Post-vaccination Levels of Covid Spike Specific IgA Antibody in Nasopharyngeal Samples
Although Covid vaccines are manufactured with improved technology and delivered parenterally, their effectiveness in inducing mucosal immunity remains uncertain. Mucosal immunity plays an important role in protection against Covid-19; but unfortunately, it wasn’t considered in developing the vaccines when the pandemic emerged due to the challenges of high mortality and large-scale vaccine demand. The induction of a high Covid-specific secretary IgA antibody is important for early virus neutralization at its mucosal entry portals, and helps to eradicate the virus in the respiratory and other mucosae. The study demonstrated lower levels of IgA antibodies, which were anticipated due to the route of vaccine delivery rather than the COVID vaccine types that contain the viral spike in the form of inactivated, expressing vector or spike mRNA genes.
Abbreviations
IgA: Immunoglobulin A; SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus; ELISA: Enzyme Linked Immunoassay; SABC: Strept Avidin-Biotin Complex; PCR: Polymerase Chain Reaction.
Introduction
The role of Mucosal IgA in Covid protection
Secretary immunoglobulin A (IgA) represents the major class of antibody which provides humoral protection against microbial pathogens at the mucosal linings on surface of respiratory, genitourinary, and gastrointestinal surfaces [1].
At the early entry site of SARS-CoV-2 in nasal mucosa, IgA antibodies might directly prevent or block virus infection by the nasal, oral, and conjunctiva. Antibodies in the respiratory tract or oral cavity have been considered to protect against transmitted respiratory illnesses [2].
There are two subclasses named IgA1 and IgA2. The monomeric IgA predominates in serum. The dimers of either IgA1 or IgA2 - linked by a J-chain - are present on the mucosal surface where they exert a major role in protection against toxins, viruses and bacteria by neutralization, or by preventing attachment to the virus receptor on mucosal epithelium [3].
In early SARS-CoV-2 specific humoral response is dominated by IgA antibodies responses greatly contributing to virus neutralization. The lack of anti-SARS-Cov-2 IgA and secretory IgA (sIgA) might represent a possible cause of COVID-19 severity, vaccine failure, and possible cause of prolonged viral shedding in a symptomatic patients with primary antibody deficiencies, including patients with Selective IgA Deficiency [4].
It is striking that all marketed SARS-CoV-2 vaccines are developed for intramuscular administration designed to generate humoral and cell mediated immune responses, preventing viremia and the COVID-19 syndrome. They are expected to have a power full efficacy in humans (70–95%) according to the type of vaccine. While, little protection is provided against viral replication and shedding in the upper airways due to the lack or failure developing high level of mucosal sIgA immune response, indicating a risk of transmission of virus from vaccinated healthy carrier individuals [4].
In the preliminary data on salivary IgA that have been generated with the extensive published data on the critical role played by mucosal immunity in protecting against respiratory viruses for those vaccinated by sinopharm vaccine and un vaccinated individual. This makes a strong case for the clinical, research, and public health communities to better understand sIgA’s role in COVID-19 and to evaluate the possibility of its use in patient management, community monitoring, and vaccine development [5].
Aim: The study examined the capability of COVID parenteral vaccines to induce protective Covid spike-specific secretory IgA antibodies in the vaccinee’s nasopharyngeal samples.
Methods
A total of 29 nasopharyngeal swabs were collected from parentally immunized individuals who received two doses of COVID-19 (5 participant received Oxford AstraZeneca vaccine & 24 received Pfizer vaccine). The participants did not have COVID clinical symptoms at the time of sample collection. However, it was possible that some of them were healthy carriers or had recovered from earlier infections.
All participants were tested negative for covid-19 in Rt- PCR at the time of samples collection. A quantitative ELISA test kit with known standards ranged (0-25) ng/ml; used to determine Covid spike-specific IgA antibody level in 96- well microplates ELISA test kit (Table 1), pre-coated with recombinant 2019-nCoV Spike protein (antigen).
A calibration curve was created and used for calculating IgA concentration per sample. Negative control samples from individuals without a history of infection or having received the Covid vaccine were included.
| Item | Specifications | Storage |
|---|---|---|
| Coated ELISA Microplate | 8×12 | 2-8°C/-20°C |
| Standard | 1 vial | 2-8°C |
| Sample/Standard Dilution Buffer | 20ml | 2-8°C |
| Biotin-labeled Antibody(Concentrated) | 60ul | 2-8°C(Avoid Direct Light) |
| HRP-Streptavidin Conjugate(SABC) | 60ul | 2-8°C (Avoid Direct Light) |
| Antibody Dilution Buffer | 5ml | 2-8°C |
| SABC Dilution Buffer | 5ml | 2-8°C |
| TMB Substrate | 5ml | 2-8°C (Avoid Light) |
| Stop Solution | 5ml | 2-8°C |
| Wash Buffer(25X) | 30ml | 2-8°C |
Table 1: ELISA Kit.
Procedure Summary
Step 1: Wash plate 2 times before adding Standard, Sample (diluted at least 1/50 with Sample Dilution Buffer) and Control (blank) wells! Step 2: Add 50ul standard or sample to each well and incubate for 30 minutes at 37°C. Wash step: Aspirate and wash plates 3 times. Step 3: Add 50ul Biotin-labeled antibody working solution to each well and incubate for 30 minutes at 37°C.
Wash step: Aspirate and wash plates 3 times. Step 4: Add 50ul SABC Working Solution into each well and incubate for 30 minutes at 37°C. Wash step: Aspirate and wash plates 5 times. Step 5: Add 50ul TMB Substrate Solution. Incubate 10-15 minutes at 37°C. Step 6: Add 50ul Stop Solution. Read at 450nm immediately and calculation
Results
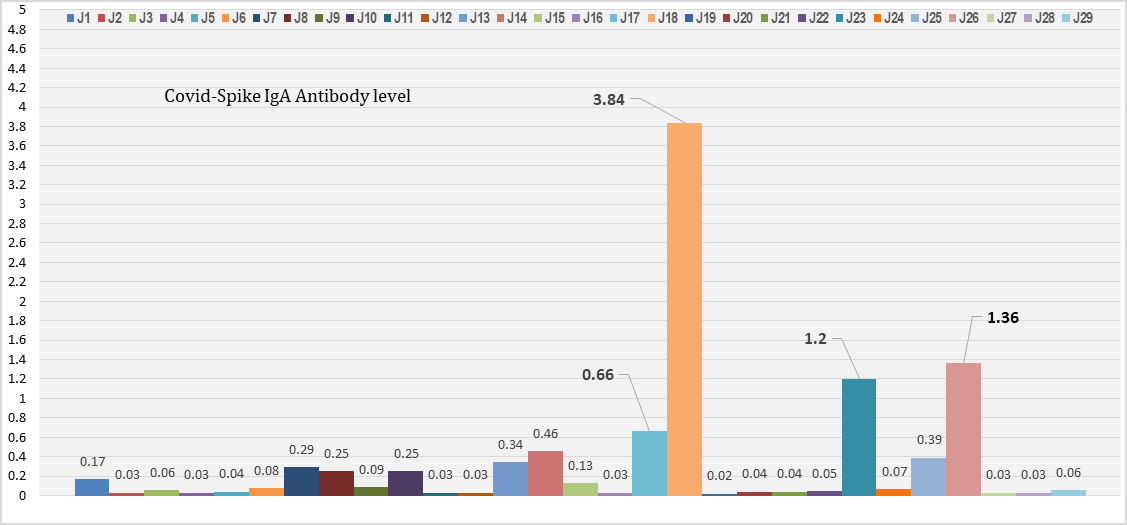
The results showed low levels of Covid spike specific IgA in most of the participants (86.2%. Only four samples showed elevated IgA, which represents 13.8% (Figure 1). The least IgA level among them was 0.01 ng/ml and medium elevated in the range 0.5-1.5ng/m in 3 individuals.
One participant’s sample showed a highly elevated level of IgA (3.4 ng/ml) indicating prior mucosal exposure to Covid infection as a healthy carrier or a recently recovered individual. The sample was re-tested and found negative for Covid RNA by PCR (Figure 1) [1].
Discussion
Higher IgA levels are required to neutralize and limit Covid spike adhesion to ACE-2 receptors, hence preventing Covid-19 from infecting target cells, replicating, and spreading among vaccinated individuals.
As a result, the findings show that vaccines fail to elicit sufficient mucosal protective IgA antibodies, primarily because all Covid vaccines are provided parentally without establishing mucosal immunity by oral immunization or nasal spray administration.
The existence of elevated IgA was only in three samples show raised IgA out of the 29 participants, which is most likely due to the presence of activated mucosal antigen- presenting memory cells after exposure to natural infection prior to or during vaccine doses. And this finding is in line with Sano, K, et al. [6].
Especially intriguing is our anecdotal finding that exposure to sub-infective doses of SARS-CoV-2 could induce a mucosal immune response as measured by salivary IgA.
A speculative interpretation is that the threshold of viral exposure required to induce a mucosal IgA response may be below that required to induce and establish infection or generate a measurable IgG response.
It also explained why the virus co-existing might continue to circulate at respiratory portals in vaccinated individuals who have become Covid healthy carriers despite receiving numerous doses after despite worldwide vaccination attempts.
Conclusion
This research concludes that employing a single immunization parenteral method to deliver the Covid vaccine may impair the vaccine’s capacity to elicit sufficient protective mucosal immunity. This is evidenced by the current prevalence of COVID infections among individuals who have received several vaccine doses.
The low post-vaccination IgA level proves the global demands for developing a new version of a mucosal- delivered Covid vaccine to boost enough protective secretary IgA to neutralize, block viral entry, and inhibit its replication at entry sites, in order to terminate the virus’s existence and halt its transmission as the only possible way for any future strategy or plan aiming for the eradication of covid-19.
Conflict of interest
All authors declared no conflict of interest.
References
-
Lippi G, Salvagno GL, Henry BM, Pighi L, Nitto SD, et al. (2022) Comparative longitudinal variation of total IgG and IgA anti-SARS-CoV-2 antibodies in recipients of BNT162b2 vaccination. Advances in Laboratory Medicine 3(1): 39-43.
-
Chan RWY, Liu S, Cheung JY, Tsun JGS, Chan KC, et al. (2021) The mucosal and serological immune responses to the novel coronavirus (SARS-CoV-2) vaccines. Frontiers in immunology 12: 744887.
-
Quinti I, Mortari EP, Salinas AF, Milito C, Carsetti R (2021) IgA antibodies and IgA deficiency in SARS- CoV-2 infection. Frontiers in Cellular and Infection Microbiology 11: 655896.
-
Tiboni Ma, Casettari L, Illum L (2021) Nasal vaccination against SARS-CoV-2: Synergistic or alternative to intramuscular vaccines? International journal of pharmaceutics 603: 120686.
-
Varadhachary A, Chatterjee D, Garza J, Garr RP, Foley C, et al. (2020) Salivary anti-SARS-CoV-2 IgA as an accessible biomarker of mucosal immunity against COVID-19. MedRxiv.
-
Sano K, Bhavsar D, Singh G, Floda D, Srivastava K, et al. (2022) SARS-CoV-2 vaccination induces mucosal antibody responses in previously infected individuals. Nature Communications 13: 5135.
- Update on Malariology and Malaria Vaccines
- Addressing Vaccine Hesitancy in the Age of Measles Resurgence: A Mini-Review
- Exploring Barriers and Facilitators of Group Antenatal Care Implementation in Kaduna State, Nigeria: A Qualitative Evaluation
- The Role of IL-11 in Regenerative Medicine and Tissue Engineering
- New Prediction of Mortality rate of Covid -19 According to WHO Estimation
- Measles Vaccine in Kano, Northern Nigeria: Past, Present and Future