Heterologus Covid-19 Vaccines Using Alternate Vaccine Modalities as Immune Booster to Overcome the Social Challenges and Problems in the Covid-19 Pandemic
The coronavirus disease 2019 (Covid-19) pandemic represents a massive impact on human health, causing sudden lifestyle changes, through social distancing and isolation at home, with social and economic consequences. Optimizing public health during this pandemic requires not only knowledge from the medical and biological sciences, but also of all human sciences related to lifestyle, social and bhavioral studies, including dietary habits and lifestyle. Our strongest and only weapon to protect from the Covid-19 pandemic is Covid -19 vaccines. We need to have “Herd Immunity” by only the vaccination to get rid of the Covid-19 pandemic in the whole world. To get Covid-19 vaccines is a “social responsibility” for all humanity and to be healthy.
Introduction
The Covid-19 outbreak has affected populations across the world. In a short time, we were exposed to a critical situation, faced with numerous medical, social, and economic challenges. The Covid-19 pandemic has severe health effects and serious implications for economic growth and social development. Quarantines and physical distancing measures, which are needed to stop the rapid spread of the coronavirus and save lives, are leading to job losses. Many international borders were closed, which limited the supply of goods, including food. In some areas, food supply chains were completely broken or drastically changed with food business operators needing to adopt new business models, e.g. suppliers reorienting themselves to new markets, increases in the need for delivery. Supplying food also presents possible risks for infection, both environmentally (i.e. in food stores) or through contaminated foods/packaging. Increased demand for certain products may result in the inability to maintain levels of supply [1, 2]. In most countries, the segmentation of health services, the concentration of human resources and medical technology in some urban hospitals, the under- financing of primary health care and epidemiological surveillance, and the lack of coordination between the different levels of care weaken the coordination of national response actions. Maintaining essential health services for women, children, and adolescents while mitigating the pandemic’s impact represents an unprecedented challenge. The pandemic and its response make it challenging to reach or sustain these targets, even though the region was well on track to achieve them. Urgent priorities oriented towards achieving women, children, and adolescent health equity during and after the pandemic require to increase public spending on health and social policies to control the pandemic and to favor social and economic reactivation and reconstruction, restore and rebuild essential health services, and strengthen the primary health care strategy. These are a few instances most of us can relate to in this world of the ‘new normal. The lockdown intensified the number of those who became frustrated and depressed. There is an upsurge in social issues, including psychological disorders, domestic violence, suicides, etc. And children are getting depressed as well [1, 2, 3]. While the medical community has focused on developing successful diagnostic and medical treatments, many countries have introduced far-reaching restrictions on daily life to prevent and control the spread of the virus. In many cases, this resulted in a complete shut-down of whole cities, regions, and even countries. The resulting changes to working patterns and living circumstances have had a large impact on the supply, purchase, preparation, and consumption of food [1, 2, 3, 4].
The covid-19 pandemic is the largest health problem worldwide. Unfortunately, the lack of an effective and clear treatment causes it to be a major health problem. There are currently no effective antiviral drugs and treatments. The symptoms and course of the disease differ individually. Symptoms vary from asymptomatic to intensive care even death. The individual variation of this symptom pattern is related to viral load, individual’s current comorbid conditions, age, gender, and most importantly, immune status. Considering the course differences of the disease in all these individual, familial and demographic distributions, it suggests that genetic and environmental factors play an important role [3, 4, 5].
The immune response plays important role in SARS- COV-2 infection and vaccination and to understand the immune response in both conditions one must understand the normal immune response. The immune system is the defense system of the body that protects against pathogenic organisms like bacteria, viruses, fungi, cancer through cells and antibodies. The immune system is divided into two components i.e innate immunity and adaptive immunity. Innate immunity is immediate and nonspecific while adaptive immunity is delayed and takes a few days to develop and is specific [6, 7, 8].
Covid-19 vaccines, those that have been approved and the ones still in development, use various methods and mechanisms to boost immunity. AstraZeneca’s adenovirus vaccine uses a weakened version of a common cold virus found in chimpanzees to present the spike protein to the immune system, while Pfizer’s mRNA-based vaccine delivers genetic instructions for making the spike protein and encourages human cells to produce it [6, 7, 8, 9, 10].
Heterologous immunization with Covid-19 vaccines may induce a superior immune response. There are 5 different platforms for Covid-19 vaccines and about 16 different vaccines developed. All these vaccines induce an immune response, some have a better humoral response and lesser cellular response while others have better cellular response than the humoral response [8, 9, 10, 11, 12, 13]. Our concerns about this issue; there are SARS-CoV2 variants and some vaccines have reduced efficacy against infection due to these variants. Secondly the strength and the type of the immune response. Thirdly length of the time that humoral response lasts and when one has to take the booster. To address the above concerns we recommend having heterologous vaccination with two different types of vaccines and there is a strong possibility that the above concerns can be addressed. For this, we have selected mRNA (Pfizer) and Inactivated Virus (Sinopharm) vaccines. There are several animal studies where immune response with heterologous vaccines was much stronger and lasting as compared to single vaccines but no human study. We strongly believe that with heterologous vaccines there will be a much stronger and longer-lasting immune response and maybe more effective against the variants. This paper has based on an observational study but shows some strong signals into potentiation of the immune system with both vaccines and has objective data that will need a study ideally randomized study to apply results to the population at large. There is a systemic inflammatory response in COVID-19. High levels of chemokine and proinflammatory cytokines are detected in patients. With the booster of the immune system via the vaccination, people can be protected from COVID-19 and make the process easy when suffering from a disease. Therefore, vaccination is one of the most important factors to be healthy and to have a normal life in society.
Covid-19 Vaccines
There are five different platforms for Covid-19 vaccines and about 16 different vaccines developed. All these vaccines train the immune system to recognize the virus differently and lead to developing more strong and durable immune response.
The platforms and vaccines in each platform are as follows: 1-RNA based vaccine eg Pfizer, Moderna, CureVac G 2-Viral Vector (adenovirus-non-replicating) eg AstraZeneca, CanSino, Sputnik, Janssen 3-Inactivated Virus eg Sinopharm, Sinovac, etc. 4-Protein subsunit eg Novavax 5-DNA based Vaccine eg Zydus Cadila All of the Covid-19 vaccines are widely available, except for Johnson & Johnson’s (J&J need a single dose) require two doses. The first dose primes the immune system and the second dose is administered usually on the 21st day after the first dose which boosts it [14, 15].
Homologous Prime Boost Vaccination
All of the Covid-19 vaccines are widely available and usually need 2 doses about 21 days apart. The first dose primes the immune system and the second dose is given 21- 28 days apart, boosts it. Using the same vaccine preparation for the first and 2nd dose is called homologous prime-boost [16].
Heterologous Prime-Boost Vaccination or Mixing and Matching Covid-19 Vaccination
There is an interesting example of mixing-and-matching as wearing office attire on top (coat, matching tie, waistcoat) and pajama pants on bottom. This is on the lighter note and here are the following types of Immunoboost strategies for the Covid-19 Vaccination schedules.
In some countries, there may be a shortage of vaccines after the first dose of the vaccine, and people can’t have the 2nd dose of the same vaccine after 21 days. If the 2nd dose of the same vaccine is given it is called homologous vaccination. Public Health Department England after the 2nd dose of the vaccines was delayed for up to 12 weeks suggested that these people can have the 2nd dose of some different platform vaccine to have some protection. This has to lead the scientists of different countries to have projects of mixing and matching the different covid vaccines. Using different vaccine preparations is called heterologous prime-boost. For example; the first dose of AstroZanca Covid dose is given and then after 21 days instead of the AstraZanca Covid vaccine we give a shot of Pfizer Vaccine and this is Heterogenous Boost Vaccination [16].
Enhanced Heterologous Immunoboost Vaccination (The corresponding author’s suggestion)
We recommend that one should get 1st dose of one type of Covid Vaccine and then after 21 days should get the 2nd Dose of the same vaccine (eg platform 3). Then one should get 2nd Vaccine from a different Covid Vaccine platform eg dose 1 and then a dose 21 days after the 1st dose from platform 1. Natural Immunity and Vaccine-Induced Immunity are different since immunity after the infection (natural) is mainly affected by the immune-evasion strategies of the virus which is considered in developing the vaccines [14, 15, 16].
Results
Record of COVID-19 Enhanced Heterologous Immuno- Boost (EHIB) Vaccination along with antibodies tests (since no study has been done till now so the corresponding author volunteered for this study, had EHIBV and post-vaccination antibodies tests with his serum):
- Initially, the author was COVID-19 negative as per the PCR test.
- Initially, COVID-19 negative as per the PCR test.
- Anti-spike antibodies test (post-vaccination antibodies Test) was done on 24/02/2021 and was NEGATIVE (<0.40U/mL).
- 1st dose of Sinopharm 6/3/2021
- Sinopharm Vaccination 2nd Dose on 27/03/2021.
- Anti-spike antibodies test (post-vaccination antibodies Test) done on 27/03/2021 and titer was 3.93U/mL mild increase in 21 days after the 1st dose of Sinopharm.
- Pfizer Vaccine 1st dose on 24/3/2021.
- Pfizer 2nd dose on 14/04/2021 which is exactly 21 days after the first dose of the Pfizer Vaccine
- Anti-spike antibodies test (post-vaccination antibodies Test) done on 10/04/2021 (35 days after 1st dose of Sinopharm), titer was 682.00U/mL, 14 days after 2nd dose of Sinopharm vaccine and 17 days after 1st dose of Pfizer Vaccine.
- Anti-spike antibodies test (post-vaccination antibodies Test) done on 27/04/2021(52 days after 1st dose of Sinopharm vaccine), titer was 2500.00U/mL, 27 days after 2nd dose of Sinopharm vaccine and 13 days after 2nd dose of Pfizer Vaccine.
- Anti-spike antibodies test (post-vaccination antibodies Test) done on 27/05/2021(82 days after 1st dose of Sinopharm Vaccine). Titer was 4764 U/mL, 57 days after 2nd dose of Sinopharm vaccine and 43 days after 2nd dose of Pfizer Vaccine.
- Anti -Spike antibodies test was done on 30/7/2021 (146 days or 4 months and 26 days after 1st dose of Sinopharm vaccine) titer of antibodies titer 3081U/mL. After 3months and 16days after 2nd dose of Pfizer 107 days.
- Anti- Spike antibodies was done on 30/8/2021(176 days or about 6 months after 1st dose of Sinopharm vaccine), titer of antibodies was 2459U/mL. 4 months and 17 days after 2nd dose of Pfizer (137 days).
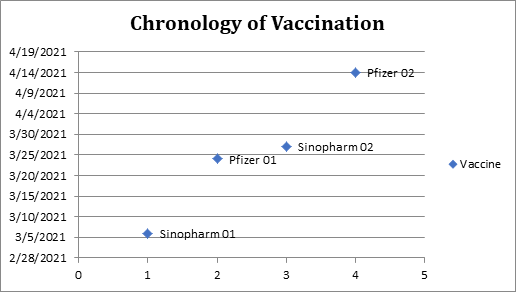
0-pcr test was negative for SARS-CoV-2 and no IgG antibodies were detected against COVID-19 on 2/24/2021. 1-1st dose of Sinopharm (01) administered on 3/6/2021(6th of March 2021) 2-1st dose of Pfizer (01) administered on 3/24/2021(24th March 2021) 3- 2nd dose of Sinopharm (02) administered on 3/27/2021(27th March 2021). 4-2nd dose of Pfizer (02) administered on 4/14/2021(14th April 2021) Explanation of (Figures 1 & 2, Table1): Since the detection limit of the Elecys (Anti-SARS-CoV-2 S) Immunoassay done on Cobas e 411 instruments using electrochemiluminescence Immunoassay (ECLIA).
| LAB | MRN NO | RESULTS | |
|---|---|---|---|
| 24/2/21 | Shaukat Khanum | 001-80003395742 BE-FOR VACCINATION | Coronavirus Antibody Test-Post Vaccination (SARS-CoV-2S) <0.40U/ML Interpretation: -Non Rreactive |
| 6/3/2021 | Sinopharm FIRST DOSE vaccine given | CODE 2620 in PIMS | No side effects |
| 18/3/21 | REHMAN | 2118375322 | PCR SARS-CO-V2 NEGATIVE |
| 24/3/21 | MEDICLINIC DUBAI | 20454398 | 219 Novel Corona Virus-(sars-Cov-2) Not detected |
| 24/3/2021 | 1st DOSE Pfizer Vaccine given | MRN # 921025679 | No side effects |
| 27/3/2021 | 2nd DOSE Sinopharma vaccine given | Code:-5975 | No side effects |
| 27/3/2021 | Post vaccination SARS-COV-2S ANTIBODIES BY Elecys(Anti-SARS-COV-2S-Quantitative-Shaukat Khanum | MRN 001-80003395742 | 3.39U/mL On the same day of having 2nd dose of SINOPHARM & 3 days after Pfizer Vaccine |
| 10/4/2021 | Post vaccination SARS-COV-2S ANTIBODIES BY Elecys(Anti-SARS-COV-2S-Quantitative-Shaukat Khanum | MRN 001-80003395742 | Coronavirus Antibody Test-Post Vaccination (SARS-CoV-2S)Coronavirus Antibody Test-Post Vaccination (SARS-CoV-2S)682.00 U/mL14 Days after 2nd Dose of Sinopharm and17 days after Pfizer 1st Dose |
| 14/4/2021 | 2nd dose Pfizer | MRN # 921025679 | Pains and aches, feverish feeling and drowizness lasted for about 6 hours on day one only |
| 27/4/2021 | Post vaccination SARS-COV-2S ANTIBODIES BY Elecys(Anti-SARS-COV-2S-Quantitative-Shaukat Khanum | Coronavirus Antibody Test-Post Vaccination(SARS-CoV-2S)2500.00 U/mL27 Days after 2nd Dose of Sinopharm and13 days after Pfizer 2nd Dose | |
| 27/05/2021 | Post vaccination SARS-COV-2S ANTIBODIES BY Elecys(Anti-SARS-COV-2S-Quantitative-Shaukat Khanum | 57 days after 2nd dose of Sinopharm vaccine and 43 days after 2nd dose of Pfizer Vaccine titre 4764U/mL. | |
| 30/7/2021 | Post vaccination SARS-COV-2S ANTIBODIES BY Elecys(Anti-SARS-COV-2S-Quantitative-Shaukat Khanum | Titer of antibodies 3081 after 4 months and 24 days 144 days from 1st day of the 1st dose of Sinopharm and 3months and 16 days after 2nd dose of Pfizer (106 days) | |
| 30/8/2021 | Titre of antibodies 2459 after 6 months,189 days from 1st day of the 1st dose of Sinopharm and 4 months and 16 days after 2nd dose of pfizer (137 days) |
Table 1: Record of the EHIB Vaccination and antibodies.
- Anti-spike antibodies and PCR test for COVID-19 were negative before the vaccination and there was little increase in these antibodies (3.93U/mL) on 27th March ie 21 days after the 1st dose of Sinopharm vaccine (date of 2nd dose of the same vaccine).
- There was a moderate increase of 682.00U/mL of these antibodies on 10/4/2021(35 days after 1st dose of Sinopharm Vaccine), 14 days after the 2nd dose of Sinopharm and 17 days of the 1st dose of Pfizer Vaccine.
- There was a much higher increase to 2500.00U/mL on 27/04/2021 which is 52 days after 1st dose of Sinopharm vaccine, 27 days after the 2nd dose of Sinopharm and 13 days after the 2nd dose of Pfizer.
- Anti-spike antibodies test titer (post-vaccination antibodies Test) done on 27/05/2021(82 days after 1st dose of Sinopharm Vaccine), 52 days after 2nd dose of Sinopharm
vaccine and 43 days after 2nd dose of Pfizer Vaccine. 4764U/ mL.
- Anti -Spike antibodies test was done on 30/7/2021 titer of antibodies was 3081 after 4 months and 26 days 146 days from 1st day of the 1st dose of Sinopharm and 3months and 16 days after 2nd dose of Pfizer (107 days).
- Anti- Spike antibodies was done on 30/8/2021 2459 titer of antibodies after 6 months, 176 days from 1st day of the 1st dose of Sinopharm and 4 months and 16 days after 2nd dose of Pfizer (137 days).
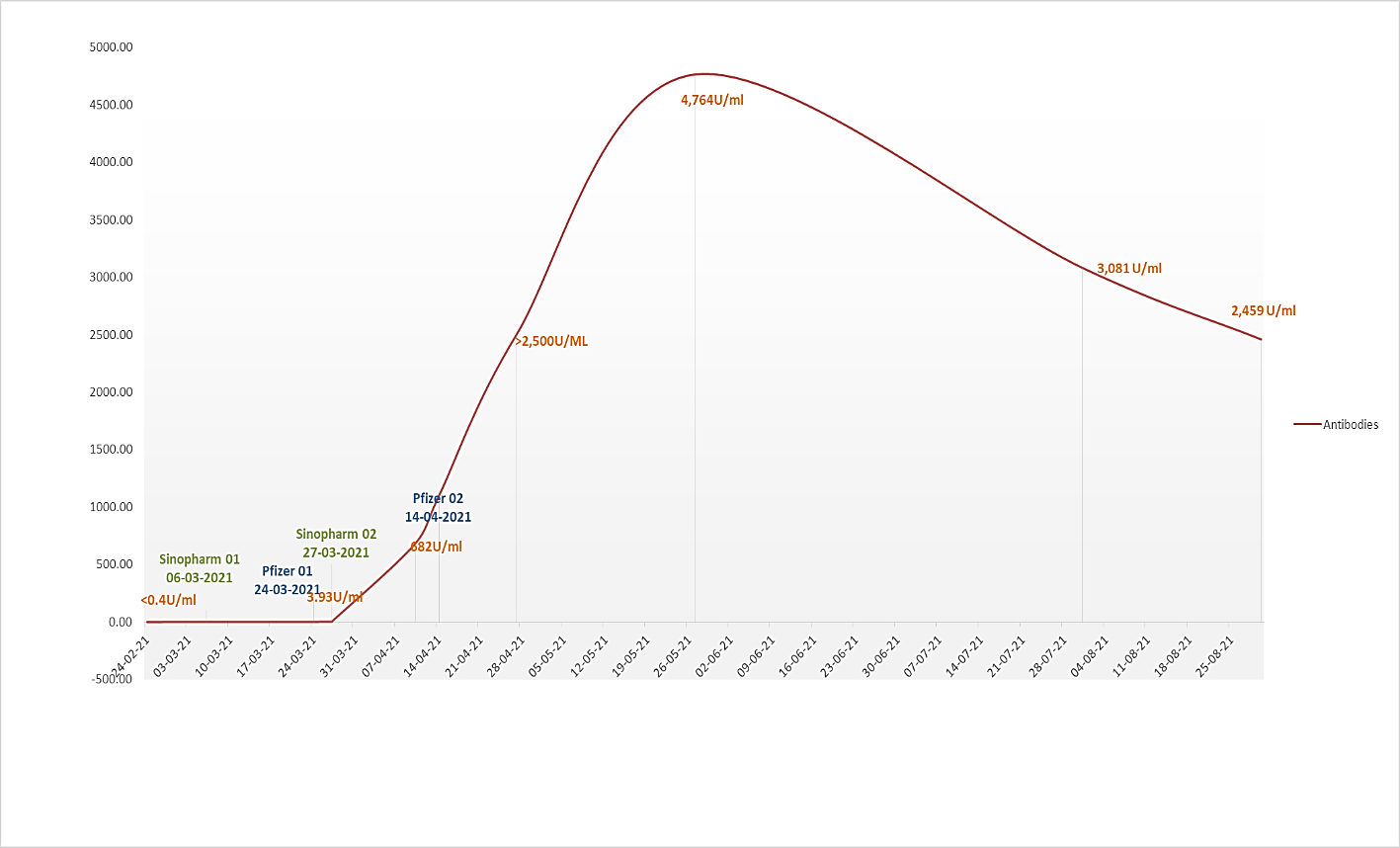
Antibody Response against Vaccination (Figures 1 & 2, Table1):
- The data shows that 1st dose of Sinopharm generated an insignificant titer of anti-spike antibodies (3.93U/mL) till 21 days after the first dose of Sinopharm Vaccine.
- 14 days (2 weeks) after 2nd dose of Sinopharm vaccine there was a moderate increase in anti-spike antibodies (titer 682.U/mL) indicating there is an only moderate increase in antibodies two weeks after the 2nd dose of Sinopharm or17 days after 1st dose of Pfizer. This could have been the combined effect of the 2 doses of Sinopharm Vaccine and one dose of Pfizer. It could be immunopotentiation of Sinopharm (two doses) and a single dose of Pfizer Vaccine otherwise the titer of Sinopharm Vaccine could be lesser.
- 27/04/2021, It is important to note that 13 days (2 weeks) after the 2nd dose of Pfizer much higher levels of anti-spike antibodies were detected 2500.00U/mL. Although killed virus vaccines are normally known to generate much higher levels of anti-spike antibodies while mRNA vaccines generate a much lower level of antibodies ad higher levels of cellular immune response 81,85. But here we have noticed that the killed virus vaccine (Sinopharm alone does not generate a higher level of antibodies even after two jabs of the vaccine (titer was 682U/mL, about 2 weeks after 2nd dose of Sinopharm). Important to note that 1st dose of the mRNA Vaccine caused initial slight boosting but 2nd dose of mRNA potentiated the immune response and much higher 27/05/2021, 43 days after 2nd dose of Pfizer Vaccine the anti-spike antibodies further increased to highest level of 4764U/mL anti-spike antibodies and then titer started decreasing.
- On 30th July 2021 i.e 146 days after 1st dose of Sinopharm vaccine and 107 days or 3 months and 17 days after 2nd dose of Pfizer the titer decreased to 3081U/mL (decrease of 1683u/ml in 64 days which is about which is about 35.3% in 2 months and 4 days or 17.6% per month.
- On 30th August 2021 (176 days or about 6 months after 1st dose of Sinopharm) titer further decreased to 2459U/mL after 2nd dose of Pfizer (137 days or 4 months and 17 days). The decrease was 2305U/mL or
20% in one month.
- Total decrease 48.3% in 4 months and 14 days n four and half months after 2nd dose of Pfizer.
- The rapid fall in first 2 months of about 17.6% in first two months.
- It is important to note that in 1st 2 months after 2nd dose of Pfizer the decrease was rapid and 17.6% and then antibodies decrease more slowly. There was total decrease in 4 months and 17 days.
- But this titer with 1:3 dilution will be followed up every 2-3 monthly. This will help to determine that the EHIB Vaccination schedule has:
- Immune boosting potential.
- Kinetics of the anti-spike antibodies with this strategy.
- How long the acceptable protective antibodies persist in the body after the EHIB (Enhanced Heterologous Immuno-Boost Vaccination against COVID-19.
- Compare with other vaccination schedules like Homologous Prime Boost and Heterologous Prime Boost strategies.
Conclusion
Antispike antibody response as demonstrated in Fig.1, Fig.2 and Table1 confirms our thesis that Enhanced Heterologous Immuno-Boost Vaccination can potentiate the immune response and there were enhanced Anti-Spike antibodies. On this basis, there are strong chances that the combined effect will lead to a much superior cellular response and EHIB will be more effective against the variants(as explained that there are numerous epitopes on the RBD region and when enhanced antibodies are generated against the different epitopes of the RBD then there is the possibility that some types of antibodies may not be effective in preventing attachment of the virus to the ACE2 receptors but still there are numerous antibodies generated in response to the EHIB Vaccine strategy that there are sufficient antibodies still present to prevent the variant. (It is to be noted that variants have only a limited number of amino acids variation in epitope while the major region of the RBD is still the same). The author believes that the Enhanced Heterologous Immuno-Boost strategy can generate a much superior and lasting humoral and cellular immune response and will be a basis of further research and implement the EHIB boost Strategy of Vaccination against COVID-19. But due to financial constraints, cellular studies could not be done in our clinic and this study will lead to further comprehensive studies to prove the thesis.
Suggestions
This pandemic is preparing us to adapt to a diverse way of living with positives and major negatives that directly or indirectly affect our mental states. These include a risk of depression and anxiety, a sense of detachment, loneliness, fear of losing our loved ones, and stressing about our futures. It offered valuable insights on the social, economic, and health impacts faced by households that consisted of adults who suffered from chronic breathlessness, children who had acute respiratory conditions, and women with gynecological problems. Therefore, we need to get some immune booster agents such as vaccines. Every year, vaccines protect millions of people’s lives. Vaccines function by retraining and strengthening the body’s natural defenses, the immune system, to detect and combat the viruses and bacteria they are designed to combat. If the body is exposed to such disease-causing microorganisms after vaccination, the body is prepared to kill them right away, minimizing sickness. Effective and reliable vaccinations will improve the future, but for the time being, we should start wearing masks, keep a safe distance, and avoid crowds. To speed healthcare innovation and combat the coronavirus, organizations all across the world are implementing considered trying technology as well as inventing new ones. There are different platforms for Covid-19 vaccines and many different vaccines developed with their various conditions. Vaccinations are a significant new tool to combat over Covid-19, and the fact that far too many vaccines are proven effective and are being developed is quite promising. There is increasing awareness that these vaccines can have significant positive effects on people’s health, physical well-being and mental states. The people in whole world need to the vaccination to overcome the social challenges and problems in the Covid-19 pandemic.
References
-
Meng L, Hua F, Bian Z (2020) Emerging and Future Challenges for Dental and Oral Medicine. J Dent 99(5): 481-487.
-
Islam S, Islam R, Mannan F, Rahman S, Islam T (2020) COVID-19 pandemic An analysis of the healthcare social and economic challenges in Banglades. Progress in Disaster Science 8: 100-135.
-
UNCTAD Defending Competition in the markets during COVID-19 (UNCTAD, 2020).
-
Jones CB, Isham L (2020) The pandemic paradox The consequences of COVID-19 on domestic violence. J Clin Nurs (13-14): 2047-2049.
-
Gondauri D, Mikautadze E, Batiashvili M (2020) Research on COVID-19 Virus Spreading Statistics based on the Examples of the Cases from Different Countries. Electronic Journal of General Medicine 17(4): 209.
-
Marshall JS, Warrington R, Watson W, Kim HL (2018) An introduction to immunology and immunopathology. Allergy Asthma Clin Immunol 14(2): 49.
-
van Boheemen S, de Graaf M, Lauber C, Bestebroer TM, Raj VS, et al. (2012) Genomic characterization of a newly discovered coronavirus associated with acute respiratory distress syndrome in humans. MBio 3(6): e00473-12.
-
Li W, Moore MJ, Vasilieva N, Sui J, Wong SK, et al. (2003) Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 426(6965): 450-454.
-
Li F, Li W, Farzan M, Harrison SC (2005) Structure of SARS coronavirus spike receptor binding domain complexed with receptor. Science 309(5742): 1864-8.
-
Li F (2016) Structure Function and Evolution of Coronavirus Spike Proteins. Annu Rev Virol 3(1): 237- 261.
-
Prompetchara E, Ketloy C, Palaga T (2020) Immune responses in COVID-19 and potential vaccines Lessons learned from SARS and MERS epidemic. Asian Pac J Allergy Immunol 38(1): 1-.99
-
Wan Y, Shang J, Sun S, Tai W, Chen J, et al. (2020) Molecular Mechanism for Antibody-Dependent Enhancement of Coronavirus Entry. J Virol 94(5): e02015-19.
-
Grifoni A, Weiskopf D, Ramirez SI, Mateus J, Dan JM, et al. (2020) Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals. Cell Jun 181(7): 1489-1501.e15.
-
Different COVİD-19 Vaccines | CDC.
-
https://www.boredpanda.com/Covid-vaccines-cards- lapipette etienne/?utm_source=tr.search.yahoo&utm_ medium=referral&utm_campaign=organic.
-
Immunological considerations for COVID-19 vaccine strategies: Mangalakumari Jeyanathan etall- Nature Reviews | IMMUNOLOGY Reviews volume 20, October 2020.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future