Current Status of Contraceptive Vaccines
The rapidly increasing global population has bowed the attention of family planning and associated reproductive health programmes in the direction of providing a safe and reliable method to limit family size. The world population is estimated to exceed a phenomenal 10 billion by the year 2050 A.D., thus presenting a real jeopardy of overpopulation with severe implications for the future. There are over one million elective abortions globally each year due to unintended pregnancies having devastating impact on reproductive health of women worldwide, despite the availability of various contraceptive methods. This highlights the need for the development of newer and improved contraceptive methods. A novel contraceptive approach that is gaining substantial attention is “Contraceptive Vaccines†targeting gamete production, gamete outcome, or gamete function. These vaccines may also find applications in clinical situations, such as in uterine fibroids, polycystic ovary syndrome, endometriosis and precocious puberty, that require the inhibition of increased secretions of sex steroids. Antisperm antibodies (ASAs) are invariably present in both females and males. However, the degree of ASA occurrence may vary according to individual and gender. Although the extent of infertility due to ASAs alone is yet to be determined, it has been found in almost 9–12% of patients who are infertile due to different causes. Vaccines targeting gamete outcome primarily focus on the HCG molecule. The HCG vaccine is the first vaccine to undergo Phase I and II clinical trials in humans. The other type of anti-hCG vaccine, developed with support from the WHO Task Force on Vaccines for Fertility Regulation, is based on a portion (the carboxyterminal peptide or CTP) of the beta subunit of the hormone (ß-hCG-CTP). This review is an attempt to analyze the current status and progress of immunocontraceptive approaches with respect to their role as a future fertility control agents.
Introduction
The human population which is increasing in several developing countries of Asia and Africa has severe consequences leading to depletion of natural resources, scarcity of drinking water, threatening food security, in addition to its impact on the environment. In spite of introducing steroid hormones based oral contraceptive pills (introduced in 1955), implants, intrauterine devices, male and female condoms, and surgical interventions such as tubectomy and vasectomy, world human population (crossed 7 billion by November, 2011) is still growing (http://www. worldometers.info/world-population/). It is estimated that human population may cross 9 billion by 2046.
Contraception is an accepted route for the control of population explosion in the world [1]. The need for contraception varies for different couples from postponing child bearing, spacing childbirth and limiting family size to absolute no child bearing which is highly personal decision based on their individual preferences, medical history, life style and other factors [2]. An ideal contraceptive should be acceptable by user, with no loss of natural feeling, no side effects, relatively inexpensive, effective, easy to use and reversible. Both men and women are accessible to the various contraceptive choices present. Immunocontraception, in which there is use of contraceptive vaccines (CVs) or preformed antibodies to prevent fertilization, is gaining substantial attention. As with the conventional vaccines, CVs utilise the body’s defence system to wedge an essential step in the reproductive process [3]. Such a vaccine entails generating either humoral and/or cell mediated immune response against hormones/proteins that have critical role during reproduction. Their biological activity will be neutralized by the immune response elicited leading to block of fertility. Nature’s experiments supported the feasibility of developing contraceptive vaccine wherein the presence of naturally occurring auto-antibodies against sperm, zona pellucida (ZP) and follicle stimulating hormone (FSH) in women and men were associated with idiopathic infertility [4, 5, 6, 7].
A successful contraceptive vaccine must be reliable, easy to administer, safe, affordable, widely acceptable, and capable of evoking homogeneous response and must be highly efficacious. The methods of birth control currently available can be classified broadly into steroid hormone methods (oral pills, injectable preparations and implants),barrier methods (condoms and caps),inert and medicated devices (IUDs), chemical methods (spermicidal foams and gels), surgical methods (salpingectomy and vasectomy), and various combinations of these approaches. The range of options is still limited in spite of these methods finding wide acceptance in many parts of the world and having a major impact in the family planning arena. Various drawbacks associated with many of the methods are, concerns about the safety of their long-term use, inconvenience of use, unreliability, and permanence of effect, which limit their acceptance and availability in the widely differing social, cultural, religious, service and personal settings of users in many developing countries.
Safe, Effective and Acceptable Contraceptive Vaccines
Safe, Effective and Acceptable Contraceptive Vaccines may be an attractive addition to the currently available range of family planning methods in that they would:
- Confer long-term (but not permanent) protection following a single course of immunization.
- Be free of overt pharmacological activity and the metabolic and endocrine disturbances that often accompany other methods of birth control.
- Not require insertion of a device or implant.
- Remain effective without continuous conscious action by the user.
- Be inexpensive to manufacture.
The term contraceptive vaccines should be used only in connection with those vaccines which have an effect prior to fertilization. However, over the years, this term has been used to describe all vaccines having an antifertility effect, irrespective of whether this occurs prior to fertilization or after fertilization and prior to the completion of implantation of the blastocyst. The term fertility regulating vaccines (FRVs) has been introduced to avoid the confusion caused by this incorrect usage [8].
Options for FRV Development
The early stages of mammalian reproduction are a complex series of events which can be divided into three stages for convenience:
- The production and transport of the male and female gametes (sperm and ova).
- The interaction of the gametes leading to fertilization.
- The process of implantation of the developing embryo into the uterine endometrium.
Selection of Molecules for FRV Development
The most attractive candidates for FRV development are molecules which:
- When eliminated or neutralized by immunological means will result in a safe, effective and acceptable means of fertility regulation.
- Are restricted to the intended target cell or tissue.
- Are present in a site where a controlled immune response will not lead to immunopathology.
- Are present transiently and/or at low levels compared to the anticipated immune response.
- Will not elicit other undesirable immune responses.
- Can be chemically characterized and easily manufactured in large quantities and at low cost.
![Figure 1: Mechanism of action that can produce successful immunocontraception along with potential antigens that can be used as vaccine candidates are depicted [9].](/fulltextimages/6669/fig_1.png)
Current Status of FRV Development
Anti-Sperm Vaccines
Two types of sperm antigens have been focused by the research on anti-sperm vaccines:-
- Functional antigens such as the enzymes known (or suspected) to be required for sperm metabolism (lactic dehydrogenase-X) or involved in sperm-egg interactions and the processes leading to fertilization (acrosin and hyaluronidase).
- Structural antigens such as the molecules expressed on the sperm cell membrane and which may be involved in gamete interaction and fusion [8].
Sperm Enzymes
Several animal species (mice and rats ~ 55%, rabbits ~ 70%, and baboons ~ 30%) which have been actively immunized with mouse lactic dehydrogenase-X (LDH-X or LDH-C4) and with a synthetic peptide based on a portion of the molecule, have shown varying degrees of fertility reduction. A cDNA expression library which is derived from human testis has been screened with polyclonal and monoclonal antibodies raised to murine LDH-C4. This research has resulted into the deduction of the nucleotide sequence coding for human LDH-X and engineering it into an expression vector system. A vaccine containing the LDH-X antigen prepared in this way is currently being evaluated in a preliminary efficacy trial in baboons.
Although anti-acrosin antibodies have been shown to inhibit the action of this enzyme on substrates invitro and that anti-hyaluronidase antibodies could inhibit rabbit in vitro fertilization, active immunization of rabbits and sheep with these two enzymes, either alone or in combination, did not result in a significant reduction in fertility. There is no major vaccine research programmer involving these particular antigens, in progress currently.
Sperm Membrane Antigens
An opportunity is provided by the recent advances that have occurred in the field of molecular genetics and in the production of monoclonal antibodies (MAbs) to identify, isolate, and synthesize peptides, representing part or all of the primary structure of selected protein molecules, which can be evaluated subsequently as antifertility immunogens. SP- 10 and PH-20, the two sperm antigens identified in this way, have been shown to have promising antifertility effects on getting injected into laboratory animals. Antifertility studies with these antigens, in primates, are further underway or planned. In infertile men and women, the presence of antibodies against an antigen is very interesting since it indicates: (i) association of these antibodies and antigens with human infertility; (ii) immunogenicity of these antigens in humans; and (iii) since most infertile men and women are healthy individuals without any disease concomitant with infertility, the presence of antibodies to an antigen is indicative, though not confirmatory, of sperm specificity.
Thus, if an antigen is involved in human immune infertility, extensive Phase I clinical trials to investigate the immune pathological consequences in actively immunized subjects may not be absolutely necessary. These immune infertile men and women provide involuntarily vaccinated models that illustrate how a CV based on sperm antigens will work in humans. There has been a lot of interest in delineating those antigens that are involved in ASA-mediated immune infertility. However, only a few antigens have been identified that have been shown to be clearly associated with human immune infertility [10].
Recently, promising research studies focusing on different aspects of ASAs in the reproductive biology of humans and other species have been considered. The usefulness of sperm antigens or ASAs (recombinant) as human/animal contraceptive vaccines although revealed, is yet to be validated via clinical testing. To overcome ASA- induced infertility in people who wish to have children, progress has been made in research associated with the development of techniques. The process of ASA generation in both human males and females is poorly understood and is a subject area that deserves further attention and research.
Various arguments have been put forward regarding the testing of males for ASAs on a routine basis, but it is assumed that such approaches are not always mandatory. Therefore, all the above findings show that ASAs impair the motility of spermatozoa, transport of sperm through the female reproductive tract, sperm survival, acrosome reactions, fusion of sperm, and oocyte and embryo development. Since specific targeted therapies against ASAs are not in practice yet, assisted reproductive technologies (ART) are the appropriate alternative choices for healthy conception [11].
Anti-Ovum Vaccines
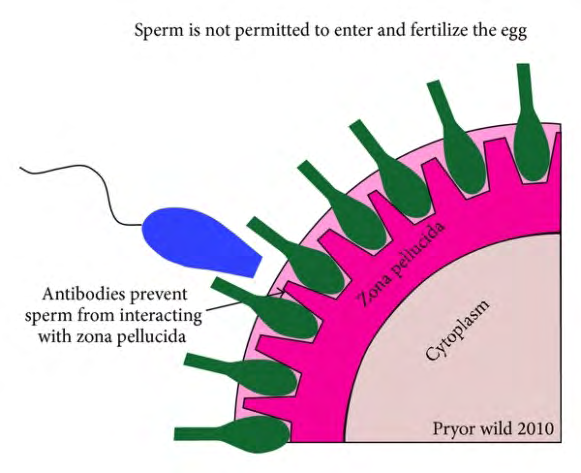
The majority of the research directed at developing an anti-ovum vaccine has focused on the zona pellucida (ZP), which is a jelly-like glycoprotein coat surrounding the egg. It acts as a source of potential candidate antigens because of its crucial role in the gamete interactions that leads to fertilization.
Crude preparations of solubilized whole porcine ZP consisting of active or passive immunization has been shown to reduce the fertility of the females of several species of laboratory animals including baboons [12]. However, amenorrhea of variable duration was observed in majority of the immunized baboons. This can suggest possible intraovarian complications. Efforts are now in progress to isolate antigens which are expressed on the surface of the ZP and are involved in sperm-ZP interactions only during the peri- and post-ovulatory period.
Amino acid sequence data on some of the protein components of ZP have been obtained. Anti-ZP antibodies have been produced by a mice immunized with a 16 amino acid peptide of one of the ZP proteins. This has exhibited reversible infertility with no evidence of ovarian damage seen [13]. No convincing data have been presented till date that indicates that a zona-specific antigen of defined chemical structure can inhibit fertility without causing an inflammatory reaction in the ovary. This might be indicative of a risk of acute ovarian disturbances or long-term immunopathology.
Recently, murine ZP3 and sperm specific (YLP-12) epitope were expressed with Johnson grass mosaic virus coat protein to present antigens as virus like particles (VLPs) [14]. Immunization of animals resulted in significant infertility. The results were quite encouraging as well as suggestive of the possibility of using above mentioned approaches for immune contraception. However, long term studies showed that immunization with zona antigens might induce immunological attack on many eggs in the ovary which might lead to premature ovarian failure [15]. Hence, enough data needs to be gathered before zona antigens are given any place in the market as immune contraceptive measure [16].
Anti-Conceptus Vaccines
A number of placenta-specific antigens have been investigated to be candidates for vaccine. As with studies on sperm antigens, both structural antigens, forming part of the trophoblast cell membrane, and functional antigens, such as placental hormones, have been evaluated.
Structural Placental Antigens
ß1 glycoprotein (SP-1) i.e. pregnancy-specific, is a placental protein, rapidly secreted by the syncytiotrophoblast. It can be detected by immunofluorescence in the cytoplasm and on the plasma membrane of this tissue [17]. Although
an antifertility effect was observed when female baboons and cynomolgus monkeys were actively immunized with human SP-1, in the majority of cases (50-80%), this effect was manifested as a late abortion. In contrast, no antifertility effect was seen in similarly treated rhesus monkeys. No such effect was observed in rhesus monkeys immunized with rhesus SP-1, even in the presence of high titres of anti-SP-1 antibodies.
Similar studies in baboons indicated that the rate of secretion of SP-1 in early pregnancy was probably too high to be neutralized by the antibody in the maternal circulation. Another placental antigen PP-5, unlike SP-1, is not found in the cytoplasm of trophoblast cells but appears to be an integral component of the cell membrane. It is present in a low concentration in trophoblast tissue, is not secreted into the maternal circulation and is very difficult to isolate from placental tissue.
However, a small group of female monkeys was actively immunized with human PP-5 and it led to a substantial reduction in fertility. Attempts to extend these studies, by immunizing rhesus monkeys with rhesus PP-5, were thwarted by the major difficulties experienced in obtaining a sufficient number of rhesus placentae from which the protein is isolated [18]. Trophoblast-derived gene libraries are being screened to facilitate and accelerate the definition of chemical structure of the more promising candidate antigens, with appropriate MAbs and PAbs to isolate. This will subsequently sequence the genes coding for these molecules. The primary structure of the antigen can be deduced from the nucleotide sequence thus obtained. The corresponding peptides should be synthesised for evaluation as candidates for vaccine development. Several candidate molecules have been identified in this way and are currently being evaluated for tissue-specificity and antifertility efficacy [19].
Hormonal Placental Antigens
By far the greatest amount of work carried out over the past two decades has been concerned with the development and clinical testing of vaccines directed against the glycoprotein hormone, human chorionic gonadotropin (hCG). HCG, which is produced by the trophectoderm of the pre-implantation embryo, within a few days of fertilization, changes its function to the maintenance of the corpus luteum in the ovary.This ensures its continued production of progesterone.
Since progesterone is needed for the successful completion of implantation of the blastocyst, if the production or function of hCG can be inhibited immunologically, the corpus luteum would regress, its production of progesterone would decline and menstruation would occur at or about the expected time, thus mimicking the events that occur naturally in a non-conceptual cycle [8].
One type of anti-hCG vaccine, developed by the Population Council in New York and by the National Institute of Immunology (NII) in New Delhi, is based on the whole beta subunit of the hormone (ß-hCG) [20, 21]. The other type of anti-hCG vaccine, developed with support from the WHO Task Force on Vaccines for Fertility Regulation, is based on a portion (the carboxyterminal peptide or CTP) of the beta subunit of the hormone (ß-hCG-CTP) [22, 23, 24, 25]. The reason for these two different approaches to the development of anti- hCG vaccines is that in 1974 WHO opted for the theoretically safer approach of the CTP vaccine. This was followed by the demonstration of the cross reactivity of antibodies which were raised to the whole ß-subunit with human luteinizing hormone (hLH). It was further followed by the concerns that this raised about possible ovulation inhibition, potential immunopathology and menstrual cycle disturbances.
The CTP vaccines do not raise such antibodies. Recent data from the Population Council and NII clinical trials with their respective ß-hCG vaccines indicate no menstrual cycle disturbances and no effect on ovulation. The question of long-term immunepathological or other squeal, if any, of the elicited cross-reactive immunity to hLH, is still unresolved. The Population Council ß-hCG vaccine has been tested in a Phase I clinical trial and has been reported to be immunogenic and free of short-term side-effects [21]. The NII ß-hCG vaccine has been tested in both Phase I and Phase II clinical trials and has also been reported to be free of short- term side-effects as well as being effective in preventing pregnancy [20].
A Phase I clinical trial has been conducted with the ß-hCG-CTP vaccine [26]. The antibody titers raised in this Phase I trial were estimated to be in excess of the level needed to neutralize the hCG in the maternal circulation at the time of implantation. The first and only birth control vaccine against HCG has gone through Phase II efficacy trials successfully. It has also shown to protect sexually active women from becoming pregnant [27]. It was a highly effective vaccine which resulted into one pregnancy in 1224 cycles so long as the antibody titers remained >50 ng/ml. The vaccine was fully reversible and women conceived readily when the antibody titres declined to <35 ng/ml. The uniqueness of this vaccine is that it is directed against a molecule which is made in detectable amounts only in pregnancy in healthy women. The vaccine is devoid of side-effects, as observed in >200 women during Phase I and Phase II trials. Women menstrual cycles are regular, making their own sex hormones and keep ovulating normally.
No irregularity of bleeding in terms of spotting, amenorrhea or extra bleeding occurs [28]. The fact that luteal phase did not lengthen in vaccinated women provided confirmation of the previous work in marmosets on anti- HCG antibodies preventing implantation of the embryo onto the endometrium. Interception is therefore before the onset of pregnancy [29]. The above protective threshold titers were generated in only 60–80% of women, which was the shortcoming of the vaccine. This degree of efficacy is highly satisfactory for vaccines against infectious diseases but a birth control vaccine in order to be acceptable has to be effective in >90– 95% of recipients. Further work is required on product development. More potent adjuvants, available today from the pharmaceutical industry, would be required, instead of the alum employed in the test vaccine. Currently, there is constant need to monitor the vaccinated individuals for the presence/absence of sufficient antibody titers that can lead to blockage of conception.
All of these anti-hCG vaccines require multiple injections to achieve and maintain effective levels of immunity. Studies are in progress to develop various formulations of these vaccines. These formulations will provide long-acting protection after a single injection. Data was obtained in preliminary studies with the ß-hCG-CTP vaccine which was incorporated in the biodegradable polymers. Using this technology, it may be possible to produce a vaccine offering one year of protection from a single administration [30].
Anti-LHRH/GnRH Vaccine
The decapeptide LHRH has some unique characteristics. A vaccine against LHRH is usable in both sexes due to its presence in both males and females. Its primary structure is largely conserved in mammals. Thus rodents can be employed as a homologous model for safety and efficacy. Furthermore anti-LHRH approaches can be employed for control of fertility, libido, and sex steroid production in dogs (companion animals), pigs, bulls and heifers (animals raised for meat production). Given that sex steroids promote the growth of accessory reproductive organs such as prostate and breasts, anti-LHRH treatment has therapeutic applications in sex hormone-dependent cancers [31].
Passive Immunization: An Effective Approach
The idea of using passive immunization for immune contraception was based on the clinical reports of infertile men. Their semen contains antibodies that immobilize sperm usually by agglutination. Previous studies data indicated that sperm agglutinating/immobilizing antibodies must be present in the reproductive tract specifically vagina. This will provide significant immune protective effect from pregnancy. Earlier reports have examined the stability of antibodies in mucus secretions and found that antibodies whether polyclonal/monoclonal are stable in seminal fluid and cervical mucus at 37°C. The antibodies can provide protection for one to several days depending on their half-life and the use of gels for the delivery of antibodies will result in sustained release [32, 33].
Further, monoclonal antibodies have been raised against MA-24, which is a human sperm and rabbit sperm, and mouse anti-rabbit sperm (MARS). Naz, et al found that systemic intraperitoneal injection of MA-24 ascites fluid in mouse models reduced the percentage of fertilized ova (from 69% in untreated to 29% in treated), thereby reducing the fertility in vivo [34, 35]. For determining the in vivo contraceptive efficacy of MARS, the antibodies were incubated in vitro with a defined volume of semen, followed by insemination of females. All the mAbs were found contraceptive effective [36].
Strengths and Weaknesses of Contraceptive Vaccines
The infrastructure to deliver vaccines exists in most of the developing countries, which is one of the strengths of the contraceptive vaccines. It is likely that the immunological approaches for contraception are cost-effective and free from the risk of failure of the user. Contraceptive vaccines are meant for young and healthy subjects, for whom alternate methods of contraception such as steroid hormones based oral pills and implants, intrauterine devices and male and female condoms, are available as compared with the vaccines for prevention of infectious diseases. Hence, it is of vital importance that the contraceptive efficacy achieved by vaccines should be comparable to the above alternate available options. However, β-hCG based contraceptive vaccine, only one that has been evaluated in humans, firstly, has not shown contraceptive efficacy that is comparable to any of the other alternative available contraceptive options described above. Secondly, major drawback of the contraceptive vaccines is the variability of immune response among immunized individual subjects. Variability of immune response is not unique to contraceptive vaccines as it is also a common feature with vaccines meant for prevention of infectious diseases. However, the saving factor in the latter is the statistical improbability of every one in a community getting infected whereas every human subject opting for anti-fertility vaccine would be of proven fertility. The observed variability in immune response in the vaccinated women will warrant monitoring of antibody titres at regular periods to arrive at decision about administering booster injection. It may be an intimidating task, especially in the developing countries, in the Family Planning Program.
Thirdly, the safety of contraceptive vaccines is critical to establish beyond doubt. Long-term safety studies over 15 to 20 years including tautological studies should be undertaken, before contraceptive vaccines may be recommended for human use. Contraceptive vaccines based on immune- mediated neutralization of GnRH and LH may have utility only in the control of fertility in animals and are not likely to be safe or acceptable for eventual human application (Table 1). Contraceptive vaccines based on either spermatozoa- or egg-specific proteins and aiming to inhibit the process of fertilization rather than gametogenesis would in principle be acceptable for human application. Long-term follow- up studies of the porcine ZP-based contraceptive vaccine immunized feral horses and white-tailed deer revealed no significant deleterious effects on the health of the immunized animals except oophoritis [37, 38, 39].
Follow-up of the immunized feral horses between
1990 to 2002 revealed no significant effect of porcine ZP contraception on the season of birth or foal survival as compared with unvaccinated feral horses habituating Assateague Island National Seashore, Maryland, USA [38]. The block in fertility was reversible [37]. Subsequent fertility was not affected in the female offspring born to vaccinated mothers [37]. White-tailed deer vaccinated with porcine ZP-based contraceptive vaccine showed ovarian pathology representing eosinophilia oophoritis [39]. Thus, the vaccines based on gamete specific antigens require extensive safety studies in various experimental animal models before these can be considered for even Phase I safety and immunogenicity studies in human subjects (Table 1). ZP-based immunogens should not induce oophoritis. Among the two contraceptive vaccines, one based on oFSH that has undergone Phase I trials in men and the second based on β-hCG which has gone through Phase II efficacy studies, the latter seems to have higher probability of clinical application (Table 1).
| Strength | Weakness | Clinical Application | |
|---|---|---|---|
| GnRH | Workable in both males and females. contraceptive efficacy demonstrated in animals | Inhibit secretion of gonadotropins, sex steroid hormones and atrophy of reproductive organs | Useful for veterinary application. Not likely to be used in humans |
| LH | Contraceptive efficacy evaluated in non-human primates | Disturbance in steroid hormonal profile | Not being pursued for veterinary or human use |
| FSH | Extensive Immunization studies in non-human primates. Phase I clinical studies in men | Discrepant results on the efficacy to decrease spermatogenesis in non-human primates | Additional safety and efficacy studies needed |
| Sperm-specific proteins | several sperm-specific proteins documented and Contraceptive efficacy established in animals | Lon-term safety studies not performed | good candidate for development of contraceptive vaccine for human |
| zona pellucida | Contraceptive efficacy demonstrated in animals. Long-term follow-up immunized animals showed to debilitating effect on health | Generate oophoritis | Useful for veterinary application. Design Not eliciting oophoritis critical for in humans use |
| hCG | Safety studies performed. Demonstrated contraceptive efficacy in women. Block in fertility reversible | Inadequate protective antibody titers in all vaccinated women. Variability in immune response amon women | Good candidate for developing contraceptive vaccine for human |
Table 1: Strength and Weakness of Various Contraceptive Vaccines. Major Challenges in the Application of Contraceptive Vaccines O
Table 1: Strength and Weakness of Various Contraceptive Vaccines. Major Challenges in the Application of Contraceptive Vaccines One of the common denominators, whether the contraceptive vaccines are meant for humans or wildlife population management, is to improve their immunogenicity. Further, the immune response elicited by contraceptive vaccines should be long lasting so as to achieve contraceptive efficacy of at least one year. It is desirable that the infertility mediated by contraceptive vaccine in humans is reversible.
In the context of wildlife population management, it will be ideal, if single injection of contraceptive vaccine generates adequate antibody titers leading to permanent sterility.
Thus, it is crucial to develop more potent adjuvants and novel vaccine delivery platforms. Additionally, the safety of the contraceptive vaccines that entails generating immune response against the self-protein(s) needs to be established beyond doubt. Both in-vitro and in-vivo experimental model systems should be developed to establish safety of contraceptive vaccines before clinical trials are initiated in humans. In addition, the adverse effects on the health of the progeny born to vaccinated human subjects in cases of vaccine failure should be addressed. Attempts have been made to address this issue in women immunized with β-hCG based contraceptive vaccine. The anti-fertility effect of the vaccine was reversible as women with low anti-hCG antibody titers conceived and pregnancy progressed to term [40].
Children born showed normal early developmental parameters [40]. However, additional safety studies need to be pursued more rigorously and for longer duration of say 20- 25 years, before contraceptive vaccine can be recommended for fertility regulation in humans. It will be another challenge to deliver vaccine to free roaming animals. In such cases, immunization through either oral route using edible baits incorporating contraceptive immunogen or by dart-gun may provide viable solutions.
Future Prospects and Needs
Vaccine Optimization
The first FRV vaccine to enter large-scale clinical use is likely to be the single-injection version of the anti-hCG vaccine. However, further studies are being carried out to develop an optimized anti-hCG vaccine. It will incorporate alternative hCG peptides, T-helper cell epitopes, new immunostimulants and delivery systems. The variation in the extent and duration of individual immune responses elicited by vaccines can be controlled, which is being addressed by other studies. Strategies are being developed to provide protection during the lag period following injection of the vaccine and the attainment of an effective level of immunity [8].
Long-Term Safety
Although FRVs are designed to have a comparatively short duration of effect (approximately 12 months), some individuals may use them repeatedly to receive protection for a period of several years. It is imperative, therefore, that long-term safety studies are carried out to determine the nature, extent and consequences of such long-term use. If cross-reactive immunity is detected in non-target cells or tissues, appropriate tests of both structural and functional effects need to be conducted. If a pregnancy occurs in the presence of sub-effective immunity, an additional careful examination in a relevant animal model is needed of the effect, if any, on the mother and fetus/offspring.
Mechanism of Action, Reversibility and Choice
FRVs could act by preventing sperm production, by interfering with ovulation, by inhibiting fertilization, or by preventing implantation of the blastocyst. It is important that studies are carried out to clearly determine how each FRV works. By understanding their mechanisms of action, more efficient and predictable FRVs can be prepared and rational intervention strategies can be developed to reverse the effects of the FRVs on demand. In addition, the user would be able to be fully informed of the known or suspected mechanisms of action of FRVs so that he or she can choose a FRV compatible with their personal needs and beliefs.
![Figure 3: Schematic model indicating various targets that are being explored for the contraceptive vaccine development. These include targeting gamete production [gonadotropin-releasing hormone (GnRH), follicle- stimulating hormone (FSH), and luteinizing hormone (LH)], gamete function [zona pellucida (ZP) proteins of the oocytes and sperm antigens], and gamete outcome (human chorionic gonadotropin [hCG]) [41].](/fulltextimages/6669/fig_3.png)
Figure 3: Schematic model indicating various targets that are being explored for the contraceptive vaccine development. These include targeting gamete production [gonadotropin-releasing hormone (GnRH), follicle- stimulating hormone (FSH), and luteinizing hormone (LH)], gamete function [zona pellucida (ZP) proteins of the oocytes and sperm antigens], and gamete outcome (human chorionic gonadotropin [hCG]) [41].
References
-
Mathew K, Bantwal G (2012) Malecontraception. Ind J Endocrinol Metab 16(6): 910-917.
-
Schwartz JL, Gabelnick HL (2002) Current contraceptive research. Perspectives on Sexual Reprod Health 34(6): 310-316.
-
Frayneand J, Hall L (1999) The potential use of spermantigensis targets for immunocontraception; past, present and future. J Reprod Immunol 43: 1-33.
-
Ingerslev HJ (1981) Antibodies against spermatozoal surface-membrane antigens in female infertility. Acta Obstet Gynecol Scand S100: 1-52.
-
Francavilla F, Santucci R, Barbonetti A, Francavilla S (2007) Naturally-occurring antisperm antibodies in men: interference with fertility and clinical implications. An update. Front Biosci 12: 2890-2911.
-
Kelkar RL, Meherji PK, Kadam SS, Gupta SK, Nandedkar TD (2005) Circulating auto-antibodies against the zona pellucida and thyroid microsomal antigen in women with premature ovarian failure. J Reprod Immunol 66: 53-67.
-
Haller Kikkatalo K, Salumets A, Uibo R (2012) Review on autoimmune reactions in female infertility: antibodies to follicle stimulating hormone. Clin Dev Immunol 2012: 762541.
-
Griffin PD (2019) Contraceptive vaccines. Special Programme of Research, Development and Research Training in Human Reproduction, World Health Organization.
-
Kaur K, Prabha V (2014) Immunocontraceptives: New Approaches to Fertility Control. Department of Microbiology, Panjab University, Chandigarh160014, India.
-
Naz R, Gupta S, Gupta J, Vyas H, Talwar GP (2005) Recent advances in contraceptive vaccine development: a mini- review 20(12): 3271-3283.
-
Vickram AS, Dhama K, Chakraborty S, Samad HA, Latheef SK, et al. (2019) Role of Antisperm Antibodies in Infertility, Pregnancy, and Potential for Contraceptive and Antifertility Vaccine Designs: Research Progress and Pioneering Vision 7(3): 116.
-
Gwatkin RBL, Williams DT, Carlo DJ (1977) Immunization of Mice with Heat-Solubilized Hamster Zonae: Production of Anti-Zona Antibody and Inhibition of Fertility. Fertil Steril 28(8): 871-877.
-
Millar SE, Chamov SM, Balir AW, Oliver C, Robey F, et al. (1989) Vaccination with a synthetic zona pellucida peptide produces long-term contraception in female mice. J Science 246(4932): 935-938.
-
Gupta SK, Gupta N, Suman P (2011) Zona pellucida- based contraceptive vaccines for human and animal utility. J Reprod Immunol 88(2): 240-246.
-
Paterson M, Koothan PT, Morris KD (1992) Analysis of the contraceptive potential of antibodies against native and deglycosylated porcine ZP3 in vivo and in vitro. Biology Reproduction 46(4): 523-534.
-
Naz RK (2005) Contraceptive vaccines. Drugs 65(5): 593-603.
-
Bohn H, Weinmann E, Gynak A (1974) Pregnancy Proteins in Animals 217: 209-218.
-
Botev B, Cinader B, Griffin D, Hay F, Kehayov I, et al. (1979) Immunol Reprod. Bulgarian Academy of Sciences, Sofia, pp: 136-143.
-
Anderson DJ, Johnson PM, Alexander NJ, Jones WR, Griffin PDJ (1987) Monoclonal antibodies to human trophoblast and sperm antigens: Report of two WHO- sponsored workshops, June 30, 1986-Toronto, Canada. Reprod Immunol 10(3): 231-257.
-
Talwar GP, Hingorani V, Kumar S, Banerjee A, Shahani SM (1990) Phase I clinical trials with three formulations of anti-human chorionic gonadotropin vaccine. Contraception 41(3): 301-316.
-
Thau R, Croxatto H, Luukkainen T, Alvarez F, Brache V, et al. (1989) Reprod Immunol. Elsevier Amsterdam, pp: 237-244.
-
Rose NR, Burek CL, Smith JP (1988) Safety evaluation of hCG vaccine in primates: auto antibody production. Contraception Research for Today and the Nineties 1: 231-239.
-
Lekhwani S, Vaswani ND, Ghalaut VS, Shanker V, Singh R (2014) Immunocontraceptives: How far from reality?. Adv Biomed Res 3: 247.
-
Rock EP, Reich KA, Lyu DM, Hovi M, Hardy J, et al. (1996) Immunogenicity of a fusion protein linking the beta subunit carboxyl terminal peptide (CTP) of human chorionic gonadotropin to the B subunit of Escherichia coli heat-labile enterotoxin (LTB). Vaccine 14(16): 1560- 1568.
-
Veron CS, John EP, Arthur CL, David G (1981) Antifertility Effects of Immunization of Female Baboons with C-Terminal Peptides of the β-Subunit of Human Chorionic Gonadotropin. Fertil Steril 36(1): 98-105.
-
Jones WR, Bradley J, Judd SJ, Denholm EH, Ing RMY, et al. (1988) Phase I Clinical Trial Of A World Health Organisation Birth Control Vaccine. The Lancet 331(8598): 1295-1298.
-
Talwar GP, Singh O, Pal R, Chatterjee N, Sahai P, et al. (1994) A vaccine that prevents pregnancy in women. Proc Natl Acad Sci USA 91(18): 8532-8536.
-
Talwar GP, Singh O, Gupta SK, Hasnain SE, Pal R, et al. (1997) The HSD-hCG vaccine prevents pregnancy in women, feasibility studies of reversible safe contraception vaccine. Am J Reprod Immunol 37(2): 153-160.
-
Hearn JP, Gidley-Baird AA, Hodges JK, Summers PM, Webley GE (1988) Embryonic signals during the peri- implantation period in primates. J Reproderi Fertil 36(4): 49-58.
-
Stevens VC, Powell JE, Lee AE, Kaumaya PTP, Lewis DH, et al. (1992) Proceedings of the international symposium on controlled release of bioactive materials. Controlled Release Society, pp: 112-113.
-
Talwar GP (1999) Vaccines and passive immunological approaches for the control of fertility and hormone- dependent cancers. Immunol Rev 171: 173-192.
-
Talwar GP, Diwan M, Dawar H, Frick J, Sharma SK, et al. (1998) Counter GnRH vaccine. In Rajalakshmi M and Griffin PD (Eds,) Male Contraception Present and Future. New Age International, New Delhi, pp: 309-318.
-
Sherwood JK, Zeitlin L, Chen X, Whaley KJ, Cone RA, et al. (1996) Residence Half-Life of IgG Administered Topically to the Mouse Vagina. Biology of Reproduction 54(1): 264-269.
-
Naz RK, Phillips TM, Rosenblum BB (1986) Characterization of the fertilization antigen1 for the development of a contraceptive vaccine. Proceedings of the National Academy of Sciences of the USA 83(15): 5713-5717.
-
Tauber PF, Zaneveld LJ, Propping D, Schumacher GF (1975) Components of human split ejaculates. I. Spermatozoa, fructose, immunoglobulins, albumin, lactoferrin, transferrin and other plasma proteins. J Reproduction Fertility 43(2): 249-267.
-
Castle PE, Whaley KJ, Hoen TE, Moench TR, Cone RA (1997) Contraceptive effect of sperm-agglutinating monoclonal antibodies in rabbits. Biology Reproduction 56(1): 153-159.
-
Kirkpatrick JF, Turner A (2002) Reversibility of action and safety during pregnancy of immunization against porcine zona pellucida in wild mares (Equus caballus). Reprod S60: 197-202.
-
Kirkpatrick JF, Turner A (2003) Absence of effects from immunocontraception on seasonal birth patterns and foal survival among barrier island wild horses. J Appl Anim Welf Sci 6(4): 301-308.
-
Curtis PD, Richmond ME, Miller LA, Quimby FW (2007) Pathophysiology of white-tailed deer vaccinated with porcine zona pellucida immunocontraceptive. Vaccine 25(23): 4623-4630.
-
Singh M, Das SK, Suri S, Singh O, Talwar GP (1998) Regain of fertility and normality of progeny born during below protective threshold antibody titers in women immunized with the HSD-hCG vaccine. Am J Reprod Immunol 39: 395-408.
-
Naz RK (2011) Contraceptive vaccines: success, status, and future perspective. American J Reprod Immunol 66(1): 2-4.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future