibility of the causative agent, did not result in a favorable response. The combination of conservative and operative therapy lead to eradication of the infection and recovery.
Introduction
| Morganella morganii is a Gram-negative | |
|---|---|
| microorganism, formerly known as Proteus morganii [1]. | |
| It has a commensal relationship within the intestinal | |
| tracts of humans, mammals, and reptiles as normal flora | |
| [2]. |
M. morganii is an uncommon cause of community acquired infections. Most commonly it occurs as a nosocomial infection of the urinary, digestive systems, and soft tissues after surgery [3]. Predisposing factors to the M. morganii infection are prolonged therapy with β- lactam antibiotics, diabetes, surgical procedures, old age, perinatal contamination [4]. We report a case of a 13- year-old boy with severe meningitis caused by M. morganii.
The child was born with Spina bifida oculta at L5-S1 level and according to the parents' data from the hairy recess in the sacral area occasionally a yellowish liquid flows out.
Surgical intervention to correct the anomaly was not conducted due to parents' disagreement. Up to 6 months of age, the patient experienced convulsions. The boy has proper neurological and physical development, he is a 7th grade student.
He was hospitalized at the Clinic of Infectious Diseases of the University Hospital in Stara Zagora on 10.08.2018
with complaints of headache, nausea, vomiting, fevering up to 37.8°C, with a 3-day duration.
From the physical exam, the patient was conscious, with fever of 38.4°C, pronounced photophobia, hyperemised throat, respiratory rate 44 of breaths/ min, heart rate of 120/min. From the neurological exam there was only neck stiffness with enhanced tendon reflexes.
At the L5-S1 level, a 0.5-0.7 cm groove was seen, masked by increased hair growth, with no visible evidence of an inflammation.
The complaints were of varying dynamics. A second fever peak to 39°C was displayed on the fifth day of the hospitalization.
Multiple CSF (cerebrospinal fluid) tests showed evidence for purulent meningitis - Leuc. up to 1098.106/L with polinuclears in 93%, glucose level 0,2 mmol/L. The blood, urine and coprocultures performed, as well as nasal, throat swabs and skin wash from the recess prior to the onset of antibiotic therapy without bacterial growth. M. morganii was proven from the first cultivation of CSF. Its identification was performed with a Vitek 2 Compact system (BioMerieux, USA) using a GN card. Antimicrobial susceptibility was tested with AST-N204 EUCAST, version 4.0.
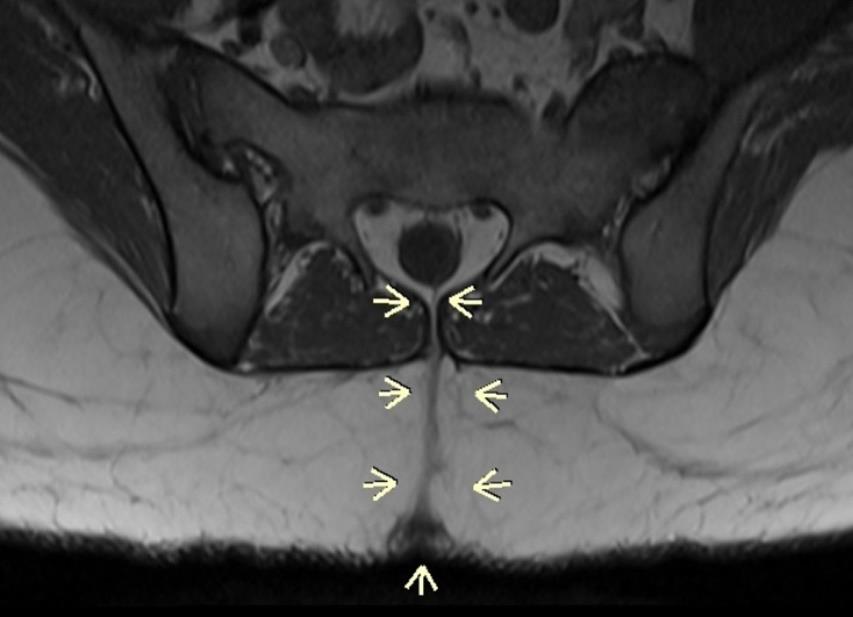
CT and MRI revealed an unclosed spinal arc without meningocelle. Dorsal dermal sinus was found in the lumbosacral section. On the S2 level there was seen a fistula between the spinal canal and the skin (Figure 1).
Pekova L, et al. A Unique Case of Severe Morganella Morganii Meningitis in Patient with Spina Bifida Oculta and Dermal Sinus. Vaccines Vacccin 2019, 4(1): 000129.
Etiological treatment according to the antibiogram - Ceftriaxon 2 x 2.0 g, Amikacin 2 x 500 mg i.v. was carried out for 16 days. Dexamethasone and Mannitol as osmodiuretic were added.
The patient was discharged with improvement. Therapy with Cefixime x 400 mg p.o was given for 7 days.
Five days after dehospitalization headaches, vomiting reappeared with dizziness and photophobia requiring re- hospitalization. On the readmission: fever up to 38.8°C with moderate neck stiffness and disturbed gait. Lumbar puncture revealed a relapse of the purulent meningitis by re-isolation of M. morganii from the CSF. Pleocytosis was higher than the previous stay – up to 7787.106/L with polinuclears in 97% and lower hypoglicorachia-0,02 mmol/L. M. morganii had the same antimicrobial sensitivity. This time a combination of Ceftazidime, Amikacin and Ciprofloxacin was started. The control lumbar punctures, showed a good response with reduction of pleocytosis, but retained proteinorachia and hypoglycorachia. Second peak of fever up to 39.3 ° C with increased headache, nausea and somnolence imposed change of antibacterial therapy with Meropenem 3 x 2.0 g and Sulfamethoxazole/Trimethoprim 2 x 1.0 g i.v. After a 22-days hospital period, objective status and laboratory parameters were improved, and the patient was referred to a neurosurgery clinic for surgical treatment of dermal sinus.
The condition of the patient was progressively improved after the intervention. At home therapy was continued with Trimetoprim/sulfametoxazol 2 x 960 mg for another 14 days p.o., Fluconazole x1 t. p.o. and probiotics. The routine examination after one month revealed normal somatic and neurological status, primarily healed surgical wound normal laboratory blood tests. Tracking up to the 6th month shows full recovery.
Discussion
The case presented was one of the few known cases of neuroinfection caused by M. Morganii [5]. As a primary location of M. morganii, infections of the urinary system were most commonly described [6]. The entrance door to M. morganii infection might be also the gastrointestinal system, skin and soft tissues [7].
In our patient, the urine, blood and coprocultures did not show bacterial growth.
Copyright© Pekova L, et al.
It was known that M. morganii is often found to be a nosocomial infectious agent [8]. However, our patient came with M. morganii neuroinfections from his home without previous hospitalization. The clinical picture of meningitis caused by M. morganii was presented with fever, neck stiffness, impaired consciousness, seizures, and CSF abnormalities [5]. All these findings were present in our patient, with the exception of seizures. The blood and CSF tests showed typical for bacterial neuroinfection changes. The incidence of M. morganii bacteraemia reached 70.5% especially as nosocomial infection [9]. In contrast, however, the blood cultures in our patient were negative.
The most severe cases had been reported in patients with impaired immunity [10]. The mmunoglobulins IgA, IgE, IgG, as well as C3 and C4 fractions of the complement in our patient were in reference values.
According to the literature, the intramedullary dermal sinus was localized most commonly in the lumbosacral region and frequently accompanied spina bifida oculta [11]. The imaging studies in our case indicated a synchronous presence of spina bifida with dermal sinus with external communication to the skin. The entry door of the infection was most likely the fistula. Some authors shared the idea of a direct invasion of M. morganii in the CNS [8].
Patient’s improving during the first hospital stay gave us reason to assume that the infection was well managed and the patient could recover completely with oral therapy at home with subsequent neurosurgical intervention. However, the repetition of purulent meningitis with the same etiological agent suggested that surgical intervention was imperative.
Patients with M. morganii bacteraemia usually had a severe clinical course with high lethality ranging from 36% to 42%, the prerequisite for which the data are diabetes mellitus, polymicrobial bacteraemia, and inadequate antibacterial therapy [12]. However, most cases of M. morganii infection were well-influenced by appropriate antibiotic therapy [13]. M. morganii had intrinsic resistance to oxacillin, ampicillin, amoxicillin, most of the first- and second-generation cephalosporins and macrolides [8]. In the present case, the isolated bacterium was sensitive to a wide range of antibiotics, ceftriaxone, ceftazidime, ertapenem, imipenem, tetracycline, aztreonam and trimethoprim/sulfamethoxazole.
Pekova L, et al. A Unique Case of Severe Morganella Morganii Meningitis in Patient with Spina Bifida Oculta and Dermal Sinus. Vaccines Vacccin 2019, 4(1): 000129.
Conclusion
We described unique case of an immunocompetent patient with M. morganii meningitis due to a fistula between a spinal canal and the skin in combination with spina bifida ocluta. In such cases the conservative treatment despite the good susceptibility of the isolated M. morganii is not enough to eradicate the neuroinfection. Therefore, the combination of antibacterial therapy with surgical treatment to eliminate the primary source is mandatory.
Acknowledgement
We are grateful to all physicians, nursing, laboratory staff and patients, who participated in this study. We thank the staff of the Clinic of Infectious diseases, Stara Zagora’s University Hospital for the medical care and treatment of the patients.
Conflict of Interest
All authors of this manuscript declare they have no competing interests. Funding Source: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Ethical Approval
All data used in this manuscript are given with the explicit consent of the patient's parents as he is a minor. The approval of the Ethics Committee at the University Hospital, Stara Zagora, Bulgaria, has been sought and received
References
-
Аbdalla J, Saad M, Samnati I, Lee P, Moorman J (2006) Central nervous system infection caused by Morganella morganii. Am J Med Sci 331(1): 44-47.
-
Cho YK, Kook H, Woo YJ, Choi YY, Ma JS, et al. (2006) Morganella morganii pericarditis in a child with X- linked agammaglobulinemia. Pediatr Int 52(3): 489- 491.
-
Erlanger D, Assous MV, Wiener-Well Y, Yinnon AM, Ben-Chetrita E (2019) Clinical manifestations, risk factors and prognosis of patients with Morganella morganii sepsis. Journal of Microbiology, Immunology Copyright© Pekova L, et al. and Infection. J Microbiol Immunol Infect 52(3): 443- 448.
-
Falagas ME, Kavvadia PK, Mantadakis E, Kofteridis DP , Bliziotis IA, et al. (2006) Morganella morganii infecti on in a general tertiary hospital. Infection 34(6): 315- 321.
-
Kim BN, Kim NJ, Kim MN, Kim YS, Woo JH, et al. (2003) Bacteraemia due to tribe Proteeae: a review of 132 cases during a decade (1991-2000). Scand J Infect Dis 35(2): 98-103.
-
McDermott C, Mylotte JM (1984) Morganella morganii: epidemiology of bacteremic disease. Infect Control 5(3): 131-137.
-
Milligan KL, Barenkamp SJ (2013) Neonatal meningitis due to Morganella morganii. Clin Pediatr (Phila) 52(5): 462-464.
-
Nakazawa T, Obinata K, Nagata Y, Ebara K, Suzuki K, et al. (2013) A Case of Morganella morganii Meningoencephatitis. J Infect Dis Ther 1: 118. Pekova L, et al. A Unique Case of Severe Morganella Morganii Meningitis in Patient with Spina Bifida Oculta and Dermal Sinus. Vaccines Vacccin 2019, 4(1): 000129.
-
Najjar MW, Kusske JA, Hasso AN (2005) Dorsal intra medullary dermoids. Neurosurg Rev 28(4): 320-325.
-
Ndiaye M, Sène MS, Sow AD, Seck LB, Coulibaly T, et al. (2010) Meningoencephalitis due to Morganella morganii: A case report. Bull Soc Pathol Exot 103(4): 230-232.
-
O’Hara CM, Brenner FW, Miller JM (2000) Classification, identification and clinical significance of Proteus, Providencia and Morganella. Clin Microbiol Rev 13(4): 534-546.
-
Tucci V, Isenberg HD (1981) Hospital cluster epidemic with Morganella morganii. J Clin Microbiol 14(5): 563-566.
-
Yu-Tin Chen, Hwei-Ling Peng,Wei-Chung Shia, Fang- Rong Hsu, Chuian-Fu Ken, et al. (2012) Whole- genome sequencing and identification of Morganella morganii KT pathogenicity-related genes. BMC Genomics 13(7): S4. Copyright© Pekova L, et al.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future