Propofol for Conscious Sedation for Fibreoptic Nasotracheal Intubation: Comparison with Fentanyl-Midazolam Combination
The safest way of doing fibreoptic intubation is with the patient under conscious sedation and maintaining spontaneous respiration. Short acting and easily titrable analgesics are excellent choices for the intensely , but usually brief airway manipulation during fibreoptic nasotracheal intubation .This study was undertaken to evaluate the efficacy of propofol for conscious sedation for FOI and to compare it with a combination of fentanyl and midazolam which is frequently used for this purpose. The parameters studied were, the quality of sedation, intubating conditions, haemodynamic changes, degree of amnesia and global acceptance of the procedure under topical anaesthesia. In our study, we found that in the doses used by us, propofol produced comparable intubating conditions as a combination of midazolam and fentanyl. It produced significantly more sedation but difference between the two groups was significant only at 2 minutes (p value=0.028). Propofol leads to less increase in heart rate when the fiberscope was inserted endotracheally (P value=.007) .As the procedure progressed more boluses of propofol were needed to continue with the procedure. The degree of amnesia for the procedure was less with propofol however; the degree of global acceptance was comparable. To conclude propofol can be used for nasotracheal fibreoptic intubation, however its role in difficult airway and the dose required need more evaluation.
KN Saxena* and N Chopra
Associated Lok Nayak Hospital, India
Anesthesiology & Intensive care, Maulana Azad Medical College & Associated Lok Nayak required need more evaluation.
Keywords: Fibreoptic intubation; Conscious sedation; Propofol; Nasotracheal FOI
Introduction
Awake fibreoptic intubation is an established method of securing a difficult airway [1, 2]. The safest way of doing it is with the patient under conscious sedation and maintaining spontaneous respiration At the same time airway reflexes and haemodynamic changes associated with it also need to be obtunded [1]. The quality and success of this procedure depends on the experience of the intubating physician and the proper preparation of the patient [2]. Short acting and easily titrable analgesics are excellent choices for the intensely, but usually brief airway manipulation during fibreoptic nasotracheal intubation [1]. Fentanyl and midazolam have been used successfully for fibreoptic intubation (FOI) [2, 3]. Propofol has not been evaluation for conscious sedation for nasotracheal intubation but has attributes that make it an ideal sedating agent in sub anaesthetic doses. It produces reliable and predictable sedation, maintenance of haemodynamic stability and profound amnesia [3] making it useful for sedation in ICU and surgery under regional anaesthesia. Propofol has been used for fibreoptic bronchoscope under conscious sedation [4, 5, 6]. It has also been used for FOI for induction of general anaesthesia for this purpose [7, 8] and light general anesthesia [9]. It has also been used for this purpose as a target controlled infusion for oral FOI [10, 11, 12]. This study was undertaken to evaluate the efficacy of propofol for conscious sedation for nasotracheal FOI and to compare it with a combination of fentanyl and midazolam which is frequently used for this purpose. The parameters studied were, the quality of sedation, intubating conditions, haemodynamic changes, degree of amnesia and global acceptance of the procedure under topical anaesthesia.
Material and Methods
After approval by the institutional ethics committee, this prospective randomized study was undertaken in 40, patients of either sex, scheduled to undergo routine surgery in our hospital. All the patients had undergone pre-anaesthetic checkup and those in ASA grade I and II, not having repiratory, cardiovascular, liver or kidney disease were included. Also excluded were those with history of drug abuse and airway difficulty as assessed by Mallampatti grading (III, IV), thyromental distance (<6cm), airway tumours or previous airway surgery and obesity (BMI>30) an informed written consent was taken and all the patients were educated about the fibreoptic Group P- A bolus of 1mg/kg body weight propofol was followed by infusion at the rate of 1 mg/kg/hr for maintenance with a syringe infusion pump. Group F- Boluses of midazolam 0.05 mg/kg and fentanyl 1μg/kg body weight were followed by fentanyl infusion at the rate of 1 μg/kg/hr with a syringe infusion pump. The degree of sedation was assessed 60 seconds after medication and every 2 minutes during airway manipulation using ‘Observer’s Assessment of Alertness/Sedation scale [1] (Table 1).
intubation procedure. They were randomized by computer generated numbers into two groups: group P (n=20) and group F (n=20) receiving sedation with propofol or a combination of fentanyl and midazolam respectively.
In the operation theatre, routine monitors were attached (spO2, ECG, NIBP) and the patient’s basal vital parameters (pulse rate, blood pressure, arterial oxygen saturation) were noted and thereafter continuously recorded. An intravenous line was secured with an 18G intracath and the patients were premeditated with glycopyrrolate 0.2 mg I.V. 15 minutes before the start of surgery. Every patient received topical anaesthesia of the airway structures as per a standard protocol-3 drops of vasoconstrictor (xylometazoline) were instilled in each nostril followed by application of 2-3 puffs of lignocaine 10% spray (Astra-xylocaine 10% spray with nasal applicator) to the nasal mucosa. Thereafter, the patient was asked to protrude his tongue and lignocaine 10% was sprayed (2 puffs on the posterior pharyngeal wall and 2 puffs each on the 2 tonsillar pillars. Oxygenation was achieved by nasal catheter in the nostril with flow rate of 2 L/min. The fibreoptic equipment (Olympus tracheal intubating fiberscope, adult size with outer diameter of 5.2mm, with camera and monitor) was tested before start of procedure.
The Patients then Received the Study Drugs
| Facial | Score | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Responsiveness | Speech | Eyes | ||||||||||||
| expression | level | |||||||||||||
| Respond readily to name Spoken in normal tone | Normal | Normal | Clear No ptosis | 5 (alert) | ||||||||||
| Lethargic response to name spoken in normal tone | Mild slowing or thickening | Mild relaxation | Glazed or mild ptosis (less than ½ the eye) | 4 | ||||||||||
| Responds only after name is called loudly and/or repeatedly | Slurring or prominent slowing | Marked relaxation (Slack jaw) | Glazed and marked ptosis (1/2 the eye or more) | 3 | ||||||||||
| Responds only after mild prodding or shaking | Few recognizable words | - | - | 2 | ||||||||||
| Does not respond to mild prodding or shaking | - | - | - | 1 (deep sleep) |
Table 1: Oaa/S Scale: Assessment Categories. Sum score: 20-18=alert, 17-15=light sedation, 14-11=heavy sedation, under 10=unable
Table 1: Oaa/S Scale: Assessment Categories. Sum score: 20-18=alert, 17-15=light sedation, 14-11=heavy sedation, under 10=unable to cooperate After assessment of the sedation score, airway manipulation was started. If the patient was uncooperative, a bolus of 10mg of propofol in group P or 10μg of fentanyl in group F was given until the patient became cooperative and the number of such boluses was recorded. A nasotracheal tube (7 to 7.5 size in males, 6.5- 7 size in females, portex) lubricated with lignocaine jelly was inserted through the nostril (tube first method) and the fibrescope guided through it. A modified version of the intubating condition score [1] described by Machata et al was used to evaluate the conditions of intubation which included jaw relaxation, vocal cord movement, coughing and limb movements (Table 2). Jaw relaxation was assessed one minute after the bolus dose. After orientation and localization of the laryngo-epiglottic region through the fibreoptic bronchoscope (FOB), vocal cord movement was assessed. Coughing and limb movements were assessed during the entire procedure
| 1 | 2 | 3 | 4 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Jaw relaxation | Complete | Slight tone | Stiff | Rigid | ||||||||||
| Vocal cords | Open | Moving | Closing | Closed | ||||||||||
| Coughing | Slight | Moderate | Severe | |||||||||||
| Limb movement | None | Slight | Moderate | Severe |
Table 2: Intubating condition score [1].
After assessing the vocal cord movement, 5 ml of lidocaine 2% was sprayed on the supraglottic region through the working channel of the FOB (Spray as you go technique). Additionally, 2 ml of lidocaine 2% was sprayed on the vocal cords while asking the patient to take deep breaths. After successful passage of the tube through the vocal cords and identification of the carina, the FOB was withdrawn. Anaesthesia was induced with propofol given in a dose to abolish eyelash reflex and vecuronium for relaxation. The cuff was inflated and the endotracheal tube connected to the breathing circuit. Heart rate, noninvasive blood pressure and oxygen saturation were noted using the same multipara monitor at different stages [2] of awake FOI as follows: a) Baseline b) Insertion of endotracheal tube at nares c) Fibrescope inserted endotracheally d) Endotracheal tube advancement e) Post induction of anaesthesia The total duration of FOI was noted i.e. the time taken from the start of airway manipulation to the first appearance of EtCO2 signal on the capnograph.
All the intubations were done by the same consultant while the observations were taken by the second person.
On the first postoperative day, a blinded investigator evaluated the patients on their degree of amnesia and degree of global acceptance with the following scales [5].
Degree of Amnesia
1. =Do not remember anything of the procedure 2. = Just remember some few moments of the procedure or do not remember it very clearly
3. =Remember the procedure very clearly
Degree of Global Acceptance
- =Do not have any discomfort
- =The procedure was bothersome but tolerable
- =The procedure was unbearable
Statistical Analysis
Measured parameters (age, weight and sex) were compared by the Chi square test with significance of ‘p’<0.05.The nonmeasurable parameters were analysed by Mann-Whitney U test and the Wilcoxon signed ranked test
Observations and Results
The types of surgeries performed in the two groups were similar. The age, weight and sex distribution of the two groups was statistically similar (Table 3).
| Sex ratio | Age in years | Weight in kg | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| G | rou | p | |||||||||
| Female:Male | (Mean+ S.D) | (Mean + S.D) | |||||||||
| F | 17:3 | 35.5 + 12.068 | 54.8 + 13.021 | ||||||||
| P | 16:4 | 30.45 + 8.568 | 51.2 + 8.618 |
Table 3: Age, weght and sex distribution of the two groups.
Sedation Scale
The distribution of patients having different OAA/S scales at different time intervals in the two groups is shown in Figures 1 & 2.
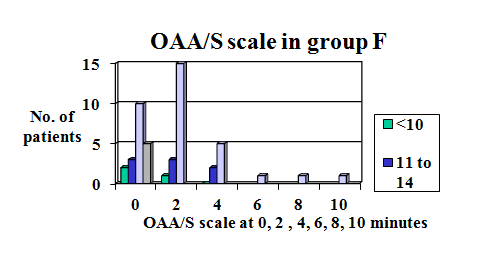
Figure1: Distribution of patients in Group F with OAA/S scales at different times.
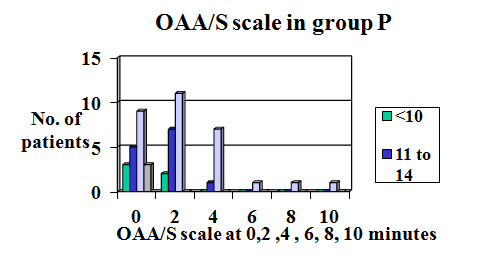
As seen, most patients in both the groups were under light sedation (sum score= 15-17).However, patients in Group P were more sedated (lower sum score) than GroupF. Table 4 shows the mean change in OAA/S scale 60 seconds after the bolus dose (0 minutes) and every 2 minutes thereafter until intubation was completed.
| OAA/S | OAA/S | OAA/S | OAA/S | OAA/S | OAA/S | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group | ||||||||||||||||||||
| 0 min | 2 min | 4 min | 6 min | 8min | 10 min | |||||||||||||||
| F | 15.4 + 3.187 | 15.16 + 2.167 | 15.13 + 1.458 | 16.0 | 16.0 | 16.0 | ||||||||||||||
| P | 14.42 + 2.764 | 13.95 +2.235 | 15.25 +1 .389 | 16.0 | 16.0 |
Table 4: OAA/S scale in the 2 groups.
In both groups, as time progressed, patients were intubated fibreoptically and the number of patients being assessed decreased. After 6 minutes only 1 patient remained in each group therefore statistical analysis was done for sedation scale at 0,2 and 4 minutes only. The difference between the two groups was significant only at 2 minutes (p value=0.028) i.e., patients were more sedated in group P at 2 minutes but not at 0 minutes (p value=0.14) and 4 minutes (p value=0.903). On comparison of OAA/S at different times within the groups, the change at 2 and 4 minutes to 0 minutes was not significant.
Intubating Conditions
A modified version of the intubating condition score [1] which included jaw relaxation, vocal cord movement, coughing and limb movements was used to assess intubating conditions. This is shown in the two groups in Figure 3.
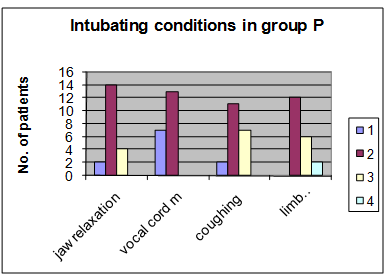
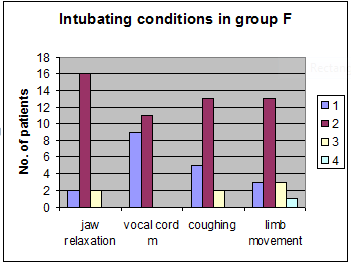
The degree of jaw relation in the two groups was assessed 60 seconds after giving the bolus dose. Slight jaw tone (grade 1) was present in majority of the patients in the two groups while rigidity (grade 4) was not seen in any patient. There was no significant (p value= 0.67) difference between the two groups. In few of the patients (1 in group F and 4 in group P, there was collapse of soft tissues of the pharynx that hampered visualization with the FOB. These patients had either complete jaw relaxation or slight jaw tone (grades 1 and 2).In these patients, a jaw thrust maneuver was performed to generate the requisite space for successfully performing FOI [13].
The vocal cord movement was assessed fibreoptically after the first localization and orientation of laryngoepiglottic region.In both groups , the vocal cords were either open(grade 1) or open but moving(grade 2) and no patient had closing(grade 3) or closed (grade 4) vocal cords. There was no significant difference (Chi square test, p value=0.519) between the two groups. Coughing was assessed in response to the FOI. No patient had severe coughing (grade 4) and the majority had slight coughing (grade 2) during the procedure. There was no significant difference between the groups (Chi square test, p value=0.121). Most patients in group F had none(grade 1) to slight(grade 2) limb movements and most in group P had slight to moderate(grade 3) limb movements. The difference was not statistically significant (Chi square test, P value=0.224). The mean integrated intubating condition score (sum of all the condition parameters) was higher in group P as compared to group F but the difference was not significant.
Haemodynamic Changes
Haemodynamic parameters were noted at different stages of the procedure as mentioned previously and are shown in Figures 4 & 5.
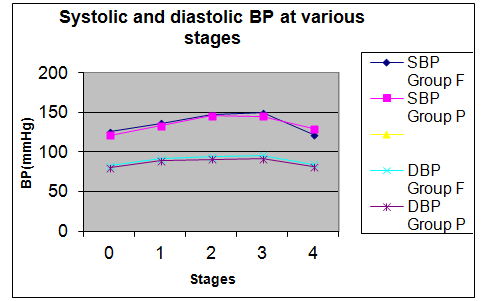
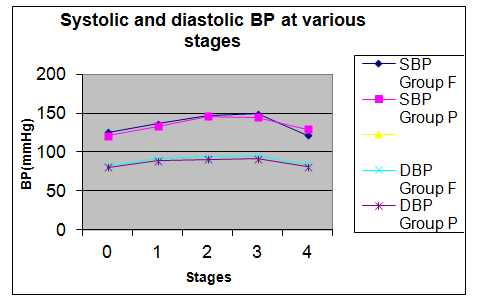
The baseline mean heart rate , systolic and diastolic blood pressures were comparable in the two groups(T test).There was a rise in heart rate from stage 1(insertion of tube at the nares )and was maximum at stage 3 i.e. during advancement of the tube into the trachea..On comparison of the change in heart rate from the baseline it was found that the change was more in group F at all the stages but was significantly more( P value=.007) in group F as compared to group P at stage 2(fibrescope inserted endotracheally). The baseline mean systolic and diastolic blood pressures were comparable in the two groups (T test).A rise in both systolic and diastolic blood pressures was seen in both the groups at the start of the procedure and was maximum at stage 3 .There was no significant difference in the changes in systolic and diastolic blood pressure on comparison of the two groups at any stage
Oxygen Saturation
The change in mean oxygen saturation in the two groups during the different stages of the FOI are shown in Figure 6.
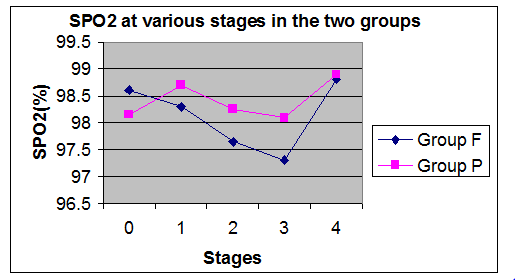
The base line oxygen saturation as well as the saturation at different stages was comparable in the two groups (T test). In group F, two patients had episodes of apnoea after receiving the bolus doses of fentanyl and midazolam. One of these patients had an associated fall in saturation (94% at stage 2 and 85% at stage 3), however the procedure was continued successfully and the saturation rose to 99% following induction. Two patients in the same group went into bradypnoea (respiratory rate < 8 breaths/minute) without associated significant fall in saturation. One patient in group P had a fall in oxygen saturation to 94% at stage 2 and 90% at stage 3.
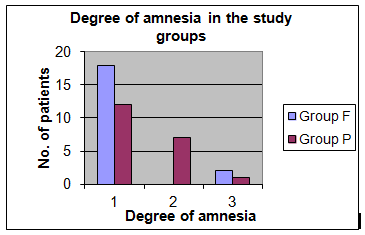
Degree of Amnesia
The degree of amnesia in the two groups of patients is shown in figure 7. 7 As can be seen, a higher number of patients in group F had total amnesia and this difference between the groups was highly significant (P value=0.014) (Figure 7).
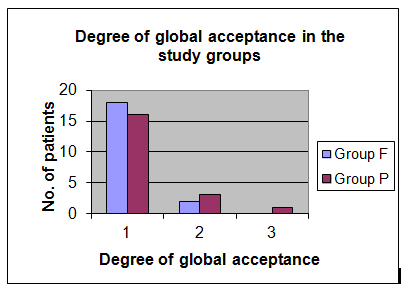
Degree of Global Acceptance
The degree of global acceptance is shown in Figure 8. A higher number of patients in group F had no discomfort as compared to group P, however this difference was not significant (p value=0.517).
Requirement of Additional Boluses
In group F, additional boluses were required in 4 patients i.e. 1 bolus in 3 patients and 3 boluses in 1 patient. In group P more patients required boluses i.e.10 patients (4 patients-2boluses, 2 patients –3 boluses, 1 patient-4 boluses). The difference was significant (p value=0.0032) The total average duration of time taken to achieve intubation was 232 seconds and255 seconds in goups F and P respectively and was comparable in the two groups.
Discussion
FOI is a very useful technique in patients with predicted difficult airway and is the technique of choice in patients with airway pathology such as tumours, trauma, limited mouth opening and decreased atlanto-occipital extension [13]. In such patients it is essential that the patient should be under conscious sedation and breathing spontaneously [1]. Blunting of airway reflexes is achieved by local anaesthesia and sedative agents. Narcotic analgesics are the key to facilitating conscious intubation. These are usually combined with benzodiazepines such as diazepam and midazolam [2, 14, 15].This combination has been used widely [2, 3, 4]. Propofol has been used as a sedating agent for fibroptic bronchoscopy [4, 5, 6] as it produces predictable and quick sedation, haemodynamic stability and deep amnesia. There are reports of its use during awake oral fibreoptic intubation and comparison of target controlled infusions of propofol with remifentanil [10, 11, 12]. Though remifentanil has ideal properties for sedation during FOI, it has been found to have very little amnesic effect [11]. Propofol has been compared to midazolam and found to be superior to it [16] but has been found comparable with the fentanyl- midazolam combination for conscious sedation during awake nasotracheal FOI [15]. We used the dose of propofol used by Gonzalez, et al. [4] and Randell, et al. [5] for sedation during bronchoscopy .The dose of midazolam was that used by Machata, et al. [1] in combination with remifentanil for nasal FOI and fentanyl was used in the dose used by Randell, et al. [5] In our study, we found that in the doses used by us, propofol produced comparable sedation and intubating conditions as a combination of midazolam and fentanyl. It produced significantly more sedation at stage 2 which is a desirable characteristic as it did not lead to bradypnoea and desaturation however, as the procedure progressed more boluses of propofol were needed to continue with the procedure. It also lead to less increase in heart rate at stage 2 which may be a desirable characteristic in some patients. Hoever airway collapse was seen more frequently with the dose used by us in comparison to fentanyl-midazolam combination .Increasing the dose further may cause collapse of airway more easily thereby compromising the airway in patients with difficult airways. The degree of amnesia for the procedure was less with propofol however, the degree of acceptance was comparable to group F. To conclude, propofol is a suitable agent for conscious sedation for FOI under topical anaesthesia without combination with any other agent. The exact infusion dose of propofol required for this purpose needs further study.
References
-
Machata AM, Gonano C, Holzer A, Andel D, Spiss CK, et al. (2003) awake nastracheal fibreoptic intubation: Patient comfort, intubating conditions, and haemodynamic stability during conscious sedation with remifentanil. Anaesth Analg 97(3): 904-908.
-
Puchner W, Egger P, Puhringer F, Lockinger A, Obwegeser J, et al. (2002) Evaluation of remifentanil as a single drug for awake fibreoptic intubation. Acta Anaesthesiol Scand 46(4): 350-354.
-
Reed AP (1995) Preparation for intubation of the awake patient. Mt Sinai J Med 62(1): 10-20.
-
Gonzalez R, Ramirez ID, Hernandez AM, Cherit GD (2003) Should patients undergoing a bronchoscopy be sedated? Acta Anaesthesiol Scand 47(4): 411-415.
-
Randell T (1992) Sedation for fibrescopy: Comparison between propofol infusion and intravenous boluses of fentanyl and diazepam. Acta Anaesthesiol Scand 36(3): 221-225.
-
Clarkson K, Power C K, Connell F Pathmakanthan S, Burke CMA (1993) comparative evaluation of propofol and midazolam as sedative agents in fibreoptic bronchoscopy. Chest 104(4): 1029-1031.
-
Kazama T, Ikeda K, Morita K, Katoh T, Kikura M(1998) Propofol concentration required for endotracheal intubation with a laryngoscope or fibrescope and its interaction with fentanyl. Anaesth Analg 86(4): 872-879.
-
Andel H, Klune G, Andel D, Felfernig M, Donner A, et al. (2000) Propofol without muscle relaxants for conventional or fibroptic nastracheal intubation: A dose finding study. Anaesth Analg 91(2): 458-461.
-
Gueret G, Billard V, Bourgain J (2007) Fibre-optic intubation teaching in sedated patients with anticipated difficult intubation. Eur J Anaesthesiol 24 (3): 239-244.
-
Lallo A, Billard V, Bourgain JL (2009) A comparison of propofol and remifentanil target-controlled infusions to facilitate fiberoptic nasotracheal intubation. Anesth Analg 108(3): 852-857.
-
Cafiero T, Esposito F, Fraioli G, Gargiulo G, Frangiosa A, et al.(2008) Remifentanil-TCI and propofol-TCI for conscious sedation during fibreoptic intubation in the acromegalic patient. European Journal of Anaesthesiology 25(8): 670-674.
-
Rai M R, Parry T M, Dombrovskis A, Warner OJ (2008) Remifentanil target-controlled infusion _vs_ propofol target-controlled infusion for conscious sedation for awake fibreoptic intubation: a double-blinded randomized controlled trial. British Journal of Anaesthesia 100(1): 125-130.
-
Durga VK, Millns JP, Smith JE (2001) Maneuvres used to clear the airway during fibreoptic intubation. Br J Anaesth 87(211): 207-211.
-
Stackhouse RA (2002) Fibreoptic Airway management. Anaesthesiology Clin Am 20(4): 933- 951.
-
Johnston KD, Rai MR (2013) Conscious sedation for awake fibreoptic intubation: a review of the literature. Can J Anesth 60(6): 584-599.
-
Sharan R, Mohan B, Kaur H, Bala A (2016) Efficacy and safety of propofol versus midazolam in fiberoptic endotracheal intubation. Anesthesia, Essays and Researches 10(3): 437-445.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index