May-Thurner Syndrome: A Case Report and Review of Anesthetic Management
May-Thurner syndrome (MTS) is a rare vascular variant that the left common iliac vein (LCIV) is compressed by the right common iliac artery. The compression may block the venous blood flow due to stenos is of the LCIV lumen, and cause thrombosis formation. Although the compression may be asymptomatic, it may develop swelling, pain and deep vein thrombosis (DVT) of the left lower extremity. However, the anesthetic management of the MTS has not well been reported. Here we describe a case of MTS patient who had an orthopedic surgery, and review the anesthetic management of MTS. Our anesthetic management mainly focused on preventing DVT or pulmonary Thromboembolism.
Jun Ho Lee1,2, Seonwoo Yoo1, Minjong Ki1, Deokkyu Kim1 and Sang-
Kyi Lee1*
Medical School and Hospital, Jeonju, Korea
250-1240; Email: leesk@jbnu.ac.kr
Our anesthetic management mainly focused on preventing DVT or pulmonary Thromboembolism.
Keywords: Common iliac vein; Deep vein thrombosis; May-Thurner syndrome
Introduction
Deep vein thrombosis (DVT) is one of the most fatal conditions in anesthetic management. Anesthesiologists are familiar with the factors that cause DVT such as immobility, prolonged bed rest, pregnancy, obesity, and vasculitis, etc. Of them all, there is a vessel related disease called May-Thurner syndrome (MTS). Here we describe a case of MTS patient who had an orthopedic surgery and review of anesthetic management. Plenty of case reports of MTS are reported to the world, but not many anesthetic management of MTS has been reported. May and Thurner described a rare vascular anatomic variant that the left common iliac vein (LCIV) is compressed by the right common iliac artery (RCIA) in 1957 [1]. This anatomical variant that the RCIA overlies the LCIV has been called May-Thurner syndrome (MTS), which blocks the blood flow and causes repeated thrombosis formation. Although the prevalence of MTS is unknown, it occurs in 2–5% of patients undergoing evaluation for lower extremity venous disorder [2]. MTS is somewhat related to DVT considering the fact that DVT is more commonly involved in the left popliteal or femoral vein than the right side [3]. The compression of the LCIV may be asymptomatic, and may be found incidentally in most case. However, some patients complain edema and severe calf pain with flexion of the lower extremity as Cockett, et al. reported [4]. Also, repetitive DVT can be induced by the thrombosis formation due to the compression of the iliac vein. The venous compression can cause thickening of the inner wall of the vein, and induces intimal hyperplasia [5]. It is often found in female patients between their twenties and forties with the thrombogenic state of pregnancy [3]. MTS is notable for anesthesiologists because the common cause of pulmonary Thromboembolism (PTE) is DVT. It is rare but serious complication in the perioperative period. We report a female MTS patient who had an arthroscopic subacromial decompression and debridement on her shoulder. Also, the anesthetic management is reviewed for the MTS patients.
Case Report
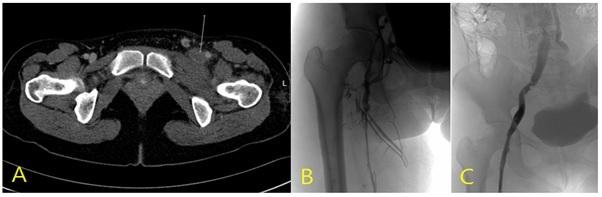
A 36-year-old female (151 cm, 49 kg) was admitted to our orthopedic department for the scheduled arthroscopic subacromial decompression and debridement on her right shoulder due to synovitis and partial tear of rotator cuff. Six years ago, the patient had been diagnosed MTS five days after normal vaginal delivery. Complete obstruction of the LCIV and acute thrombosis of the left lower leg vein was found by computerized tomography (CT) and venogram so that mechanical thrombectomy and stent insertion were performed (Figure 1). Inferior Vena Cava (IVC) filter was inserted to prevent the risk of PTE. Anticoagulation was started with warfarin, and maintained for 5 months.
of DVT and specific problems were not found in sonography, the operation was preceded without pre- treatment in preoperative period except the switch of anticoagulation to low molecular weight heparin. The past history including anticoagulant therapy was briefly summarized in Table 1.
| 6 years ago | - Left leg pain and swelling, 5 days after Vaginal Delivery diagnosed as May-Thurner Syndrome by CT scan - Complete obstruction of the LCIV* and acute thrombosis (Figs. 1A and 1B) LCIV* thrombectomy & stent insertion (Fig. 1C) and systemic heparinization - Infrarenal IVC filter insertion to prevent PTE† |
|---|---|
| Warfarinization for 5 months and stop. | |
| 1 year ago | - Right leg pain and swelling, 4 days after Vaginal Delivery. ribaroxaban Thrombosysis & thrombectomy. |
| - Aspirin and ribaroxaban for 6 months | |
| 6 months ago | - Stop ribaroxaban and maintain Aspirin - Thrombi were not found and venous flow was normal by sonography and CT |
| 2 weeks ago | - Aspirin was held. - Preoperative lab: Hb 13.4 mg/dl, PT INR 0.97, aPTT 27.9 - ECG, Chest PA, Echocardiogram: Non-specific |
Table 1: Past history of the Patient. Preoperative laboratory tests were within normal range including hemoglobin 13.4 mg/dl, Pro
Table 1: Past history of the Patient. Preoperative laboratory tests were within normal range including hemoglobin 13.4 mg/dl, Prothrombin Time International Normalized Ratio (INR) 0.97 and activated partial thromboplastin time (aPTT) 27.9 second. Also, chest PA, electrocardiography (ECG) and echochardiogram presented non-specific. After arriving at the operating room, ECG, blood pressure, pulse oximetry, bispectral index scale (BIS) and a peripheral nerve stimulator (TOF watch®, Organon Ltd., Dublin, Ireland) were monitored. Initial vital sign was blood pressure 130/78 mmHg, heart rate 90 /min, respiratory rate 18 /min, Oxygen saturation 97%. Before anesthesia induction, pneumatic compression device was applied, and lidocaine 75 mg and dexamethasone 5 mg was administered intravenously. General anesthesia was induced by propofol (80mg) and remifentanil (6ng/ml target controled infusion), and rocuronium (50mg). Anesthesia was maintained with desflurane and remifentanil to sustain BIS values 40–60. Orotracheal intubation was performed at 3 minutes after loss of consciousness without any difficulty when train-of-four count was 0, and effect-site concentration of remifentanil was maintained at the steady-state levels, 3–3.5 ng/ml. Controlled mechanical ventilation was maintained with a TV 8 ml/kg and an inspiratory to expiratory ratio 1: 2 without PEEP. The ventilatory frequency was set to keep the end-tidal PCO2 range of 34–38 mmHg. Cuff pressure of the endotracheal tube was monitored, and the pressure was maintained in between 20–25 cm H2O. Nasopharyangeal temperature was monitored and the patient was actively warmed to keep the body temperature 36.0–36.5℃ by using a forced air warming unit and a fluid line warmer.
The duration of the operation was 77 minutes. The amount of bleeding was trivial, and the amount of fluid was about 700 ml crystalloid during the period of the operation. The regimen of patient controlled analgesia was morphine 40 mg and ketorolac 150 mg in total 60 ml solution. The operation was done without any complication. After the surgery, muscle relaxant was reversed with neostigmine (2 mg) and glycopyrrolate (0.4 mg). After checking spontaneous breathing, return of consciousness and TOF ratio more than 0.9, the patient was extubated and transferred to post-anesthesia care unit. The postoperative laboratory tests were unchanged including hemoglobin 12.5 mg/dl, Prothrombin Time INR 1.05 and aPTT 29.9 second. The patient was ambulated as early as possible with wearing high elastic stockings, and aspirin was re-administered. In the postoperative lower extremity CT, IVC filter and LCIV stent was intact, DVT was not found. The patient was discharged without an event.
Discussion
This case covers a report of a patient who had been diagnosed with MTS and receiving medication to prevent repeated DVT and its anesthetic management review. Although the patient was fortunate to have no particular problem with anesthesia and operation, anesthesiologists should always be alert when manage high risk patients of DVT.MTS is a rare vascular variant that the LCIV is compressed by the RCIA [1]. Due to the compression of the iliac vein, venous flow is decreased, and formation of thrombosis is promoted [4]. Endothelial irritation and spur formation in the LCIV resulting from persistent compression and pulsating stimulus of the RCIV may be the cause of sluggish venous flow [3]. Although the prevalence of MTS has not well known, in a study, up to 5% of patients to evaluate lower extremity venous disorder have MTS [6]. The clinical manifestation of MTS is left leg edema, pain, sensation of thigh tightness, venous stasis, and claudication with thrombi. Majority of the cases are female patients aged 20s to 40s [5]. The thrombus formation of the syndrome is related to pregnancy, surgery and immobilization. Sudden onset of the left lower extremity swelling after persistent immobilization is more frequent [7]. In this case, MTS was first diagnosed at the age of 30 after vaginal delivery with sudden onset. MTS can be diagnosed with contrast venography that presents narrowing lesions and spurs at the pelvic brim level [2]. Complete obstruction of the LCIV and its collateral vasculature can be easily detected in venogram as our case (Figure 1B). The key to MTS management is anticoagulation therapy and large vessel patency. Heparin therapy is commonly used for anticoagulation to achieve the target aPTT 1.5– 2.4 times normal. Warfarin is concurrently used with heparin therapy, and prothrombin time INR are generally within the therapeutic range, 2.0–3.0. Anticoagulation is a traditional therapy for DVT, but surgical correction such as thrombectomy, thrombolysis or endovascular stent placement is required because anticoagulation may not be very effective alone [8]. IVC filters may be considered if there are free-floating clots to prevent PTE [9]. Our patient received warfarin for 6 months along with thrombectomy and stent insertion. Also IVC filter was executed in the consideration for the risk of PTE. Warfarin was switched to aspirin until 2 weeks before surgery. There is no specific guideline for the perioperative management with MTS or iliofemoral DVT. The therapeutic goal is to prevent PTE resulting from the formation of DVT prior to surgery. In general the use of anticoagulation should be continued if the patient has high risk of thrombosis. It is tough to decide whether antiplatelet is held or bridging is required. However, the operation was arthroscopic surgery, and the surgeon wanted clear view. Even if aspirin is stopped before surgery, it usually held a week before the surgery. Our patient stopped aspirin 2 weeks before the surgery due to her operational schedule and the result of preoperative imaging studies showing no evidence of DVT. LMWH was administered instead of aspirin. Anticoagulation is one of the most important methods of prevention of DVT or PTE. Anticoagulation should be restarted as soon as the operation was done. The patient resumed aspirin a day after surgery in our case. Utilizing high elastic stockings or pneumatic compression of the legs may decrease the risk of venous thrombosis [10]. Intermittent pneumatic compression device was used throughout the operation. Postoperative early ambulation with high elastic stocking would be helpful to prevent PTE. Also, fluid should be warmed to avoid hypothermia [7]. In this case, we tried to keep the patient’s body temperature more than 36℃. Also, we hydrate adequately to lower the viscosity of the blood as possible. Because sudden hypoxemia is presented when intraoperative pulmonary embolism occurs, a decrease in end-tidal CO2 concentration is a very reliable clinical finding. Therefore, end-tidal CO2 was monitored and maintained within normocapnic state in this case. In addition, the authors made an effort on keeping the adequate depth of anesthesia and muscle relaxation by using BIS and TOF monitoring. The choice of anesthetics may affect the coagulability or bleeding time although the effect is clinically somewhat questionable. Among the inhaled anesthetics, halothane has been known to have a property that inhibits platelet aggregation and increases bleeding time. However, desflurane also inhibits platelet function similar to halothane in an in vitro study [11]. Propofol has an effect on inhibiting human platelet aggregation and intracellular calcium increases induced by proinflammatory lipid mediators [12]. In a study that compared propofol- remifentanil total intravenous anesthesia with sevoflurane on platelet function, propofol and remifentanil significantly diminished collagen induced platelet aggregation, while sevoflurane did not [13]. Dexamethasone affected platelet aggregation and fibrinolytic activity, but therapeutic lidocaine concentrations had no effect on platelet function [14]. In this case, dexamethasone and lidocaine were administered before induction, and balanced and general anesthesia was maintained with desflurane and remifentanil. Lidocaine use seems not to be related with coagulability, but it reduces the injection pain. Plasma D-dimer is a marker of cross-linked fibrin degradation products, and it is useful to diagnose DVT. Activated clotting time (ACT) monitors the effect of heparin and is well correlated with aPTT. Although D- dimer or ACT was not measured in this case, we struggle to monitor as thorough as possible to detect the signs of PTE. Moreover, the postoperative pain was actively managed in this case, because surgical stress and pain provokes catecholamine release, leading to increased coagulability [15]. The patient was ambulated early with high elastic stockings.In summary, anticoagulation, intraoperative monitoring of signs of PTE, maintenance of body temperature, use of elastic stockings, adequate management of anesthesia, adequate choice of anesthetics, adequate control of anesthetic depth and pain, prevention of PTE should be considered when MTS patients are anesthetized.
Acknowledgment
This case report was supported by funds from the Biomedical Research Institute of Chonbuk National University Hospital, Jeonju, South Korea.
References
-
May R, Thurner J (1957) the cause of the predominantly sinistral occurrence of thrombosis of the pelvic veins. Angiology 8(5): 419-427.
-
Cil BE, Akpinar E, Karcaaltincaba M, Akinci D (2004) Case 76: May-Thurner syndrome. Radiology 233(2): 361-365.
-
Zander KD, Staat B, Galan H (2008) May-Thurner Syndrome resulting in acute iliofemoral deep vein thrombosis in the postpartum period. Obstet Gynecol 111(2): 565-569.
-
Cockett FB, Thomas ML (1965) The iliac compression syndrome. Br J Surg 52(10): 816-821.
-
Loukas M, Shah R, Esmaeili E, Bangeholm A, Tubbs RS, et al. (2008) A case of May-Thurner syndrome. Folia Morphol (Warsz) 67: 214-217.
-
Delis KT, Bountouroglou D, Mansfield AO (2004) venous claudication in iliofemoral thrombosis: long- term effects on venous hemodynamics, clinical status, and quality of life. Ann Surg 239(1): 118-126.
-
Lee SK, Choi EJ, Kim KI, Kim YM, Choi H, et al. (2008) Perioperative Management for the Patient with May- Thurner Syndrome: A Case Report. Korean J Crit Care Med 23: 115-119.
-
Grunwald MR, Goldberg MJ, Hofmann LV (2004) Endovascular management of May-Thurner syndrome. AJR Am J Roentgenol 183(5): 1523-1524.
-
Acharya G, Singh K, Hansen JB, Kumar S, Maltau JM (2005) Catheter-directed thrombolysis for the management of postpartum deep venous thrombosis. Acta Obstet Gynecol Scand 84(2): 155-158.
-
Cayley WE (2007) Preventing deep vein thrombosis in hospital inpatients. 335: 147-151.
-
Berlet T, Krah A, Börner U, Gathof BS (2003) Desflurane inhibits platelet function in vitro similar to halothane. Eur J Anaesthesiol 20(11): 878-883.
-
Fourcade O, Simon M, Litt L, Samii K, Chap H (2004) Propofol inhibits human platelet aggregation induced by proinflammatory lipid mediators. Anesth Analg 99(2): 393-398.
-
Son SC, Lee WH, Lee JH, Lee JH, Cho HY, Shin YS (2008) The effects of propofol-remifentanil total intravenous anesthesia on platelet function. Korean J Anesthesiol 54(2): 134-138.
-
Van Giezen JJ, Brakkee JG, Dreteler GH, Bouma BN, Jansen JW (1994) Dexamethasone affects platelet aggregation and fibrinolytic activity in rats at different doses which is reflected by their effect on arterial thrombosis. Blood Coagul Fibrinolysis 5(2): 249-255.
-
Kohro S, Yamakage M, Arakawa J, Kotaki M, Omote T, et al. (1998) Surgical/tourniquet pain accelerates blood coagulability but not fibrinolysis. Br J Anaesth 80(4): 460-463.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index