Re-purposing Drugs and Prominent Vaccines Efficacy against Covid-19: A Short Review
Coronavirus disease 2019 (COVID-19 or SARS-CoV-2) a newly outbreak of respiratory infection firstly reported in December 2019, in Wuhan, China has not only affected healthcare worldwide but also created global economic disruptions. As of now, more than 120 million cases have been reported with 2.6 million confirmed deaths so far as of mid-March 2021. With having high availability of transmission rate within the few months, it quickly speeded all across the globe. Although with the modern technologies in scientific research we are now in a better position to understanding and cope with this outbreak. Recently vaccine candidates like Pfizer/Biotech and Moderna received emergency approval from US FDA based on their clinical safety showed around 95 % efficacy profile in preventing infection. However, to vaccinate the majority of populations all around the globe in a limited time is extremely challenging especially in under developing countries. Here some of the repurposing drugs could be an alternative approach to reduce the mortality rate based on in vitro or in vivo studies. Additionally, numerous chemical drugs are also to be prescribed are underway based on the computational tools. In this mini-review, we have speculated some of the repurposing drugs against SARS-CoV-2 infection whether its effective or not, their life cycle mechanism, and some prominent vaccine efficacy.
Introduction
An unexpected outbreak emerged as the new pandemic in the 20th century threatening the entire world named novel coronavirus 2019 later on 11 Feb 2020 by the International Committee on Taxonomy of Viruses (ICTV) named Coronavirus disease as SARS-CoV-2 causing serious lungs disease ranging from the mild common cold to more severe pneumonia. The virus was first originated in the local South Seafood market of Wuhan city, China, when a bunch of cases of pneumonia was reported in late December 2019. Later this virus was identified as Zoonotic (Bat Virus), which has transmitted from the bat population to the human called to be the SARS- CoV-2 zoonotic origins—related to the closely associated like siblings with the same associated coronaviridae family (Middle East Respiratory Syndrome (MERS-CoV) in 2012 & Severe Acute Respiratory Syndrome-1 (SARS-CoV) in 2003
[1]. However, the rate of mortality is very much higher in SARS CoV-2 as compare to the earlier epidemical outbreaks. Due to human transmission in the community, the symptoms have been varying from acute to severe pneumonia depending on the patient’s condition across the population and region. However, the clinical presentation of confirmed cases could be heterogeneous: almost 80% of confirmed cases with mild pneumonia, 15% comprised with critical pneumonia with shortness of breathing, and 5% evolved critical ill reported with respiratory failure, with multiple vital organ failure resulting in death [1]. Notably, several clinical manifestations reported with an increase in the level of C-reactive protein, aspartate aminotransferase enzyme, creatine kinase were more often in severely infected patients with COVID-19 as a comparison to mildly infected patients [2]. Causing the large pro-inflammatory event of cytokine storm in severely ill patients, resulting in the high number of mortalities recorded in COVID-19. These coronaviruses belong to the large and enveloped spike (S) glycoprotein structure containing a single strand of positive-sense RNA (with the genomic length of 26- 32 kb) that can efficiently use human angiotensin-converting enzyme (ACE2) receptor for viral insertion inside the host cells and then endocytosed [3]. Although it’s genetically more identical to the previous outbreak SARS-CoV-1 than to MERS-CoV with 80% shared nucleotide homology [3]. These viruses target the pulmonary epithelial cells of the lower windpipe of the respiratory tract rich in ACE2 receptors, further transporting their nucleocapsid and highjacks the host cell machinery process to multiply inside the cytoplasm making viral copies by damaging the vital organs having ACE2 receptors available at various organs locations like the gastrointestinal tract (GI), kidney, liver and the heart [4].
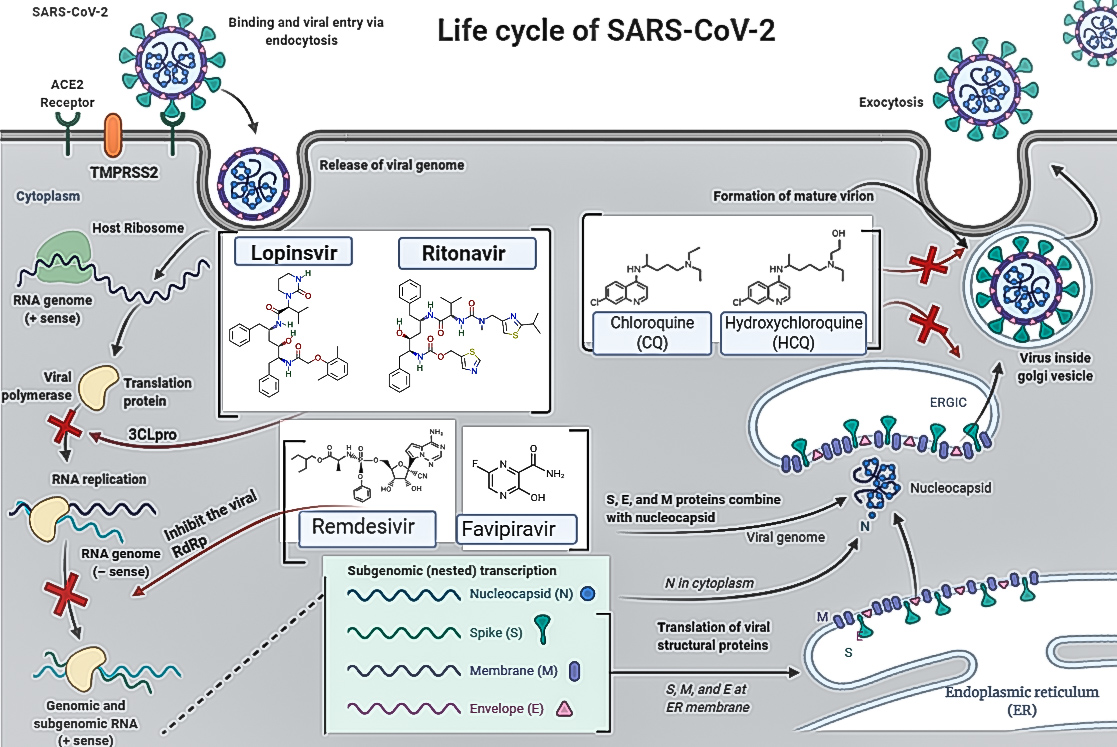
The SARS-CoV-2 involves six different steps to complete its viral life cycle: viral entering inside the host cell, replication machinery of protein, RNA-dependent RNA polymerase (RdRp) for replication, structural proteins translation with the help of ribosome, virion assembly for genomic RNA, and release of virions through cell membrane [4]. The virus attaches itself strongly to a specific ACE2 receptor present on the cell membrane of the host. Further after the attachment, the type II transmembrane serine protease 2 (TMPRSS2) receptor on the host cell surface helps the ACE2 & activate the receptor by attaching to spike (S) proteins, following the activation of spike (S) protein it prompts a conformational change and allows the virus to enters inside the host cell [5] Both the protein receptors ACE2 and TMPRSS2 plays a significant role in the insertion of the virus inside the host cell [5]. Currently, some of the re-purposing antiviral drugs inhibit the translation step of the RNA-dependent RNA polymerase (RdRp) enzyme-like Remdesivir/ favipiravir, HIV protease inhibitor (PI) drugs Lopinavir/Ritonavir, and Ivermectin and dexamethasone are prescribing for emergency medical use against the viral infection. Meanwhile, vaccines like Pfizer- BioNTech and Moderna (both ~ 95 % efficacy rate) have also started inoculation in many countries presently after receiving emergency approval from US FDA. Besides, two versions of the AstraZeneca/Oxford vaccine also received emergency use approval (EUA) from WHO against covid-19. Here, in this review, we present a systematic overview of the pharmacodynamics of some re-purposing drugs considering that it could be an alternate avenue for the poorest and most vulnerable people until the vaccine is available to everyone.
Drugs, Inhibiting the RNA-Dependent RNA Polymerase
Remdesivir Drug
Remdesivir (GS-5734), a nucleoside analog prodrug, was developed by Gilead (USA) against the Ebola virus. It has broad antiviral properties against RNA virus families like filoviridae, Paramyxoviridae, Filoviridae, and Coronaviridae [6]. The intravenous infusion of triphosphate form of RDV (RDV-TP) of GS-5734 (10 mg /kg) on non-human primates has shown enormous suppression of viral replication resulted in almost 100% protection against the Ebola virus [7]. Based on the pre-clinical study in vitro & Vivo data of this drug, it was found that remdesivir with its dynamic property can inhibit the (RdRp) enzyme by terminating the viral RNA synthesis of SARS CoV-2 by competing with the traditional counterpart of adenosine-triphosphate (ATP) (Figure, 1) (Table, 1) [7, 8, 9]. As the (RdRp) enzyme incorporates one, two, three more nucleotides, the few additional involved nucleotides simple moves back, while the rest prodrug reaches the third location away from the enzyme’s proactive site further collides with a specific amino acid, a serine (Ser) in the active position of the enzyme and prevents the enzyme for moving ahead to combined at the next nucleotide [8, 9, 10]. Although, 3’to 5’ exoribonuclease ExoN (proofreading) of the SARS-2 virus is susceptible to remdesivir drug but they can resist themself against the proactive form of remdesivir [9, 10]. It is essential to acknowledge that the current SARS-CoV-2 infection shares almost 80% RNA sequence homology with the previous SARS-CoV-1 and some enzymes like (RdRp) also share ~ 96% sequential similarities [9]. According to The New England Journal of Medicine a study done on a 35-year-old person with COVID-19 infection in the United States (first case in the US) who traveled from the province of China, Wuhan, was cured with intravenous (IV) remdesivir started on day 7 of hospitalization, with no adverse effect reported with the infusion [11]. Later the U.S FDA permitted the emergency use approval (EUA) use of Remdesivir for treating the confirmed Covid-19 patients in hospitalized via intravenous (IV) infusion including pediatric patients [12]. However, this drug is in clinical evaluation in many countries like the USA, France, and Canada (NCT044131453) (NCT04365725).
Favipiravir
Favipiravir (T-705) an effective antiviral drug permitted for treating the influenza virus, developed by Toyama Chemical (Fujifilm group, Japan). A potent inhibitory drug targets the (RdRp) enzyme of the RNA viruses (Figure 1) [13]. These prodrugs incorporated inside the cell & became active intra-cellularly by phosphoribosylation metabolic process into its proactive form (favipiravir-ribofuranosyl-5- triphosphate), these molecule acts as a substrate for (RdRp) replicase enzyme, which misguided by the enzyme as a purine nucleotide further interrupting its activity by terminating the viral protein synthesis [14, 15]. However, the mode of the action of favipiravir-RTP with the RdRp replicase enzyme has not been completely understood [13]. It was theorized that favipiravir may be mis-incorporated into an emerging viral RNA, or it could act by binding to conserved polymerase domains, thus preventing incorporation of nucleotides for viral RNA replication and transcription [13]. In recent, it was discovered that the SARS-CoV-2 RdRp enzyme complex is at least 10-fold more active than any additional viral RdRp known [15, 16]. Unlike the RNA viruses, humans do not have an RdRp enzyme yet have DNA dependent RNA-polymerase (DdRp) and DNA dependent DNA-polymerase, favipiravir act by hindering this viral RdRp polymerase enzyme, permitting the simple addition of favipiravir molecules into viral RNA while leaving the human DNA apart [13]. This presumed shows that nucleotide analogs are promising against theSARS-CoV-2 [13, 15]. Favipiravir was previously utilized against SARS-CoV-2 infection in Wuhan, China & in March 2020, later got approved by the Chinese Medical Administration as the first drug against SARS-CoV-2. As the pandemic spread all across the continents of Europe, the middle east, and Asia, this drug received emergency approval in many countries to be used in mild symptomatic to moderate COVID-19 patients [15, 17]. Currently, this drug is in clinical evaluation (NCT04359615) (NCT04411433).
Protease Inhibitory Drugs (Blocking Virus- Cell Membrane Fusion)
Hydroxychloroquine-HCQ & Chloroquine
Chloroquine & Hydroxy analog (Hydroxychloroquine- HCQ) uses as an antimalarial drug with anti-inflammatory properties (suppressing TNFα & IL-6) blocks the virus entry inside the target cell by raising the pH of the endosomal region and lysosome changing the protein degradation pathway in the endocytic pathway (Figure 1) (Table 1) [18]. Centre for Disease Control and Prevention (CDC) reported effective anti-SARS coronavirus effects of chloroquine in vitro, shows that glycosylation inhibition process may be the key machinery for the anti-viral effect of chloroquine [19]. Although both of these chemical drugs are hypothetically similar in their antiviral activity, efficient in inhibiting the angiotensin-converting enzyme2 (ACE2) glycosylation, in the endosome of the host cell preventing the cytokine storm, moreover HCQ, a less harmful aminoquinoline, has an N-hydroxyethyl side chain at the location of the N-diethyl group of chloroquine, this confirmational adjustment makes HCQ more soluble property in comparison to chloroquine against SARS CoV-2 [20, 21]. Apart from the general safety consideration, some psychiatric & neurological side effects have been reported during the initial days of the treatment and further got improved after the end of treatment [22]. The Lancet study collected data between the 10,700 patients receiving HCQ, and 21,400 patients not receiving HCQ found no significant differences reported against active SARS- CoV-2 [23]. These controversies led the U.S FDA to withdraw the emergency usage of HCQ and chloroquine against SARS- CoV-2 infection due to some serious heart rhythm and other organ failures reported [24].
| Drug Name | Mode of action | Current use | Ref | |
|---|---|---|---|---|
| 1 | Remdesivir | Interferes with viral RNA polymerase | Ebola | [6-8] |
| 1 | Remdesivir | Interferes with viral RNA polymerase | (FDA approved for COVID-19) | [6-8] |
| 2 | Favipiravir | Interferes with viral RNA polymerase | Influenza | [13-17] |
| 3 | Chloroquine/Hydroxychloroquine (HCQ) | Blocking Virus-Cell Membrane Fusion | Antimalarial | [18,19] |
| 3 | Chloroquine/Hydroxychloroquine (HCQ) | Blocking Virus-Cell Membrane Fusion | (Halted by WHO) | [18,19] |
| 4 | Ivermectin | Inhibiting the Viral Protease | Anti-parasitic agent | [25,26] |
| 5 | Lopinavir/Ritonavir | Inhibiting the Viral Protease | HIV | [17,28] |
Table 1: Drugs approved for the trial on SARS-CoV-2 patients.
Inhibiting the Viral Protease
Ivermectin
Ivermectin, an FDA-approved drug with antiparasitic properties, recently, in a study demonstration shown broad anti-viral property in vitro studies, an inhibitor of the contributory infection SARS-CoV-2, with reduced the effect of SARS-CoV-2 viral RNA up to ~5000 overlays after 48 hrs [25]. The mode of action of ivermectin inhibits the host cell importin α or β transporter-mediated protein, decreasing the translocation of viral SARS-2 nucleocapsid protein (NCP) the cytoplasm to the nucleus core, altered NCP distribution disrupts viral spreading & persistence (Figure 1) (Table 1) [26]. Based on the efficacy demonstrated in vitro studies, it can be said theoretically that ivermectin may prove to be beneficial to the Covid-19 patients can be assumed [27]. Currently, this drug is in clinical evaluation (NCT04391127), (NCT04435587), and in recent the WHO advises for ivermectin drug only to be used to treat covid-19 patients within clinical trial until more data is available.
Dexamethasone
An affordable, regularly used as corticosteroid, dexamethasone has now become the potentially life-saving medication to diminish the death rate in infected Covid-19 patients which are requiring oxygen or ventilator support, proved by the primary clinical trial led all across the region of United Kingdom (UK) patients shown promising results [31]. Due to its wide range of anti-inflammatory and immunosuppressant effects (WHO), a very low-cost steroid decreases the level of IL-6 (Interleukin-6) & TNF-α (tumor necrosis factor-alpha) causing cytokine storm in critically Covid-19 infected patients with no side effect. According to the recently published data, over 2100 patients were appointed to get low dose dexamethasone treatment, and over 4300 patients to get receive regular treatment, found that in the dexamethasone group, the occurrence of death was lower than that in the regular care group among patients receiving invasive mechanical ventilation resulted (29-41%) low dead as compared among those patients receiving oxygen without invasive mechanical ventilation (23-26%) of low mortality [32]. However, there was no evidence that dexamethasone gave any advantage among those Covid-19 patients who were not getting help at randomization [32]. Shortly after the outcome, it is now prescribing worldwide for those COVID-19 patients who required oxygen, including those on ventilators with intensive care.
Vaccines Candidates
To encounter the pandemic outburst vaccines could be a reliable method to cope with the current situation. Many of the vaccines are underway (Phase III trial) to provide long- term immunity against SARS-CoV-2 with better effectiveness, safety, and efficacy profile. With the genomic sequencing of the SARS-CoV-2 available in early January 2020, multiple vaccine candidates had launched their trials to developed vaccines at an unprecedented speed [33]. As per as WHO draft landscape, almost 174 Covid-19 vaccine candidates are in diffe rent steps of preclinical stages and 63 clinical are in advanced evaluation on humans are underway [34] (Table 2).
| Type of Vaccine | Developer/Founder | Clinical trial (ongoing) | Efficacy in % | Ref | |
|---|---|---|---|---|---|
| Pfizer-BioNTech | BNT-162b1 (RNA) | Pfizer & BioNTech | NCT04713553 III NCT04368728 II/III | 95% | [35] |
| Moderna | Encapsulated mRNA-1273 | NIAID & Moderna | NCT04470427 III | 94.10% | [36] |
| Oxford-AstraZeneca | AZD-1222 ChAdOx1-5 (non-replicating AdV) | University of Oxford/AstraZeneca | NCT04516746 III NCT04540393 III NCT04536051 III | Efficacies from two groups- 90 % & 62.1% Overall: 70.4% | [37] |
| Sputnik V | Adeno based (rAd26+rAd5) virus | Gamaleya Research Institute of Epidemiology and Microbiology, Russia | NCT04530396 III NCT04564716 III NCT04642339 III NCT04656613 III | 91.40% | [38] |
| Novavax | NVXCoV2373 (protein-based) | Novavax (USA) | NCT04611802 III NCT04583995 III | 89.3 % (recent in UK clinical trial) | [39] |
| Johnson & Johnson (J&J) | Ad26.COV2. S | Janssen Pharmaceutica, a division of Johnson & Johnson (J&J), Belgium | NCT04505722 III | (66 %) efficacy in a single shot (data is yet to published) |
Table 2: Some prominent vaccine candidates for Covid-19 with efficacy profile.
Importantly, some of the vaccine candidates have already been launched after receiving emergency approval based on their excellent clinical efficacy in the Phase III safety clinical trials. In late December the Pfizer-BioNTech became the first approved vaccine from US FDA followed by the Moderna mRNA1273 showed around (~95 %) efficacy profile, and already started vaccination in the USA [35, 40]. Recent a new vaccine from Johnson & Johnson (J&J) also received FDA authorization. However, the complete data is yet to be published. Importantly the J&J vaccine report to delivered (66 %) efficacy in a single shot to moderate and severe covid-19 patients in multi-countries. Several others candidates have also started their inoculating programs in many countries, vaccines like ChAdOx1-nCoV-19 by AstraZeneca/ Oxford (overall 70.4% efficacy), Sputnik -V from Gamaleya Research Institute Moscow Russia (91.4 %), NVX-CoV2373 vaccine from Novavax (89.3% efficacy in UK trial) these vaccines will be administrated into two shots the standard dose on Day 0 and booster regimen after 21/28 days apart. Suggested to provide better neutralizing antibodies for long-term protection. However, at this moment it’s hard to predict which vaccine might be the best for longer-lasting protection but we believe it will depend on the infection severity.
Conclusion Remark
In this review, we have tried to summarise some of the re-purposing drugs and the efficacy rate of several prominent vaccine candidates. As the third zoonotic outbreak which is associated with the similar coronaviridae familial like SARS-CoV-1 and MERS-CoV previously outbreaks disease has not just affected the worldwide but also disrupted the global supply chain which led to the global economic crisis and raised a big question on the public health care system worldwide. However, at the time of writing many countries have again announced for their lockdown as the second wave of covid-19 has emerged and causing a wide surge of infection again. Till now over 219 countries and territories have reported this virus so far as per a WHO report. We believe that repurposing drugs like antiviral drugs could remain an alternative approach against SARS-CoV-2 in the current scenario especially for the low-income countries because the availability of covid-19 vaccine supply will still take a lot of time in these countries. Drugs like remdesivir have already in public used after getting emergency authorization from US FDA. Dexamethasone also a potential lifesaving corticosteroid drug is prescribing in many countries to diminish the death rate in covid- 19 patients on a ventilator. Hydroxychloroquine drug has been halted by WHO due to some adverse reaction reported and later found very unlikely to be beneficial. Recently the WHO advises for ivermectin drug only to be used to treat covid-19 patients within clinical trial until more data is available. Other than that, numerous pharmacological drugs are already registered globally and many are in pipelines based on computational tools. As per as covid-19 NMA initiative (https://www.covid-nma.com/ dataviz/) around 2818 studies of treatments are underway worldwide.
On another side, the good news is several vaccines candidates had started rolled out in less than a year which is a remarkable achievement in medical sciences, two mRNA vaccines like Pfizer/BioNTech and Moderna with an efficacy rate of around (~95 %) received emergency US FDA approval in the US, and in European Union (EU) and other countries too. Later Johnson &Johnson (J&J) vaccine also followed in the row and became the third emergency approved vaccine from US FDA emergency use in the USA, EU, and other countries too. Additionally, a vaccine from Oxford/AstraZeneca with an overall 70.4% efficacy profile has also started its inoculation programme after receiving emergency regulatory approval in many different countries. One more challenge for these vaccine candidates is the rise of the new contagious emerging strain of mutated SARS-CoV-2 virus-like (South African variants B.1.351), (United Kingdom variants B.1.1.7). Despite all these challenges we believe that upcoming vaccines will come up with better therapeutics and common effective treatments in the future.
Competing Interests
The author declared no competing of interest.
Funding
Not Applicable
Authors Contribution
Satyendra Prakash contributed in writing drawing the figure and table in this review article. Sachchida Nand Rai and Sushil Dubey designed the content of the article. M.P Singh drafted and reviewed the manuscript.
Acknowledgment
Satyendra Prakash is thankful to the Department of Biotechnology (DBT) New Delhi for providing facilities in the Centre of Biotechnology, University of Allahabad, Prayagraj, India.
References
-
Pennica A, Conforti G, Falangone F, Martocchia M, Tafaro T, et al. (2020) Clinical Management of Adult Coronavirus Infection Disease 2019 (COVID-19) Positive in the Setting of Low and Medium Intensity of Care: A Short Practical Review. SN Compr Clin Med, pp: 1-6.
-
Hossen MS, Barek MA, Jahan N, Safiqul IM (2020) A Review on Current Repurposing Drugs for the Treatment of COVID-19: Reality and Challenges. SN Compr Clin Med pp: 1-13.
-
Yi Y, Lagniton PNP, Ye S, Li E, Xu RH (2020) COVID-19: what has been learned and to be learned about the novel coronavirus disease. Int J Biol Sci 16(10): 1753-1766.
-
Hushmandi K, Bokaie S, Hashemi M, Moghadam ER, Raei M, et al. (2020) A review of medications used to control and improve the signs and symptoms of COVID-19 patients. Eur J Pharmacol 887: 173568.
-
Astuti I, Ysrafil (2020) Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): An overview of viral structure and host response. Diabetes MetabSyndr 14(4): 407-412.
-
Lo MK, Jordan R, Arvey A, Sudhamsu J, Shrivastava- Ranjan P, et al. (2017) GS-5734 and its parent nucleoside analog inhibit Filo-, Pneumo and Paramyxoviruses. Sci Rep 7: 43395.
-
Warren TK, Jordan R, Lo MK, Ray AS, Mackman RL, et al. (2016) Therapeutic efficacy of the small molecule GS-5734 against Ebola virus in rhesus monkeys. Nature 531: 381-385.
-
Brown AJ, Won JJ, Graham RL, Kenneth HD, Amy CS, et al. (2019) Broad spectrum antiviral remdesivir inhibits human endemic and zoonotic delta coronaviruses with a highly divergent RNA dependent RNA polymerase. Antiviral Res 169: 104541.
-
Hashemian SM, Farhadi T, Velayati AA (2020) A Review on Remdesivir: A Possible Promising Agent for the Treatment of COVID-19. Drug Des Devel Ther 14: 3215- 3222.
-
Laurel Oldach (2020) A mechanism for remdesivir activity and a platform to test other antivirals.
-
Holshue ML, DeBolt C, Lindquist S, Kathy HL, John W, et al. (2020) First Case of 2019 Novel Coronavirus in the United States. N Engl J Med 382(10): 929-936.
-
Veklury (2020) Fact Sheet for Healthcare Providers Emergency Use Authorization (Eua) of Veklury ® (Remdesivir) for Hospitalized Pediatric Patients Weighing 3.5 Kg to Less Than 40 Kg or Hospitalized Pediatric Patients Less Than 12 Years of Age Weighing at Least 3.5 Kg.
-
Furuta Y, Komeno T, Nakamura T (2017) Favipiravir (T-705), a broad-spectrum inhibitor of viral RNA polymerase. Proc Jpn Acad Ser B Phys Biol Sci 93(7): 449-463.
-
Smee DF, Hurst BL, Egawa H, Takahashi K, Kadota T, et al. (2009) Intracellular metabolism of favipiravir (T-705) in uninfected and influenza A (H5N1) virus-infected cells. J Antimicrob Chemother 64(4): 741-746.
-
Agrawal U, Raju R, Udwadia ZF (2020) Favipiravir: A new and emerging antiviral option in COVID-19. Med J Armed Forces India 76(4): 370-376.
-
Shannon A, Selisko B, Le N, Piorkowski G, Fattorini V, et al. (2020) Favipiravir strikes the SARS-CoV-2 at its Achilles heel, the RNA polymerase. Preprint bio Rxiv.
-
Tu YF, Chien CS, Yarmishyn AA, Yi-Ying L, Yung-Hung L, et al. (2020) A Review of SARS-CoV-2 and the Ongoing Clinical Trials. Int J Mol Sci 21(7): 2657.
-
Savarino A, Boelaert JR, Cassone A, Majori G, Cauda R (2003) Effects of chloroquine on viral infections: an old drug against today’s diseases? Lancet Infect Dis 3(11): 722-727.
-
Savarino A, Di Trani L, Donatelli I, Cauda R, Cassone A (2006) New insights into the antiviral effects of chloroquine. Lancet Infect Dis 6(2): 67-69.
-
Beura S, Chetti P (2020) In-silico strategies for probing chloroquine-based inhibitors against SARS-CoV-2. J Biomol Struct Dyn, pp: 1-13.
-
Satarker S, Ahuja T, Banerjee M, Vignesh BE, Shagun D, et al. (2020) Hydroxychloroquine in COVID-19: Potential Mechanism of Action Against SARS- CoV-2. CurrPharmacol Rep, pp: 1-9.
-
Gevers S, Kwa MSG, Wijnans E, van Nieuwkoop C (2020) Safety considerations for chloroquine and hydroxychloroquine in the treatment of COVID-19. Clin Microbiol Infect 26(9): 1276-1277.
-
Gentry CA, Humphrey MB, Thind SK, Hendrickson SC, Kurdgelashvili G, et al. (2020) Long-term hydroxychloroquine use in patients with rheumatic conditions and development of SARS-CoV-2 infection: a retrospective cohort study. Lancet Rheumatol 2(11): E689-E697.
-
FDA (2020) FDA cautions use of hydroxychloroquine/ chloroquine for COVID-19. US Food and Drug Administration.
-
Caly L, Druce JD, Catton MG, Jans DA, Wagstaff KM (2020) The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Antiviral Res 178: 104787.
-
Vora A, Arora VK, Behera D, Tripathy SK (2020) White paper on Ivermectin as a potential therapy for COVID-19. Indian J Tuberc 67(3): 448-451.
-
Gupta D, Sahoo AK, Singh A (2020) Ivermectin: potential candidate for the treatment of Covid 19. Braz J Infect Dis 24(4): 369-371.
-
Chandwani A, Shuter J (2008) Lopinavir/ritonavir in the treatment of HIV-1 infection: a review. Ther Clin Risk Manag 4(5): 1023-1033.
-
Li H, Yang L, Liu FF, Xin-na M, Pei-lan H, et al. (2020) Overview of therapeutic drug research for COVID-19 in China. Acta Pharmacol Sin 41: 1133-1140.
-
Cao B, Wang Y, Wen D, Liu W, Wang J, et al. (2020) A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe Covid-19. N Engl J Med 382(19): 1787-1799.
-
Dexamethasone (2020) Dexamethasone: the first drug to improve survival in Covid-19.
-
Recovery Collaborative Group (2020) Horby P, Lim WS, et al. Dexamethasone in Hospitalized Patients with Covid- 19-Preliminary Report. N Engl J Med 384(8): 693-704.
-
Tu YF, Chien CS, Yarmishyn AA, Yi-Ying L, Yung-Hung L, et al. (2020) A Review of SARS-CoV-2 and the Ongoing Clinical Trials. Int J Mol Sci 21(7): 2657.
-
WHO Team (2021) Draft landscape and tracker of COVID-19 candidate vaccines.
-
Hossain MS, Hami I, Sawrav MSS, Md Fazley R, Otun S, et al. (2020) Drug Repurposing for Prevention and Treatment of COVID-19: A Clinical Landscape. Discoveries (Craiova) 8(4): e121.
-
Polack FP, Thomas SJ, Kitchin N, Judith A, Alejandra G, et al. (2020) Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N Engl J Med 383(27): 2603-2615.
-
Knoll MD, Wonodi C (2021) Oxford-AstraZeneca COVID-19 vaccine efficacy. Lancet 397(10269): 72-74.
-
Logunov D, Dolzhikova I, Shcheblyakov D, Amir IT, Olga VZ, et al. (2021) Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: an interim analysis of a randomised controlled phase 3 trial in Russia. The Lancet 397(10275): 671-681.
-
MVEC (2021) Novavax COVID-19 Vaccine Demonstrates 89.3% Efficacy in UK Phase 3 Trial Novavax Inc-IR Site. Novavax Inc-IR Site.
-
ChilamakuriR, Agarwal S (2021) COVID-19: Characteristics and Therapeutics.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future