Aluminium Leukoencephalopathy in an Alcoholic Patient
Potentially toxic elements have a wide range of use for human mankind. But with those applications, they also have a darker side with its impact on human health. The affection of potentially toxic elements in humans causing neurological symptoms is also well known. Out of those potentially toxic elements, aluminium is known to cause dialysis encephalopathy in chronic kidney disease patients in the past. Aluminium leukoencephalopathy resulting from other causes is not commonly reported. To the best of our knowledge only seven cases have been reported in the literature till date. We present aluminium intoxication in a patient consuming country liquor causing leukoencephalopathy.
Introduction
Aluminium leukoencephalopathy is a rare entity worldwide. The route of entry of aluminium into human body is through gastrointestinal tract, lungs, nose, and skin [1]. It was well described in patients of chronic kidney disease who undergo hemodialysis [2]. One prior case report has found aluminium deposits in central nervous system [3]. Here we present a case of leukoencephalopathy caused by aluminium toxicity in patient consuming country liquor.
Case Report
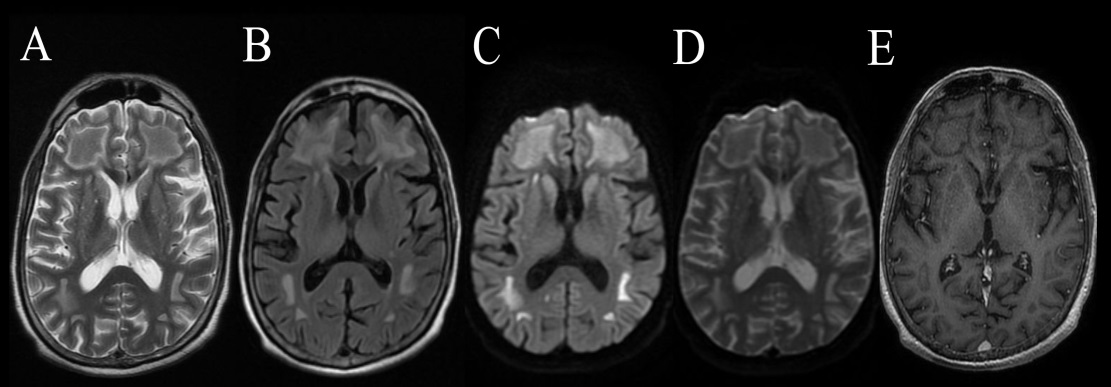
A 63 year old man presented to the emergency department with subacute onset and progressive cognitive impairment in the form of memory loss and decreased processing speed. He used to consume approximately 300 ml per day of country liquor for 10 years whose source was unknown. On examination, patient had altered sensorium, Glasgow Coma Scale of E3V2M5, sluggishly reactive bilateral pupils, increased muscle tone, brisk deep tendon reflexes and bilateral extensor planter response. His blood investigations including complete blood count, liver and renal function tests were normal. Cerebrospinal fluid study was normal. Thyroid function test, anti-thyroid peroxidise, vitamin B12, folic acid, serum lactate, and creatine phosphokinase were within normal limits. Viral serology and autoimmune profile were negative. Contrast enhanced computed tomography of thorax, abdomen, and pelvis was normal. Heavy metal screening in serum revealed aluminium concentration to be 67.78 µg/L (reference value <10). Electroencephalography showed generalized slowing. Brain MRI Figure 1 showed symmetrical T2/FLAIR hyperintense areas involving deep white matter of both frontoparietal and occipital regions along with diffusion restriction and corresponding drop in ADC sequence. The gray matter was spared and mild enhancement especially in frontal white matter was visible. Magnetic Resonance Spectroscopy showed normal Cho/ NAA and Cho/Cr ratio. Brain biopsy was not feasible in our hospital. Based on neurological features, high serum aluminium concentration, radiological abnormalities and battery of investigations ruling out other causes, the patient was diagnosed as a case of toxic leukoencephalopathy secondary to aluminium toxicity. Symmetric periventricular white matter involvement with gray matter sparing is seen in acute toxic leukoencephalopathy [4]. The country liquor which the patient used to consume could not be obtained for laboratory analysis. The relatives of the patient did not give consent for chelation therapy, and the patient succumbed in the following week of admission. Autopsy was not performed as approval was not given by family members.
Discussion
The clinical spectrum of aluminium leukoencephalopathy include cognitive dysfunction, seizures, behavioural features, visual symptoms, motor impairment, cerebellar signs, tremors, dystonia and delirium. Aluminium can cause neurotoxicity by oxidative damage to myelin [5]. We included autoimmune, paraneoplastic, toxic and metabolic etiologies in our differential diagnosis and consequently investigated accordingly. Consumption of country liquor and its health hazards are already present in public domain [6]. This kind of liquor production lacks proper distillation process and is unregulated. This case further highlights and alerts concerned authorities to take appropriate steps for banning this type of dangerous alcohol consumption.
Author Roles
• Research project: A. Study concept and design, B. Acquisition of data, C. Analysis and interpretation of data, D. Supervision.
• Manuscript: A. Writing of the first draft, B. Review and revision.
• PB: 1A, 1C, 1D, 2A
• SK: 1A, 1D, 2B
• VS: 1B , 1C, 2B
• KR: 1B , 1C, 2B
• AK: 1B , 1C, 2B
Disclosures
Ethical Compliance Statement
The authors confirm that approval of an institutional review board was not required for this work. Informed written consent was obtained from patient’s relatives.
Funding Sources and Conflicts of Interest
The authors report no relevant disclosures or conflicts of interest for this manuscript. Funding – The authors did not receive support from any organization for the submitted work. Conflicts of Interest : The authors have no conflicts of interest to declare that are relevant to the content of this article.
Highlights
Consider toxic leukoencephalopathy and do heavy metal screening when symmetric periventricular white matter involvement with gray matter sparing is seen in patients suspected to have toxin exposure. Consent to Publish – Patient’s relative signed informed consent regarding publishing data and photographs.
References
-
Exley C (2013) Human exposure to aluminium. Environ Sci Process Impacts 15(10): 1807-1816.
-
Wills MR, Savory J (1989) Aluminum and chronic renal failure: sources, absorption, transport, and toxicity. Crit Rev Clin Lab Sci 27(1): 59-107.
-
Reusche E, Pilz P, Oberascher G, Lindner B, Egensperger R, et al. (2001) Subacute fatal aluminum encephalopathy after reconstructive otoneurosurgery: a case report. Hum Pathol 32(10): 1136-1140.
-
Oliveira AM, Paulino MV, Vieira APF, Lucato LT, McKinney AM, et al. (2019) Imaging Patterns of Toxic and Metabolic Brain Disorders. Radiographics 39(6): 1672-1695.
-
Verstraeten SV, Golub MS, Keen CL, Oteiza PI (1997) Myelin is a preferential target of aluminum-mediated oxidative damage. Arch Biochem Biophys 344(2): 289- 294.
-
BBC (2011) Who, What, Why: Why are Indians dying from alcohol poisoning.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future