Comparative Evaluation of Fixed Dose Combinations of Fluticasone/ Formoterol and Budesonide/ Formoterol in Patients of Mild- Moderate Bronchial Asthma
The prevalence of asthma is rising worldwide with 10–12% adults and 15% children affected presently. It can have a considerable impact on the quality of life of both, patients and their caregivers. Fixed dose combination of Inhaled corticosteroids (ICS) like fluticasone and budesonide and long acting beta 2 agonists (LABAs) in the form of metered dose inhaler (MDI) are synergistic in action and provide effective control in asthma. Objectives: In the present study, two ICS & LABA combinations i.e. fluticasone/ formoterol and budesonide/ formoterol were compared, both administered through a metered dose inhaler (MDI) with a spacer, for achieving and maintaining asthma control, improving symptoms, pulmonary function tests and quality of life in patients of mild to moderate bronchial asthma. Methods: It was a prospective, open- label, randomized, parallel study conducted for a total duration of 12 weeks. The parameters used to compare the two MDIs at 0, 6 and 12 weeks were: a. Pulmonary function tests – FEV1, PEFR b. Asthma control scoring (according to the GINA definition of "control") c. Standardized Asthma Quality of Life Questionnaire [AQLQ(S)] d. Adverse effect profile Results: By the end of 12 weeks, asthma control was similarly achieved among the two groups except that fluticasone/ formoterol was significantly better than budesonide/ formoterol in reducing the need for rescue bronchodilator use (p= 0.000) and in improving daytime symptoms at 6 weeks (p=0.000). Fluticasone/ formoterol at 6 weeks, significantly increased the percent predicted PEFR (p= 0.007) and percent improvement in AQLQ(S) score (p=0.006) in comparison to budesonide/ formoterol. Conclusion: Fixed dose combination MDIs containing fluticasone/ formoterol and budesonide/ formoterol are effective in elevating pulmonary functions, controlling & relieving symptoms and revamping the quality of life in patients of bronchial asthma. Fluticasone/ formoterol were better in providing a more rapid and greater improvement in percent predicted PEFR, controlling daytime symptoms for a longer time and reducing the need for rescue therapy. Both the treatments were well tolerated.
Introduction
Asthma is a chronic disease with recurrent episodes of breathlessness, wheeze, cough and expectoration and is defined as “chronic inflammatory disorder of airways” characterized b [1] airway obstruction that is reversible either spontaneously or with treatment; [2] airway inflammation an [3] airway hyper-responsiveness to a variety of stimuli [1]. Its prevalence is rising worldwide with 10–12% of adults and 15% of children affected presently (more than 300 million people) and it is estimated that 100 million more people may be affected by 2025 [2]. The overall prevalence in India is 2.38%. Female sex, advancing age, urban residence, lower socio- economic status, history of atopy, asthma in a first degree relative and all forms of tobacco smoking are associated with significantly higher odds of having asthma [3]. Asthma can have a considerable impact on the quality of life of patients and their caregivers. The vast economic burden comprises both direct costs, such as emergency care, hospitalizations and medications, and indirect costs, largely driven by absenteeism and reduced productivity [4, 5]. It is diagnosed as reversibility of airflow obstruction in response to inhaled bronchodilator, with spirometer demonstrating a 12% improvement and 200 ml increase in forced expiratory volume in 1 second (FEV1) [6]. The efficacy of inhaled corticosteroids (ICS) in reducing airway inflammation and hyper-responsiveness has led to their widespread use as initial therapy in the treatment of patients with moderate-to-severe asthma, especially those requiring daily beta-2 adrenoceptor agonists [7]. These drugs are highly efficacious in reducing symptoms, frequency and severity of exacerbations and risk of a life- threatening attack. ICSs drastically improve lung function and asthma quality of life (AQLQ) of asthmatic patients [8, 9, 10]. An aerosolized short acting β 2-agonist (SABA) is the bronchodilator of choice as a symptom-reliever in acute, severe asthma and a long acting β 2-agonist (LABA) in combination with inhaled corticosteroid (ICS) is used as disease-controller in chronic asthma [11]. ICS and LABA in conjunction effectively achieve a higher level of asthma control and reduce exacerbations and asthma-related hospitalizations [12, 13] .There is a strong rationale of combining ICS and LABA as they optimize each others’ beneficial actions in the airways. Corticosteroids increase the transcription of beta- 2 receptors which protects against the down-regulation of beta-2 receptors in response to long-term exposure to LABAs. LABAs potentiate the molecular mechanism of corticosteroid actions, with increased nuclear localization of glucocorticoid receptors and a synergistic suppression of inflammatory mediator release [14]. Currently accepted goal of asthma care [15] is to achieve and maintain control of the clinical manifestations for prolonged periods so that patients can prevent most attacks, avoid troublesome symptoms day and night and keep physically active. In the present study, two ICS & LABA combinations i.e. fluticasone/ formoterol and budesonide/ formoterol were compared, both administered through a metered dose inhaler (MDI) with a spacer, for achieving and maintaining asthma control, improving symptoms, quality of life and pulmonary function tests, over 12 weeks in patients of mild to moderate bronchial asthma. The main parameters used to compare the said combination inhalers were: a. Asthma control scoring (according to the GINA definition of "control" b. Pulmonary function tests – FEV1, Peak expiratory flow rate (PEFR) c. Standardized Asthma Quality of Life Questionnaire [AQLQ(S)] d. Adverse effect profile
Material and Methods
Study design
It was a prospective, open- label, randomized, parallel study conducted for a total duration of 12 weeks including one baseline and two follow-up observations. The study was conducted on 80 patients of bronchial asthma attending the outpatient department (OPD) of the Tuberculosis and Respiratory Diseases Hospital attached to the Government Medical College, Amritsar after seeking the approval of the institutional thesis committee and ethics committee. Symptom score of each patient was noted at the beginning of the study and accordingly, the patients with mild to moderate symptoms were included [15].
Inclusion criteria
- Asthmatic patients aged 17- 70 yrs
- Reversibility of airway obstruction (>12% and 200 ml increase in FEV
5. Able to use metered dose inhaler (MDI) with zerostat VT spacer and perform the spirometer as per the study requirement [17]
Exclusion criteria
a) Irreversible airway obstruction b) Chronic Obstructive Pulmonary Disease, Chronic bronchitis, Cor pulmonale c) Patients having steroid dependent asthma d) Tuberculosis – active or old, treated patients e) Ischemic heart disease f) Severe respiratory tract infections g) Contraindications to corticosteroid use, like diabetes mellitus, severe hypertension, ischemic heart disease h) Patients having any other illness thought to affect quality of life adversely i) Current or ex- smokers more than 10 pack years j) Pregnant and lactating mothers
Methodology
The patients were recruited after taking informed consent and randomly divided into two groups A and B. Group A included 40 asthmatic patients who were prescribed fluticasone/ formoterol (125/ 6 microgram per puff) one puff twice daily, administered through an MDI and a spacer device. Group B included 40 asthmatic patients who were to take budesonide/ formoterol (200/ 6 microgram per puff) one puff twice daily, administered through an MDI and a similar spacer device. Detailed history of atopy, allergy, smoking, and number of acute exacerbations, factors triggering exacerbations, family & occupational history was taken for each patient. Quarries were made to rule out any cardiac diseases, hypertension, diabetes or any previous history of intolerance or allergy to inhaled steroids and beta agonists. Every patient was subjected to X- ray chest PA view. Asthmatic patients either had a normal X-ray or showed bronchovascular prominence or hyperinflation during an attack. Pulmonary function tests were performed in each case at start of the study, at 6 weeks and 12 weeks which included: 1. FEV1 (Forced expiratory volume in 1 second) 2. PEFR (Peak expiratory flow rate) Percentage reversibility in FEV1 was calculated by repeating the FEV1 ten minutes after inhalation of 2 puffs of salbutamol (100 microgram/ puff) by using the i. Totally limited ii. Extremely limited iii. Very limited iv. Moderate limitation v. Some limitation vi. A little limitation vii. Not at all limited The patients were instructed about the correct use and maintenance of metered dose inhaler (MDI) with zero stat spacer device, [21] and were advised to take care of oral hygiene. They were asked to keep a diary record of symptom severity and the frequency of rescue salbutamol puffs used. They were allowed to take as many salbutamol puffs as demanded by their symptoms along with daily dose of fluticasone/ formoterol or budesonide/ formoterol. They were asked to come for follow-up daily for first 1 week and then weekly for the next 12 weeks. On each follow-up visit, symptom history was taken, physical examination done, PEFR, FEV1 measured and [AQLS (S)] was administered. Any side effects of the drugs were noted. Patients who deteriorated or had acute severe attacks were managed accordingly and dropped from the formula: (Post bronchodilation FEV1)–(Pre bronchodilation FEV1) X 100 Pre bronchodilation FEV1 These tests were done using a computerized spirometer ‘Spirolab 2’ [18] which also gave the predicted values of FEV1 and PEFR of each patient depending on their height, weight, age, sex and environmental temperature [19]. Levels of asthma control over 0, 6 and 12 weeks were assessed and graded into controlled, partly controlled and uncontrolled according to the criteria given by GINA 2011 [15]. Patients were also administered an interview based Standardized Asthma Quality of Life Questionnaire [AQLS (S)] at the baseline visit, 6 weeks and 12 weeks. The questionnaire was available in English, Hindi and Punjabi. For illiterate patients, questions were explained verbally and after being convinced that the patient understood the meaning of the question put to him, the response was recorded. Questions were asked in the order specified in the questionnaire. There was no advice, suggestion or encouragement from the interviewer’s side to the patient. [AQLQ(S)] is a structured disease specific quality of life questionnaire developed to measure the functional (physical, social and emotional) problems that trouble the patients of asthma. It contains in total 32 items that measure four domains of health i.e. symptoms, emotional function, effect of environmental stimuli and activity limitation [20]. All responses were recorded on a scale of 1 to 7 and score of each domain was expressed as a mean of score given to each item. Overall quality of life was assessed from mean score of all domains and graded into 7 levels of severity as follows:
study. Those suffering mild exacerbations were continued to be a part of the study and the number of exacerbations was noted in each patient. At the end of the study, the entire data was compiled, tabulated and analyzed statistically using Student‘t’ test and Chi square test.
Results
The two treatment groups were well-matched with respect to all key demographic characteristics and other variables at baseline as shown in Table 1.
| Baseline | Fluticasone/ | Budesonide/ | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p value | ||||||||||||||
| Characteristics | Formoterol | Formoterol | ||||||||||||
| 1. | Number of patients | 40 | 40 | - | ||||||||||
| 2. | Sex Male- n (%) | 23 (57.5) | 23 (57.5) | - | ||||||||||
| Female- n (%) | 17 (42.5) | 17 (42.5) | - | |||||||||||
| 3. | Age in years (Mean ±SD) | 40.50 ± 14.85 | 37.73 ± 15.33 | 0.41 | ||||||||||
| 4. | Duration of asthma in years (Mean ±SD) | 20. 23 ± 13.61 | 18.05 ± 11.89 | 0.45 | ||||||||||
| 5. | History of atopy- n (%) | 22 (55) | 18 (45) | 0.37 | ||||||||||
| 6. | Family history of asthma- n (%) | 18 (45) | 11 (27.5) | 0.10 | ||||||||||
| 7. | Patients hospitalized at least once during the last year- n (%) | 29 (72.5) | 26 (65) | 0.47 | ||||||||||
| 8. | No of exacerbations in the last year (Mean ± SD) | 1.40 ± 0.71 | 1.45 ± 0.85 | 0.78 | ||||||||||
| 9. | Socioeconomic status High- n (%) | 5 (12.5) | 2 (5) | 0.36 | ||||||||||
| Average- n (%) | 9 (22.5) | 13 (32.5) | ||||||||||||
| Low- n (%) | 26 (65) | 25 (62.5) | ||||||||||||
| 10. | FEV1 at baseline (Mean ± SD) | 1.12 ± 0.47 | 1.09 ± 0.47 | 0.72 | ||||||||||
| 11. | PEFR at baseline (Mean ± SD) | 4.04 ± 1.75 | 3.67 ± 1.92 | 0.37 |
Table 1: Patient characteristics at baseline.
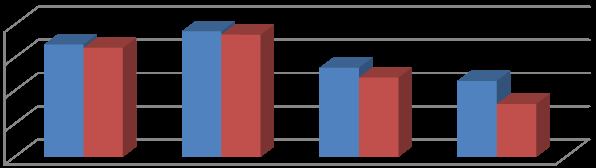
History revealed that an acute exacerbation of asthma was triggered by multiple factors and most patients had exacerbations due to more than one trigger. The common factors were as shown in Figure 1.
Fluticasone/ Formoterol (n=40)
Budesonide/ Formoterol (n=40)
0 10 20 30 40 34 38
27 23 33 37
Pulmonary function tests improved over baseline values and percent predicted values in both treatment groups during the course of the study and this change was highly significant (p= 0.000). The inter-group differences in FEV1 and PEFR change from baseline was not statistically significant as depicted in table 2.
| Fluticasone/ | Budesonide/ | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| t value | p value | ||||||||||||
| Formoterol | Formoterol | ||||||||||||
| FEV1 | At day 0 | 1.12 ± 0.47 | 1.09 ± 0.47 | 0.36 | 0.72 | ||||||||
| At 6 weeks | 1.93 ± 0.57 | 1.89 ± 0.57 | 0.32 | 0.75 | |||||||||
| At 12 weeks | 2.42 ± 0.65 | 2.48 ± 0.61 | 0.42 | 0.68 | |||||||||
| PEFR | At day 0 | 4.04 ± 1.75 | 3.67 ± 1.92 | 0.91 | 0.37 | ||||||||
| At 6 weeks | 6.47 ± 1.73 | 5.99 ± 1.98 | 1.16 | 0.25 | |||||||||
| At 12 weeks | 6.75 ± 1.84 | 6.83 ± 1.55 | 0.22 | 0.82 | |||||||||
| p values > 0.05 = Not significant |
Table 2: Inter group comparison of change in FEV1 and PEFR from baseline.
Over the 12 weeks duration, groups a (fluticasone/ formoterol) and group B (budesonide/ formoterol) were compared with respect to 5 domains of asthma control scoring (Table 3).
| Fluticasone/ | Budesonide/ | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control of | Time | Formoterol | Formoterol | p value | ||||||||||
| (n = 40) | (n = 40) | |||||||||||||
| Daytime symptom | At day 0 | 22 (55%) | 18 (45%) | 0.37 | ||||||||||
| At 6 wk | 40 (100%) | 29 (72.5%) | 0.000* | |||||||||||
| At 12 wk | 40 (100%) | 40 (100%) | - | |||||||||||
| Limitation of activities | At day 0 | 32 (80%) | 27 (67.5%) | 0.20 | ||||||||||
| At 6 wk | 39 (97.5%) | 35 (87.5%) | 0.09 | |||||||||||
| At 12 wk | 39 (97.5%) | 40 (100%) | 0.31 | |||||||||||
| Nocturnal symptoms | At day 0 | 16 (40%) | 22 (55%) | 0.18 | ||||||||||
| At 6 wk | 22 (55%) | 39 (97.5%) | 0.000* | |||||||||||
| At 12 wk | 39 (97.5%) | 40 (100%) | 0.31 | |||||||||||
| Need for rescue therapy | At day 0 | 25 (62.5%) | 22 (55%) | 0.49 | ||||||||||
| At 6 wk | 35 (87.5%) | 24 (60%) | 0.005* | |||||||||||
| At 12 wk | 40 (100%) | 40 (100%) | - | |||||||||||
| Lung function | At day 0 | 1 (2.5%) | 1 (2.5%) | 1.00 | ||||||||||
| At 6 wk | 36 (90%) | 32 (80%) | 0.21 | |||||||||||
| At 12 wk | 39 (97.5%) | 39 (97.5%) | 1.00 | |||||||||||
| *p value < 0.01 = Highly significant |
Table 3: Comparison of asthma control between 2 groups.
During the treatment period, the number of additional salbutamol puffs (rescue bronchodilator) taken by the patient were noted as given in Table 4.
No. of patients in
No. of
Fluticasone/
Salbutamol
Formoterol group
puffs used (n=40) 4 5 0 5 (6.3%)
6 23 0 23 (28.7%) 7 1 0 1 (1.3%)
8 8 4 12 (15%) 10 2 6 8 (10%)
12 1 16 17 (21.3%) No. of patients in Budesonide/
Total
Formoterol group
(n=40)
| 14 | 0 | 8 | 8 (10%) |
|---|---|---|---|
| 16 | 0 | 5 | 5 (6.3%) |
| 18 | 0 | 1 | 1 (1.3%) |
Table 4: Patients using rescue bronchodilator during treatment Mean number of salbutamol puffs used by group A (fluticasone/ form
Table 4: Patients using rescue bronchodilator during treatment Mean number of salbutamol puffs used by group A (fluticasone/ formoterol) and group B (budesonide/ formoterol) was 6.53 ± 1.68 and 12.35 ± 2.43 respectively and this difference was highly significant (p= 0.000). Mean AQLQ(S) scores divided into four domains (symptoms, activity limitation, emotional function and environmental stimuli) were compared between the two groups. Both combinations i.e. fluticasone/ formoterol and budesonide/ formoterol significantly improved (p= 0.000) all the domain scores throughout the study period. There was no significant difference in score improvement between the two groups except for emotional function, which improved significantly in fluticasone/ formoterol group (p=0.029) at 6 weeks (Table 5).
| Fluticasone/ | Budesonide/ | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Formoterol | Formoterol | ‘t’ | |||||||||||||||
| DOMAINS | Time | p value | |||||||||||||||
| Mean ± SD | Mean ± SD | value | |||||||||||||||
| Symptom score | At day 0 | 44.33 ± 6.3 | 45.05 ± 6.5 | 0.50 | 0.61 | ||||||||||||
| At 6 wk | 65.1 ± 4.6 | 63.30 ± 5.6 | 1.57 | 0.12 | |||||||||||||
| At 12 wk | 73 ± 5 | 73.5 ± 5.8 | 0.41 | 0.68 | |||||||||||||
| Activity limitation | At day 0 | 42 ± 4.8 | 43.75 ± 4.29 | 1.15 | 0.25 | ||||||||||||
| At 6 wk | 59 ± 4.07 | 57.73 ± 4.66 | 1.30 | 0.19 | |||||||||||||
| At 12 wk | 65.38 ± 4.16 | 65 ± 4.55 | 0.39 | 0.70 | |||||||||||||
| Emotional function | At day 0 | 20.40 ± 2.63 | 21.15 ± 2.35 | 1.35 | 0.18 | ||||||||||||
| At 6 wk | 27.75 ± 1.88 | 26.63 ± 2.6 | 2.22 | 0.029* | |||||||||||||
| At 12 wk | 30.70± 2.52 | 29.8 ± 2.33 | 1.66 | 0.10 | |||||||||||||
| Environment al stimuli | At day 0 | 11.5 ± 1.85 | 11.95 ± 2.48 | 0.92 | 0.36 | ||||||||||||
| At 6 wk | 19.45 ± 2.1 | 18.95 ± 2.17 | 1.05 | 0.29 | |||||||||||||
| At 12 wk | 22.55 ± 1.66 | 22.33 ± 2.07 | 0.54 | 0.59 | |||||||||||||
| *p value < 0.05 = Significant |
Table 5: Inter-group comparison of mean AQLQ(S) domain scores.
Mean total AQLQ(S) score for group a (fluticasone/ formoterol) was 118 ± 12.1 at baseline that improved to 191 ± 12.29 at the end of the study. For group B (budesonide/ formoterol) this value increased from 121 ± 10.58 at baseline to 190 ± 13.15 at 12 weeks. There was no significant difference in total scores of groups A and B at any time of the study [p= 0.08 (6 weeks); p= 0.73 (12 weeks)].
Percent improvement in quality of life at 6 weeks and 12 weeks was also compared between the two groups. For group A (fluticasone/ formoterol), AQLQ(S) score increased by 45.38 ± 14.97 percent and for group B (budesonide/ formoterol), it increased by 37.16 ± 10.56 percent at 6 weeks. This difference among the two groups was statistically significant (p value < 0.05). At the end of 12 weeks quality of life increased by 62.95 ± 20.11
percent for group A and 57.02 ± 12.06 percent for group B. But this difference was not significant statistically. There was no significant difference in adverse effect profile between the two groups. In fluticasone/ formoterol group, 2 patients suffered from sore throat, 3 from hoarseness of voice, 1 had or pharyngeal candidacies and 2 had upper respiratory tract infection. In budesonide/ formoterol group, 2, 1, 1 and 3 patients suffered these adverse effects respectively.
Discussion
Comparison between the two groups on the basis of improvement in pulmonary function tests (FEV1 and PEFR) demonstrated no significant change at the end of the study period as depicted in previous studies. [22, 23] In concordance with past studies, fluticasone/ formoterol provided a more rapid and greater improvement in percent predicted PEFR [24, 25]. Symptom control was achieved by most patients at the end of the study. Significant differences were seen at 6 weeks, when nocturnal symptoms were better controlled in budesonide/ formoterol and a higher control was seen in fluticasone/ formoterol in terms of daytime symptoms and need for rescue therapy analogous to the results of another study [26]. During the course of therapy, the average number of rescue bronchodilator puffs (salbutamol 200 mcg per puff) required by patients in fluticasone/ formoterol group was significantly lower than that for budesonide/ formoterol group. Therefore fluticasone/ formoterol was better in controlling asthma symptoms for a longer time as recorded by a double – blind, randomized, parallel study where percent days without the use of additional bronchodilator was significantly more in fluticasone/ formoterol group as compared to budesonide/ formoterol group [27]. AQLQ(S) scoring did not differ significantly between the two groups, except for the emotional function at 6 weeks, which improved more in fluticasone/ formoterol group. Also the overall percent improvement at 6 weeks was higher with fluticasone than with budesonide. In a similar study done previously, there were significant treatment differences in favor of fluticasone in three of the four domains - activity limitations, symptoms, and emotional function [28]. Both the treatments were well tolerated and there was no significant difference in incidence of side effects between them.
Conclusion
This study concludes that fixed dose combinations MDIs containing fluticasone/ formoterol and budesonide/ formoterol are very effective in elevating pulmonary functions, controlling & relieving symptoms and revamping the quality of life in patients of bronchial asthma. Fluticasone/ formoterol were better in providing a more rapid and greater improvement in percent predicted PEFR, in controlling daytime symptoms for a longer time and reducing the need for rescue therapy.
References
-
[INLINE_TABLE:7:0] [INLINE_TABLE:8:0] respiratory inhalers to hospitalized patients with asthma or COPD: a randomized trial. J Gen Intern Med 27(10): 1317-1325.
-
Gogtay JA, Balki A, Dalal S, Singh A, Bardapurkar S, et al. (2010) Efficacy and tolerability of a new HFA- Propelled fluticasone/formoterol combination inhaler compared to budesonide/formoterol combination in subjects with moderate to persistent asthma. Chest 138(4): 161.
-
Derom E, Schoor JV, Verhaeghe W, Vincken W, Pauwels R (1999) Systemic Effects of inhaled fluticasone propionate and budesonide in adult patients with asthma. Am j respir crit care med 160(1): 157-161.
-
Ayres JG, Bateman ED, Lundbäck B, Harris TAJ (1995) High dose fluticasone propionate, 1 mg daily versus fluticasone propionate, 2 mg daily or budesonide, 1.6 mg daily in patients with chronic severe asthma. Eur Respir J 8(4): 579-586.
-
Hoekx JCM, Hedlin G, Pedersen W, Sorva R, Hollingworth K, et al. (1996) Fluticasone propionate compared with budesonide: A double-blind trial in asthmatic children using powder devices at a dosage of 400 mcg per day. Eur Respir J 9(11): 2263-2272.
-
Adams NP, Lasserson TJ, Cates CJ, Jones P (2007) Fluticasone versus beclomethasone or budesonide for chronic asthma in adults and children. Cochrane Database Syst Rev 17(4): CD002310.
-
Ringdal N, Swinburn P, Backman R, Plaschke P, Sips AP, et al. (1996)A blinded comparison of fluticasone propionate with budesonide via powder devices in adult patients with moderate-to-severe asthma: a clinical evaluation. Mediators of Inflammation 5(5): 382-389.
-
Rutherford C, Mills R, Gibson PG, Price MJ (2003)
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index