Adhesiolysis in Women with Chronic Pelvic Pain and a Temporal Resolution of Pain
Study Objectives: To evaluate the duration of pain improvement after laparoscopic and/or robotic assisted adhesiolysis in women with prior abdominal or pelvic surgeries that have been diagnosed with chronic pelvic pain with suspected pelvic and/or abdominal adhesions. Design: Retrospective Cohort (Canadian Task Force Level II) Setting: Hospital based practice of gynecological surgery and pelvic pain, St. Joseph Hospital and Medical Center, Phoenix AZ Patients: Women with prior surgery who underwent laparoscopic or robotic assisted adhesiolysis for chronic pelvic pain secondary to pelvic and/or abdominal adhesions between April 2012-Febuary 2016. Intervention; Adhesiolysis performed via laparoscopic or robotic assisted, defined as 30 minutes or greater of operating time needed to restore normal anatomy. Measurements and Main Results: Eighty-eight women were identified with Current Procedural Terminology (CPT) code 4410 and 58550 for adhesiolysis. Women > 18 years old who had prior surgery, and symptoms of pelvic pain were included in the study. Women were excluded if they were found to have another source of pelvic pain, malignancy, surgical complications, co-surgery with another specialty, and conversion to laparotomy, and organ resection. The average age at the time of adhesiolysis was 39 years old (range of 19-57). The average number of abdominal surgeries was 1.42 (range 1-4). Fifty-six patients were excluded for concomitant procedures. Thirty-patients patients meet eligibility criteria, of those; seventeen patients had previously undergone at least one adhesiolysis procedure for the treatment of chronic pelvic pain. All 17 of these patients had improvement of their pain. Fourteen of the 17 patients had 2 adhesiolysis procedures with the median length of time between the first and second procedure (improvement in pain after procedure) being 24 months (range of 6-162 months). Three of 14 underwent a third adhesiolysis procedure with the median pain free interval of 24 months. Two of the 3 patients had a fourth adhesiolysis procedure with the average pain free interval being 24 months prior to the 4th procedure. Fifteen of the 32 patients, who underwent their first adhesiolysis treatment, 10 had resolution of pain and 5 patients had a significant improvement of pain. Of this cohort the earliest reported return of pain was 6 months, and the longest total pain free interval was 13 years and 6 months. Conclusion: In patients who present with pelvic pain and prior abdominal or pelvic surgery adhesiolysis may be associated with a temporal improvement of pain.
Introduction
The International Association for the study of Pain (IASP) defines chronic pelvic pain (CPP) as pain that lasts for more than 6 months and notes that at least 20% of chronic pelvic pain is from a gynecologic cause [1]. CPP has a complex etiology because it can be associated with gynecologic, urologic, gastrointestinal, musculoskeletal, and psychosocial comorbidities [2]. As a result, a chronic pain evaluation may include an exhaustive course of tests and studies without a clear diagnosis or treatment plan and the pain may be dismissed as drug seeking or malingering pain; which may delay a patient’s diagnosis or treatment [3]. CPP continues to be clinically challenging for gynecologists because symptoms may persist even after standard gynecologic management [4].
When gastroenterological and genitourinary sources have been excluded as the cause of pelvic pain a gynecologic evaluation is warranted. After a thorough history and physical examination, a diagnostic laparoscopy may be a valuable tool for delineating an underlying cause of pelvic pain. It is equally important to note that negative findings on laparoscopy provide reassurance [4, 5, 6, 7, 8]. In approximately 50% of investigative surgeries for chronic pelvic pain pelvic adhesions are often found [5, 6, 7, 8]. Although controversial, it remains unclear if pelvic adhesions encountered during laparoscopy are a source of chronic pelvic pain and whether adhesiolysis provides any relief [9, 10, 11, 12].
Adhesions may be a physical cause for abdominal or pelvic pain, and are known to develop after more than 90% of abdominal surgeries [8, 13]. There continues to be a growing body of literature attempting to address the benefit of surgical intervention for pain associated with adhesions but treatment success has varied and is controversial [14, 15, 16]. Further drawbacks lie with practitioner’s inability to predict the severity of surgical adhesion formation or prevention of re-occurrence following treatment. Adhesiolysis may be beneficial for patients with chronic pelvic pain especially those who have undergone laparotomy, or if there was suspected intestinal involvement, butin those studies there was no confirmation and the power was too small [11, 17, 18, 19, 20, 21].
We hypothesized that adhesiolysis alleviates chronic pelvic pain for a period of time especially in patients with prior surgery. This study was therefore designed with the objective to evaluate the duration of pain improvement after laparoscopic and/or robotic assisted adhesiolysis in women with prior abdominal or pelvic surgeries that have been diagnosed with chronic pelvic pain with suspected pelvic and/or abdominal adhesions.
| Classification of Diseases | |
|---|---|
| Terminology; | BMI: Body M |
Materials and Methods
Institutional review board was requested and approval was received, to conduct a retrospective chart review of a single institution practice. The practice is a referral center that specializes in the evaluation of women with chronic pelvic pain and minimally invasive gynecologic surgery located at Dignity Health St. Joseph’s Hospital in Phoenix, Arizona. It is considered an advanced gynecologic surgery center especially for patients who have undergone multiple surgeries.
This was a retrospective study of all patients who underwent laparoscopic or robotic assisted adhesiolysis for treatment of chronic pelvic pain from February 2012 to November 2016, with prior abdominal and pelvic surgery(s) with adhesive disease. Patients were first identified from the electronic medical records (EMR) with an International Classification of Diseases (ICD)-9 code with an associated Current Procedural Terminology (CPT) code (Table 1). Demographic data, such as patient’s age; body mass index (BMI), prior surgeries, pre-operative subjective pain, intraoperative and postoperative complications, intra-operative consultations, postoperative follow up, postoperative subjective pain, interventions and treatments for post-operative pain was extracted from EMR.
| CPT Code | Procedure | ||||
|---|---|---|---|---|---|
| 44005 | Enterolysis | ||||
| 44180 | Laparoscopy, surgical, enterolysis (freeing of intestinal adhesion) | ||||
| 58660 | Lysis of adhesions involving tubes and ovaries | ||||
| 58740 | Lysis of adhesions (salpingolysis, ovariolysis) |
Table 2: Current Procedural Terminology (CPT) code used to identify patients.
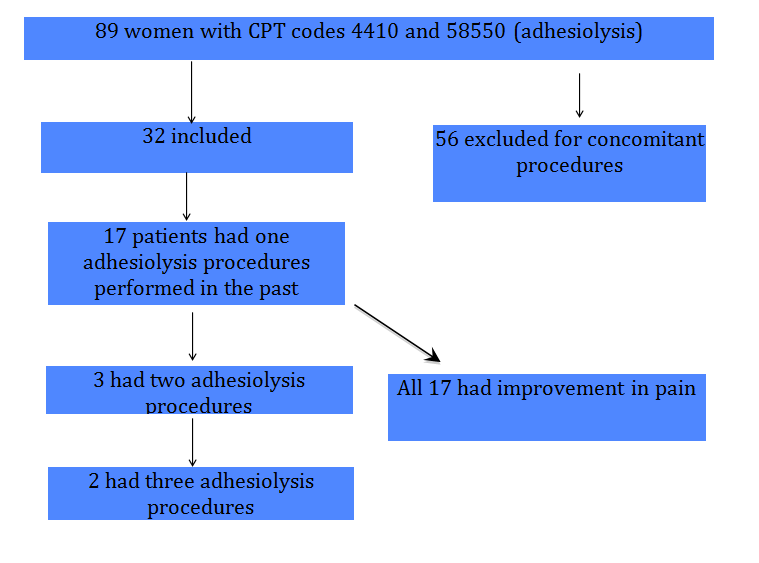
Figure 1 shows that a total of eighty-nine women were identified; Fifty-six patients were excluded for concomitant procedures, as outlined in exclusion criteria. Thirty-two remaining patients, and seventeen (53.1%) patients had previously undergone at least one adhesiolysis within the practice.
The eligibility for inclusion: 1) Women over the age of 18 years old and 2) Patients included in this study were not noted to have gastrointestinal symptoms commonly associated with bowel obstruction such as intermittent nausea and vomiting or changes in their bowel movement 3) Had undergone prior surgery, 4) Presence of chronic pelvic pain defined as pelvic pain which is constant/cyclical in nature for greater than or equal to 6 months duration who had failed physical therapy or medical management. 5) Prior urologic and/or gastrointestinal evaluation for bladder or bowel etiology for pain. Exclusion criteria: 1) If patients had other source of pelvic pain (such as Irritable Bowel, Painful bladder Syndrome, Pelvic Floor Tension Myofascial Pain (PFTM), Pelvic Congestion Syndrome or Endometriosis), 2) Malignancy, 3) Complications during surgery such as visceral injury or repair at the time of adhesiolysis, 4) Concomitant surgeries with other practices such as Gynecologic Oncology, General Surgery or Urology, 5) Conversion to laparotomy, resection, or organ removal such as hysterectomy, salpingectomy or oophorectomy.
During the patient’s pre-operative visit, pain was mainly a verbal self-reported assessment (severe pain, moderate, or mild) and documented. Some patients did have numerical scores from the visual analogue score (VAS) by the McGill pain questionnaire (a quantitative self-reported questionnaire for intensity and quality of pain, however not all assessments were found in the patient’s charts due to transition from paper charts to electronic medical records (EMR) [22].
All surgical procedures either conventional laparoscopy or robotic assisted was performed at the same tertiary hospital that was associated with chronic pelvic pain and minimally invasive gynecologic surgery program. All the surgeons have had extensive experience with both robotic assisted and/or conventional laparoscopy. The decision to proceed with either laparoscopy vs. robot assisted was based on the surgeon’s preference. The operative technique used for patients undergoing adhesiolysis is as follows: For all procedures the patient was placed in the dorsal lithotomy position with legs in Allen-style stirrups. Open technique [23, 24] was used to gain abdominal access, and after abdominal access was verified a 12 mm trocar was placed at the umbilicus to accommodate a 10 mm camera and two 5-mm trocars were placed for conventional laparoscopy. For robotic assisted laparoscopy the DaVinci Surgical System (Intuitive Surgical Inc., Sunnyvale, CA) was consistently docked on the patient’s right side. For robotic-assisted laparoscopy, one 12-mm trocar, two or three (if extensive dissection was needed) 8-mm trocars and one 5-mm assistant trocar were placed.
For conventional laparoscopy, the instruments included a Davis & Geck, laparoscopic forceps and monopolar scissors. The instruments used for robotic- assisted treatment of lysis of adhesions included monopolar scissors Da Vinci PK dissecting forceps advanced bipolar, and grasping forceps if needed in the third arm. Adhesiolysis performed via conventional laparoscopy or robotic assisted, was defined as 30 minutes or greater of operating time needed to restore normal anatomy. Adhesiolysis was accomplished by cutting close to the peritoneum and as far away from the bowel as possible. No adhesion prevention solutions or barriers were used in any of our patients.
Once surgery was completed patients were discharged from the recovery room or they were observed overnight based on the extent of the adhesiolysis and surgeon’s preference. If a patient was observed overnight they were discharged the next day. Patient’s follow-up appointment was scheduled with primary surgeon 6 weeks from the surgery date. At the patient’s 6-week postoperative visit, subjective pain scores were obtained and documented. Pain was a verbal self-reported assessment (complete resolution and continued pain (minimal, moderate, or no change) with some VAS numerical scores. If patients expressed compete resolution of pain at that visit, they were instructed to follow up with their primary gynecologist. However if they continued to have any form of pain they would continue follow-up until adequate pain relief was achieved, and at that time they were cleared to follow-up with their primary gynecologist. This was the routine practice for all patients who presented to this Advanced Pelvic Pain and Gynecology Clinic.
If patients returned after an adhesiolysis procedure and expressed pain, time from prior adhesiolysis surgery to clinic presentation was documented as interval pain improvement or pain free time. Patients who desired to proceed with additional surgery, the average time from clinic visit to surgery was one to two weeks depending on the surgeon’s schedule.
Results
A total of eighty-nine women were identified; 56 patients were excluded for concomitant procedures, as outlined in exclusion criteria. Sixteen patients were excluded because they were found to have another associated diagnosis for pelvic pain 7 PFTM, 4 Painful Bladder Syndrome, 2 Pelvic Congestion, 4 Endometriosis, and2 were excluded for the need to convert to laparotomy. Thirty-two had either a resection or organ removal such as hysterectomy, salpingectomy or oophorectomy. Three patients General surgery was consulted intra-operatively, and one patient had a malignancy. A total of 32 women meet eligibility criteria and underwent adhesiolysis for chronic pelvic pain from February 2012 to November 2016, shown in Figure 1.
The mean age at the time of adhesiolysis was 39 years old (range 19-57). The average number of abdominal surgeries was 1.42 (range 1-4). Prior surgeries included: 8 total robotic assisted hysterectomies, 7 abdominal hysterectomies, 4 vaginal hysterectomies, 1 supra- cervical hysterectomy, 3 exploratory laparotomies, 5 appendectomies, 4 cesarean sections. Other concomitant surgeries included prior lysis of adhesions by an outside provider, removal of ectopic pregnancy via unilateral salpingectomy, cholecystectomy, myomectomy, tubal ligation, and bowel resection.
Results from office pre and post-operative evaluation of pain are summarized in (Table 2). Twenty-five patients had their self-reported pain documented, four VAS numerical scores, and 3 did not have pain documentation at pre-operative visit, as seen in Table 2. One of the patients included was an initial patient of the clinic when it started in 2003, retrospective data was available in her chart and her results were included in the study.
| 1st Surgery | |||||||||
| Pre operative evaluation | Post operative evaluation | ||||||||
| Subjective Pain | 25 patients | Subjective Pain | 25 | ||||||
| VAS pain score | 4 | VAS pain score | 5 | ||||||
| Not documented | 3 | Not documented | 2 | ||||||
| 2nd Surgery | |||||||||
| Subjective Pain | 13 | Subjective Pain | 10 | ||||||
| VAS pain score | 1 | VAS pain score | 0 | ||||||
| Not documented | 0 | Not documented | 4 | ||||||
| 3rd Surgery | |||||||||
| Subjective Pain | 3 | Subjective Pain | 3 | ||||||
| VAS pain score | 0 | VAS pain score | 0 | ||||||
| Not documented | 0 | Not documented | 0 |
Table 3: Pre and Post-operative evaluation of pain from February 2012 to November 2016.
Of the 32 patients included in the study17 (53.1%) patients had previously undergone at least one adhesiolysis within the practice, and 15 (46.9%) had their first adhesiolysis procedure, as seen in Figure 1. Of the 32 patients, nine had laparoscopic adhesiolysis. All 17 of
| 6-week postoperative visit for | 6-week postoperative visit for | |||||||
| 6-week postoperative visit for 1st surgery | ||||||||
| 2nd surgery | 3rd surgery | |||||||
| Number of patients evaluated 32 Pain Improved 18 Pain resolved 10 Not Documented/ Lost to Follow- up 4 | Number of patients evaluated 14 Pain Improved 5 Pain resolved 9 Not Documented/ Lost to Follow- up 0 | Number of patients evaluated 3 Pain Improved 1 Pain resolved 2 Not Documented/ Lost to Follow- up 0 |
Table 4: Post-operative evaluation of pain after adhesiolysis from February 2012 to November 2016.
patients had undergone four adhesiolysis with the average pain free interval being 24 months prior to the 4th procedure. The earliest reported return of pain was 6 months, and the longest total pain free interval was 13 years and 6 months. Of those 15 patients who underwent their initial adhesiolysis procedure, none returned for pain within the study period.
| Time between first 1st and 2nd | Time between first 2nd and 3rd | T | ime between firs 3rd and 4t | h | |||||||
| Patient # | |||||||||||
| adhysiolysis | LOA adhysiolysis | LOA adhysiolysis | |||||||||
| 1 | 24 | 24 | 24 | ||||||||
| 2 | 9 | ||||||||||
| 3 | 30 | ||||||||||
| 4 | 162 | ||||||||||
| 5 | 66 | ||||||||||
| 6 | 62 | ||||||||||
| 7 | 14 | ||||||||||
| 8 | 6 | 30 | 24 | ||||||||
| 9 | 15 | ||||||||||
| 10 | 21 | ||||||||||
| 11 | 39 | ||||||||||
| 12 | 87 | ||||||||||
| 13 | 14 | ||||||||||
| 14 | 24 | ||||||||||
| 15 | 36 | ||||||||||
| 16 | 12 | 18 | |||||||||
| 17 | 42 |
Table 5: Patients and Time interval in months of subsequent surgeries and pain relief.
Discussion
The use of laparoscopic and/or robotic assisted adhesiolysis provided a temporal relief in women with chronic pelvic pain who had undergone prior abdominal and/or pelvic surgeries with adhesive disease. For women who underwent initial adhesiolysis and for those who have had consecutive lysis of adhesions continued to show an improvement or resolution of pelvic pain for a significant period of time. This was further supported in our study, by using a patient that had retrospective data from when the clinic was founded in 2003; her initial surgery was in 2003 with a reoccurrence of symptoms after being pain free for 13 years. As demonstrated in prior studies, this study follows a patient’s self-reported pain and it showed an interval improvement of pain for an extended period of time [17, 25, 26, 27]. This will be the first study to include a cohort of patients who had undergone the same procedure and patients continued to have an improvement of pain symptoms after each procedure was performed.
Even though there remains to be a debate in the role of surgical adhesiolysis and its effectiveness in treating chronic pelvic pain [28, 29, 30, 31, 32]; this study adds support that adhesiolysis is an effective tool in patients who have had prior surgeries and exhibit pelvic pain. McClain, et al. presented that adhesiolysis without organ removal or resection provided a resolution of pain that is different than organ removal or repair. It was proposed that the body notices a correction of the pathology and the pain usually resolves quickly. But when removal or resection does not occur, pain is suspected to be part of the spinal thalamic pathway similar to that found in phantom pain that presents after limb amputation. This may explain why pain resolves over time with adhesiolysis vs. an immediate improvement of pain [33]. Kresch, et al. suggested pain was only presented if the adhesions restricted movement of the viscera because these adhesions may cause tension on the bowel itself [34]. Because patients with adhesions may present with bowel obstruction symptoms (nausea, vomiting, inability to pass flatus, and irregular bowel movements), several require hospitalization and have accounted for Gastrointestinal admissions 51% in the United Kingdom and 60% within the United States [35, 36]. In 1997, adhesive bowel obstruction had 2330 hospital admissions annually, which was associated with an estimated direct cost of about US$13 million [37]. In 2010, 381,364 patients underwent adhesiolysis surgery with an average $65,955 per surgery [38]. Lastly 2016 surgical intervention for adhesive disease was €16,305 (SD €2,513), and for non-operative treatment €, 277 (SD € 265) [36]. It has been proposed that with the use of improved diagnostic tools such as CT Scans and more experience with minimally invasive adhesiolysis may also help reduce cost by decreasing hospitalization time and improve post operative recovery allowing a patient to return to work quicker [25]. It is also difficult to state that all women who have had prior abdominal or pelvic surgeries warrant lysis of adhesion. This was supported by the patients we excluded in our study which were patients who had underwent adhesiolysis but were also found to have endometriosis, malignancy, or pelvic congestion syndrome, and these too could have contributed to their pain in spite of adhesive disease also being present. We further support that a diagnostic laparoscopy should be a tool to help with evaluation and diagnosis for identifying the source of pain [12, 33, 37, 38, 39].
The primary strength of the present study was having a specialized center devoted to pelvic pain. Having such specialized care has enabled consistent follow up and thorough physical exam, in order to evaluate for other sources for pelvic pain (nerve compression, interstitial cystitis, pelvic congestion or pelvic floor tension myofascial pain). With such a work-up other interventions or treatments could be offered aside from surgery in order to ameliorate a patient’s pain. Lastly another strength may be the extensive experience of the both the surgical team, ancillary staff (nurse practitioners or physical therapist), and operating room staff, all of who are familiar in helping to treat this particular group of patients.
Limitations of the present study are the retrospective nature, number of participants identified by the study, lack of uniform evaluation of pre and post-operative pain, and the findings within the surgical documentation did not always thoroughly record the specific location of adhesions. Another issue may have been the absence of a validated questionnaire to effectively assess symptoms and pain. Furthermore many of the patients travel from across the United States and foreign countries and immediately return home with follow-up by their primary gynecologist. This also applied to local patients who had immediate resolution of pain at postoperative visit; they were cleared to follow up with primary gynecologist. Duration or improvement of pain relief may have been skewed if patients never returned to the chronic pelvic pain clinic for evaluation. Confounding factors that can affect results including the surgeon’s skills and experience were not taken into consideration in this study.
Even though our study is retrospective and treats a small representative group of patients with chronic pelvic pain it continues to support that adhesiolysis may be a treatment for patients with chronic pelvic pain especially those with adhesive disease. Prospective double blinded study randomized studies are needed to further validate our results. It is uncertain if enrolling more patients or following patients for a longer duration in the study would affect our results. A future goal would be to develop an algorithm for chronic pelvic pain treatment due to suspected adhesive disease. In order to generate such an algorithm for evaluation and treatment of chronic pelvic pain, as a noted issue with this study documentation would need to be improved. Pre-operative, operative and post-operative documentation with a validated pain score, questionnaire, and detailed operative findings will be needed to help improve patient care. The algorithm would also need to incorporate multiple practices especially those that focus on chronic pelvic pain to develop a multi-disciplinary approach with internists, general surgeons, family practitioners and gynecologist with consistent follow-up. Our institution has continued to enroll and treat patients with chronic pelvic pain and offer them a plan to help improve not only their pain but also quality of life.
We conclude that adhesiolysis improves pain with patient who have had prior pelvic or abdominal surgeries. But the best and definitive form or treatment for these patients has yet to be seen.
References
-
Global Year Against Pain in Women Chronic Pelvic Pain, (n.d.).
-
Jarrell JF, Vilos GA, Allaire C, Burgess S, Fortin C, et al. (2005) Chronic Pelvic Pain Working Group, SOGC, Consensus guidelines for the management of chronic pelvic pain. J Obstet Gynaecol Can 27(8): 781-826.
-
Cheong YC, Reading I, Bailey S, Sadek K, Ledger W, et al. (2014) Should women with chronic pelvic pain have adhesiolysis? BMC Womens Health 14: 36.
-
Allaire C, Aksoy T, Bedaiwy M, Britnell S, Noga HL, et al. (2017) An interdisciplinary approach to endometriosis-associated persistent pelvic pain. J Endometr Pelvic Pain Disord 9(2): 77-86.
-
Howard FM, El Minawi AM, Sanchez RA (2000) Conscious pain mapping by laparoscopy in women with chronic pelvic pain. Obstet Gynecol 96(6): 934- 939.
-
Swank DJ, Swank Bordewijk SC, Hop WC, van Erp WF, Janssen IM, et al. (2003) Laparoscopic adhesiolysis in patients with chronic abdominal pain: a blinded randomised controlled multi-centre trial. Lancet 361(9365): 1247-1251.
-
Rapkin AJ (1986) Adhesions and pelvic pain: a retrospective study. Obstet Gynecol 68(1): 13-15.
-
Yosef A, Ahmed AG, Al Hussaini T, Abdellah MS, Cua G, et al. (2016) Chronic pelvic pain: Pathogenesis and validated assessment. Middle East Fertil Soc J 21(4): 205-221.
-
Nezhat FR, Crystal RA, Nezhat CH, Nezhat CR (2000) Laparoscopic adhesiolysis and relief of chronic pelvic pain. JSLS 4(4): 281-285.
-
Schmidbauer S, Hallfeldt KKJ, Ikard R, Klingensmith M, Soybel D, et al. (2001) Laparoscopic adhesiolysis in the treatment of chronic abdominal pain. Surgery 129(4): 513.
-
Malik E, Berg C, Meyhöfer Malik A, Haider S, Rossmanith WG (2000) Subjective evaluation of the therapeutic value of laparoscopic adhesiolysis: a retrospective analysis. Surg Endosc 14(1): 79-81.
-
Miller K, Mayer E, Moritz E (1996) The role of laparoscopy in chronic and recurrent abdominal pain. Am J Surg 172(4): 353-356.
-
ten Broek RP, Strik C, Issa Y, Bleichrodt RP, van Goor H (2013) Adhesiolysis-Related Morbidity in Abdominal Surgery. Ann Surg 258(1): 98-106.
-
Swallen KC, West DW, Stewart SL, Glaser SL, Horn Ross PL (1997) Predictors of misclassification of hispanic ethnicity in a population-based cancer registry. Ann Epidemiol 7(3): 200-206.
-
Jacobson TZ, Duffy JM, Barlow D, Koninckx PR, Garry R (2009) Laparoscopic surgery for pelvic pain associated with endometriosis. Cochrane Database Syst Rev 4: CD001300.
-
Barbul A (2015) In brief. Abdominal adhesions. Curr Probl Surg 52(27): 266-269.
-
Hammoud A, Gago LA, Diamond MP (2004) Adhesions in patients with chronic pelvic pain: A role for adhesiolysis? Fertil Steril 82(6): 1483-1491.
-
Holloran Schwartz MB (2014) Surgical evaluation and treatment of the patient with chronic pelvic pain. Obstet Gynecol Clin North Am 41(3): 357-369.
-
Howard FM (1994) Laparoscopic evaluation and treatment of women with chronic pelvic pain. J Am Assoc Gynecol Laparosc 1(4): 325-331.
-
Vrijland WW, Jeekel J, van Geldorp HJ, Swank DJ, Bonjer HJ (2003) Abdominal adhesions: intestinal obstruction, pain, and infertility. Surg Endosc 17(7): 1017-1022.
-
Stones W, Cheong YC, Howard FM, Singh S (2015) Interventions for treating chronic pelvic pain in women. Cochrane Database Syst. Rev.
-
Melzack R (1975) The McGill Pain Questionnaire: major properties and scoring methods. Pain 1(3): 277-299.
-
Nuzzo G, Giuliante F, Tebala GD, Vellone M, Cavicchioni C (1997) Routine use of open technique in laparoscopic operations. J Am Coll Surg 184(1): 58- 62.
-
Bonjer HJ, Hazebroek EJ, Kazemier G, Giuffrida MC, Meijer WS, et al. (1997) Open versus closed establishment of pneumoperitoneum in laparoscopic surgery. Br J Surg 84(5): 599-602.
-
Nezhat FR, Crystal RA, Nezhat CH, Nezhat CR (2000) Laparoscopic adhesiolysis and relief of chronic pelvic pain JSLS 4(4): 281-285.
-
Rapkin AJ (1986) Adhesions and pelvic pain: a retrospective study. Obstet Gynecol 68(1): 13-15.
-
ten Broek RP, Issa Y, van Santbrink EJ, Bouvy ND, Kruitwagen RF, et al. (2013) Burden of adhesions in abdominal and pelvic surgery: systematic review and met-analysis. BMJ 347: f5588.
-
Mueller MD, Tschudi J, Herrmann U, Klaiber C (1995) An evaluation of laparoscopic adhesiolysis in patients with chronic abdominal pain. Surg Endosc 9(7): 802- 804.
-
Steege JF, Stout AL (1991) Resolution of chronic pelvic pain after laparoscopic lysis of adhesions. Am J Obstet Gynecol 165(2): 278-283.
-
Hammoud A, Gago LA (2004) Diamond MP, Adhesions in patients with chronic pelvic pain: a role for adhesiolysis? Fertil Steril 82(6): 1483-1491.
-
McClain GD, Redan JA, McCarus SD, Caceres A, Kim J (2011) Diagnostic laparoscopy and adhesiolysis: does it help with complex abdominal and pelvic pain syndrome (CAPPS) in general surgery? JSLS 15(1): 1- 5.
-
Kresch AJ, Seifer DB, Sachs LB, Barrese I (1984) Laparoscopy in 100 women with chronic pelvic pain. Obstet Gynecol 64(5): 672-674.
-
Fact sheet on adhesions and bowel obstruction surgeries.
-
Krielen P, van den Beukel BA, Stommel MWJ, van Goor H, Strik C, et al. (2016) In-hospital costs of an admission for adhesive small bowel obstruction. World J Emerg Surg 11: 49.
-
Ivarsson ML, Holmdahl L, Franzén G, Risberg B (1997) Cost of bowel obstruction resulting from adhesions. Eur J Surg 163(9): 679-684.
-
Bricker L, Neilson JP, Dowswell T (2008) Routine ultrasound in late pregnancy (after 24 weeks’ gestation). Cochrane Database Syst Rev (4): CD001451.
-
Howard FM (2003) The role of laparoscopy in the chronic pelvic pain patient. Clin Obstet Gynecol 46(4): 749-766.
-
Howard FM (2003) Chronic Pelvic Pain. Obstet Gynecol 101: 594-611.
-
Hebbar S, Chawla C (2005) Role of laparoscopy in evaluation of chronic pelvic pain. J Minim Access Surg 1(3): 116-120.
- The Need for Partner Education and Mental Health Support During Pregnancy and the Postpartum Period
- Application of Combined PGT-A and PGT-M for Reproductive Management in a Couple Carrying GCDH Mutations with Prior Affected Offspring: A Rare Case Report
- The Effect of Using a New Technique Karman Injector (Elif Technique) on the Healing Process of Wound Infection-Case Series
- GSM: Counseling Points to Discuss with Women Fearful of Vaginal Estrogen
- Antenatal Diagnosis of Meckel Syndrome: A Case Report
- Discrimination and Workplace Harassment (Mobbing) against Women in the Post-Pandemic Era