Effect of Caffeine on Time to Anesthetic Emergence after Laparoscopic Cholecystectomy: Randomized-Controlled Trial
Background: The aim of this study was to examine the effect of caffeine on the time to emerge from sevoflurane anesthesia for laparoscopic cholecystectomy. Methods: Prospective, randomized, double-blind study conducted between July 2021 and October 2021. ASA I and II patients proposed for laparoscopic cholecystectomy were included and randomized into 2 groups at the end of the surgery to receive either 300mg of caffeine citrate infusion (C) or saline infusion (S). The main endpoint was to compare anesthetic recovery times. The secondary endpoints were recovery scales, postoperative pain, time to the first flatus, fatigue, occurrence of cardiovascular adverse events, and plasma caffeine levels one and twenty-four hours after intravenous infusion. Results: Sixty patients were included. Both groups were comparable regarding demographic characteristics and anesthesia parameters. All average times to emergence were shorter in group C with significant differences (p <0.05) for time to spontaneous ventilation (p= 0.002, -2.86 min) and time to extubation (P= 0.004, -3.51 min). In group C the modified Aldrete scale and the Richmond agitation-sedation scale were significantly higher. Fatigue was significantly lower 4 hours postoperatively with caffeine (p = 0.049). There was no difference regarding postoperative pain, headache incidence, nausea and vomiting, time to the first flatus and satisfaction at discharge from hospital. Plasma levels of caffeine were well below the toxicity threshold. Conclusion: Caffeine administration following laparoscopic cholecystectomy reduced the time to emergence and sedation. Cardiovascular adverse events were not reported and plasma levels were well below the toxicity threshold.
Introduction
Recovering from general anesthesia starts at the moment of stopping infusion of anesthetic drugs. It is considered as a critical phase during which occurred many complication due to anesthesia [1]. In addition to that, emergence from anesthesia could be prolonged due to several factors which could affect the turnover in the operating room especially for ambulatory surgery [2]. So reducing tracheal extubation time should have economic and medical impacts. Elderly patients represent a particularly vulnerable population because their emergence from general anesthesia could be prolonged from hours to days in some cases [3]. However, there are actually no available molecule which, by antagonizing hypnotic, actively accelerate anesthetic emergence contrary to other categories of drug routinely used like opioids, benzodiazepine and curare. Recently, it has been demonstrated in several studies that a series of drugs (aminophylline, doxapram and caffeine) which elevate cAMP could accelerate recovery time from anesthesia but they have cardiovascular side effects. Among these drugs, caffeine was considered as the most effective one with fewer side effects. This was confirmed initially by trials on rats [4] than by studies on healthy humans [5] but as far as we know there is no trials published in the literature which evaluated effect of caffeine on recovery time after laparoscopic surgeries. Thus, we conduct this study in order to examine the effect of one single dose of intravenous (IV) caffeine (300 mg) on the time to emerge from Sevoflurane anesthesia for laparoscopic cholecystectomy.
Methods
After approval of the local ethics committee (HTHEC-2017-09), in addition to the collect of the patient written informed consent during the pre-anesthetic consultation, a double blind prospective randomized study was conducted at the anesthesia and intensive care unit with the collaboration of the visceral surgery department between July 2021 and October 2021.
American society of Anesthesiologists (ASA) I and II patients, aged older than 18 years old and scheduled for laparoscopic cholecystectomy were screened for eligibility.
We did not include patient with an allergy to caffeine citrate and analgesics used during postoperative period, those with severe renal or hepatic failure, those who refused to participate in addition to patient with heart rhythm disorder, seizure disorder, hypertension, alcoholic or psychiatric illness. They were excluded also those with difficult intubation criteria or in case of intraoperative complications and conversion into laparotomy.
Randomization of Patients
Patients were Randomized into Two Groups using Drawing Lots
- GC group: those who received 300 mg of caffeine citrate infusion
- GS group: those who received saline infusion Study group allocation, preparation of the infusion and blood samples were assessed by an anesthesiologist who was unaware to the surgery and data collection. That is why our study needed at least two different investigators.
Anesthesia Procedure
No premedication was given and upon arrival to the operating room, peripheral venous catheter was placed and standard monitoring was initiated including electrocardiogram, non-invasive blood pressure (systolic, diastolic and mean arterial pressure) respiratory rate, end- tidal CO2 (EtCO2), sevoflurane levels and pulse oximetry (SpO2).
Hemodynamic parameters which represented by the heart rate (HR), systolic blood pressure (SBP) and mean blood pressure (MBP) in addition to the SpO2 were noted initially before the initiation of the general anesthesia.
We started with a preoxygenation with an inspired oxygen fraction (FiO2) 100% until the expired oxygen fraction (FeO2) exceeded 90%, and then we performed the induction with: fentanyl 2 µg/kg, titrated infusion of propofol (2 mg/kg) and cis-atracurium 0.15 µg/kg. After that, an orotracheal intubation was done with an adapted probe and the maintenance phase was ensured using Sevoflurane (inspired fraction 2%), cis-atracurium 0.03 µg/ kg and fentanyl 0.05µg/kg. Ventilation was adjusted in order to maintain ETCO2 at 35±5 mmHg using 2L/min of oxygen and room air. Subjects were given nausea prophylaxis with 8 mg of IV Dexamethasone.
At the end of the surgery, the study drug was given intravenously over ten minutes than the sevoflurane infusion was stopped corresponding to the start of the recovery period (T0). In addition to that, every patient received 1g IV paracetamol, 20 mg of Nefopam and 100 mg IV Ketoprofen. The following parameters were evaluated: time to return to spontaneous breathing, eye opening on verbal command, responsiveness to commands (hand squeezing) and tracheal extubation. Throughout emergence period, we measured the mean arterial pressure (MAP), heart rate (HR) and SpO2 every 5 minutes during 30 minutes than every 30 minutes during two hours. In the post anesthesia care unit, Richmond agitation-sedation score (RASS score) was measured in addition to the Aldrete score every five minutes during 30 minutes. A visual analogic scale (VAS) was using in order to assess postoperative pain and measured every five minutes during 30 minutes than every one hour during four hours and finally after 12 and 24 hours postoperative. If the VAS value was greater than 40 mm, the patient received 2 mg IV morphine with an objective of VAS < 40 mm. Patients were returned to their hospitalization unit if Aldrete score was greater than 9 and VAS value < 40 mm.
Several parameters were measured during postoperative period: incidence of headaches and their intensity, incidence of nausea and vomiting, feeling of tiredness at 4 hours postoperative and 24 hours with tiredness score, rehabilitation parameters (food intake and bowel movement) and satisfaction of the patient.
Plasma Caffeine Levels
Concerning the patient who received caffeine infusion, blood samples (3 mL, prechilled tube containing heparin) were done at one hour postoperative (after the end of the infusion) and 24 hours. Blood samples were sent directly to the laboratory or stored at -80°C until performing the assays. Plasma caffeine level was measured by high performance liquid chromatography with ultraviolet detection (HPLC-UV) after centrifuging the plasma.
The mobile phase consisted of 17% of acetonitrile and 83% of Dipotassium Phosphate, the acidity of which was adjusted to pH=3.5 and the flow of the eluent was 1mL/ min. For the stationary phase, we used RP 18 Lichrospher® column (150 mm * 5µm). Extraction of caffeine was done using perchloric acid 17.5%. Finally, and after centrifugation, the organic phase was collected (50µL) and injected into the chromatographic system.
Outcome Measures
The primary endpoint in our study was anesthetic recovery time while we measured time to return to spontaneous breathing, eye opening on verbal command and time for extubation. Several secondary endpoints were measured, including plasma caffeine levels at H1 and H24 after infusion of IV caffeine, as well as hemodynamic parameters after infusion of caffeine, RASS score and Aldrete score, postoperative pain (VAS) and consumption of morphine. Additional secondary endpoints related to postoperative rehabilitation were also collected including the incidence of headache, nausea and vomiting, tiredness score, time to the first flatus and satisfaction of patients.
Statistics and Sample Size
Parameters used to calculate simple size were derived from data obtained by Fong R, et al. [12] in healthy male. Based upon those results, we used an overall two-sided significance level of 0.01, 95% power and expected reduction in recovery time of 50% so we estimated that 30 subjects in each group would be sufficient.
SAS®Studio 9.04 was used for statistics. The qualitative variables were described as percentage and compared using the Pearson Chi2 test. The distribution of continuous variables was evaluated using the Kolmogorov-Smirnov test. Student t-test was used for normality distributed continuous variables and the Mann-Whitney test for non-normality distributed variables. We expressed continuous variables as means and standard deviation or median and interquartile depending on the data distribution. General linear modeling (GLM) and least square mean method were used for clearly compare the anesthetic recovery time. A P-value less than 0.05 was considered as significant.
Results
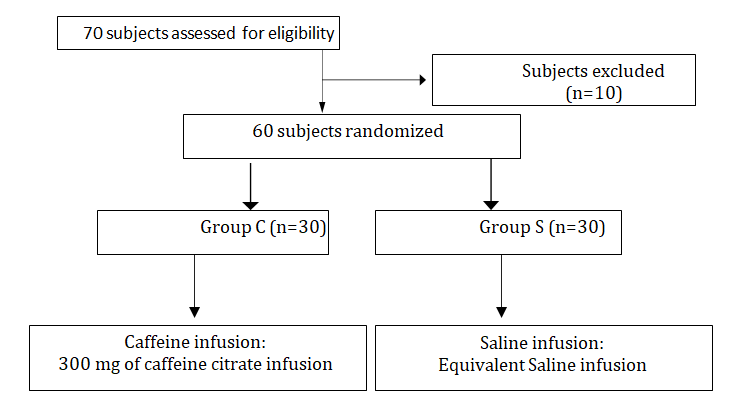
Seventy subjects were assessed for eligibility (Figure 1), ten were excluded and others randomized into two groups (30 patients in each group). Patients characteristics were comparable among the two groups with no significant difference noted (Table 1). Concerning the surgery, we did not notice any conversion into laparotomy or other complication. In addition to that, duration of surgery was comparable among the two groups. The corresponding average dose per kilogram of weight of caffeine was 3.9 ± 0.59 mg and minimum and maximum doses were respectively 2.7 and 5.2 mg per kg.
| Group C (n=30) | Group S (n=30) | P | ||
|---|---|---|---|---|
| Age (years) | 39,3±10,0 | 42,4±12,3 | NS | |
| BMI (kg/m2) | 29,2± 04,2 | 28,5± 03,8 | NS | |
| Sex (M/F) | 27-Mar | 27-Mar | NS | |
| ASA | I | 23 | 26 | NS |
| II | 7 | 4 |
Table 1: Patient characteristics.
Group C: caffeine group; Group S: Saline group; P: p value; NS: non-significant; M: male; F: female; BMI: body mass index; ASA: American Society of Anesthesiology. Table 1: Patient characteristics.
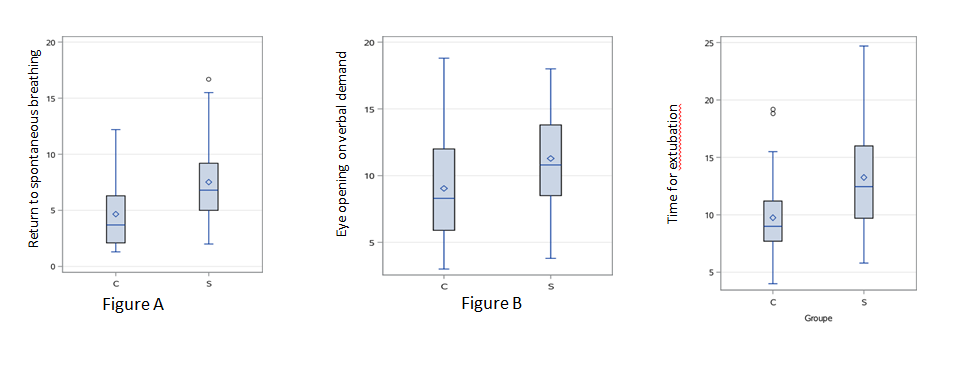
Concerning the primary endpoint which was anesthetic recovery time (Figure 2), the return to spontaneous breathing occurred first in the caffeine group (4,6 ± 3,1 min vs 7,5 ± 3,5 min). Eye opening on verbal command was observed after 9,0 ± 4,1 min in group C and 11,3 ± 4.4 min in group S. Extubation of patients were done after 9,7±3,7 min in group C and 13,3 ±4,9 in group S. That is why, time to emergence was shorter in group C comparing to group S however significant difference was noted only for the return to spontaneous breathing (p=0.002) and time for extubation (p=0.004). In order to analyze the net impact of the caffeine on the anesthetic recovery time, general linear modeling was used and we found that the fact of randomization into two groups was the principal factor affecting the return to spontaneous breathing and time for extubation (Table 2).
| Source of variation | P | |
|---|---|---|
| RSB | TE | |
| Group | 0.0035 | 0.0015 |
| Weight | 0.094 | 0.17 |
| Age | 0.8206 | 0.8044 |
| Duration of general anesthesia | 0.8687 | 0.2439 |
| Total dose of fentanyl | 0.4323 | 0.5812 |
Table 2: principal factor affecting the return to spontaneous breathing and time for extubation.
P: p value; RPB: return to spontaneous breathing; TE: time for extubation. Table 2: principal factor affecting the return to spontaneous breathing and time for extubation.
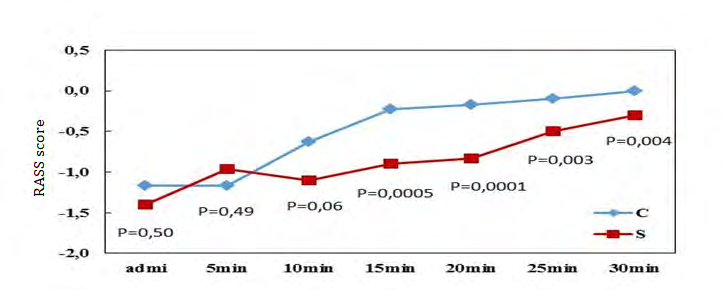
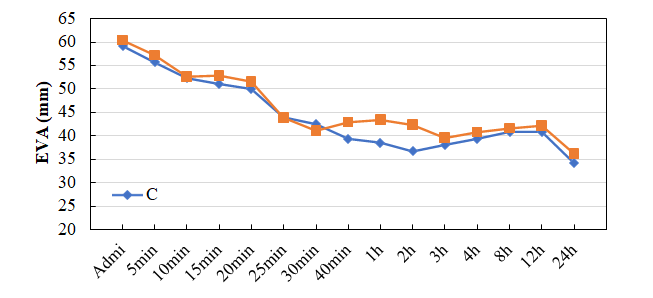
After the extubation, RASS score and Aldrete score were higher in group C with significant difference (Figure 3). Concerning the hemodynamic parameters, heart rates were higher in group S from 15 min after the drug infusion but without a significant difference. Although, PAS and PAD were similar with no significant difference. Fatigue was significantly lower 4 hours after surgery with caffeine (p = 0.049). There was no difference between the two groups regarding postoperative pain (Figure 4), headache incidence, nausea and vomiting, time to the first flatus and satisfaction at discharge from hospital.
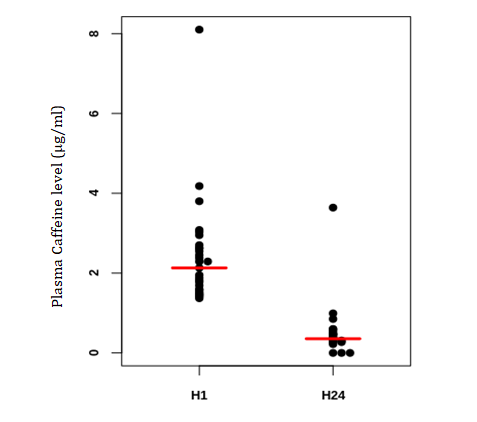
For the plasma caffeine levels, a total of 29/30 of blood samples were collected at H1 from patients of group C and 26/30 at H24. As a result, plasma caffeine level was 2,4 ± 1,3 µg/ml at H1 and 0,5 µg/ml at H24 (Figure 5).
Discussion
In our study, we demonstrate that caffeine administration at the end of a laparoscopic cholecystectomy reduced the time to emergence and sedation in patients recovering from sevoflurane anesthesia without any significant negative effects. Although, we noted that after a single intravenous dose of 300 mg of caffeine citrate, plasma levels dosed one hour and 24 hours after the end of infusion were much lower than the toxicity threshold.
As far as we know, there are currently no available drugs which reverse or accelerate emergence from general anesthesia [6]. Many factors influencing patient recovery from anesthesia are beyond the clinician’s control, like for example some comorbidities, age or genetic factors [7]. Although, several neurochemical circuits are supposed to be involved in the emergence from anesthesia including the cholinergic and adrenergic system [8, 9]. In addition to that, increasing level of intracellular cyclic adenosine monophosphate (cAMP) could decrease sensitivity to hypnotics by stimulating the release of neurotransmitters in neurons [10, 11], however according to Wang Q, et al. [4], of the drugs that were supposed to elevate cAMP, caffeine (which is a psychoactive drug that block adenosis receptors and elevate cytosolic cAMP levels [12]. was considered as most effective with a reduction in the recovery time up to 60%.
Regarding time to emergence from anesthesia, our results were similar to those published by Fong R, et al. [5] which concluded that intravenous caffeine was able to accelerate emergence from isoflurane anesthesia in healthy volunteer males without any apparent adverse effects. In our study, we included patients from both gender and it is well known that gender is involved in pharmacokinetics of drugs.
Concerning the respiratory effect of caffeine, it is well known that this type of drug stimulates the respiratory centers via the antagonization of adenosine A1 and A2a receptors that is why it was used in newborns as an apnea treatment [13]. So according to this effect, we could explain why the return to spontaneous breathing occurred first in caffeine group with a significant difference comparing to the saline group. This was also confirmed by Kim DW, et al. [14] which found that other respiratory stimulant like aminophylline and doxapram (with the same effect of caffeine) reduced the return to spontaneous breathing after general anesthesia. However, in contrast to the results found by Gouda NM, et al. [15] and Fong R, et al. [5], we observed that there was no significant difference concerning eye opening on verbal command between the two groups. This could be explained by the low dose of caffeine that was used (300 mg) comparing to those used in other studies (500 mg), because the fact of increasing the dose of caffeine was associated with a larger reduction of recovering time from anesthesia [4, 12].
The choice of this low dose was explained by the risk of reaching peaks of high plasmatic concentration of caffeine. 300 mg was chosen according to the recommendation of European Food Safety and Authority published in 2015 indicating a maximum daily oral consumption of caffeine for adults not exceeding 400 mg [16] that is why a pharmacologic study was deemed necessary in order to measure plasma caffeine level after single dose of IV caffeine. In our study, we found that plasma levels varied from 1.4 µg/ml to 8.1 µg/ml at H1 and from 0 to 3.6 µg/ml at H24. Although, in the literature, analysis of maximal plasma levels after ingestion of caffeine has shown a certain variation [17] and this variation is essentially due to the interindividual difference of the cytochrome P450 1A2 (CYP A12) activity affected either by genetic factor or environmental factors like smoking or certain drugs (omeprazole, oral contraceptives or fluoroquinolones) [18, 19]. Our result was close to those published in the literature concerning oral ingestion of caffeine (Table 3).
| Authors | Year | Dose | Sex | Plasma level |
|---|---|---|---|---|
| Benowitz (4) | 1995 | 2 mg/kg | M/F | 3 µg/ml |
| Benowitz (4) | 1995 | 4 mg/kg | M/F | 7.5 µg/ml |
| Teekachunhatean(23) | 2013 | 100 mg | M | 2.5 µg/ml |
| Beach (3) | 1984 | 200 mg | M/F | 3.4 µg/ml |
Table 3: Review of studies concerning emergence from anesthesia after oral ingestion of caffeine.
M: male; F: female. Table 3: Review of studies concerning emergence from anesthesia after oral ingestion of caffeine.
Furthermore, we did not note any side effects due to the infusion of caffeine and this could be explained by the low dose of caffeine used, however some authors suggested that there is no correlation between plasma level and side effects probably because of the interindividual difference of pharmacokinetic and pharmacodynamic of caffeine [20, 21]. Concerning the toxicity value, 50 µg/ml is considered as toxicity threshold and 80 µg/ml as lethal threshold [22, 23] however Jones, et al. found by reviewing 51 cases of caffeine poisoning, a median plasma concentration of caffeine around 180 µg/ml. Finally, there are some limits in our study. First, it was a study with small population size. A study with more patients seems necessary especially to assess possible side effects of caffeine. In addition to that, we did not monitor neither the sedation by the Bispectral Index nor the curarization. Concerning the pharmacological part, more blood samples are necessary in order to better explore the pharmacokinetic of caffeine after one infusion [24, 25].
Conclusion
We have shown through this study that caffeine should be an effective molecule in order to reverse Sevoflurane anesthesia and this effect would probably be much better with higher doses. No side effects of caffeine were observed that is why this procedure could be considered as safe, however the right IV posology must be identified and contraindication of caffeine must be respected before using it routinely. Finally, further study with larger simple size in addition to more robust pharmacological methodologies will be necessary in order to establish whether caffeine enhances anesthesia recovery.
Author Contribution
- Hazem Jaoua: This author helped in designing and implementation of the manuscript, analyzing the result, writing the manuscript and approving the final version.
- Mohamed Aziz Daghmouri: This author helped in writing the manuscript and approving the final version.
- Bochra Fouzai: This author helped in designing and implementation of the manuscript, analyzing the result.
- Soumaya Akremi: This author helped in writing the manuscript and approving the final version.
- Hela Kraiem: This author helped in writing the manuscript and approving the final version.
- Samia Arfaoui: This author helped in writing the manuscript and approving the final version.
- Kamel Ben Fadhel: This author helped in writing the manuscript and approving the final version.
- Marc Raucoules-Aime: This author helped in writing the manuscript and approving the final version.
Clinical Trial Number: NCT05079880.
Ethical Approvement: This trial was approved by the local ethics committee (HTHEC-2017-09).
Prior Presentation: SFAR congress.
Acknowledgments: We would like to express our appreciation to our department team for their valuable assistance and we thank members of visceral surgery department for the in contribution in this study.
Summary Statement: not applicable.
Funding Statement: Support was provided solely from our institutional and departmental sources.
Conflicts of Interest: The authors declare no competing interest.
References
-
Gupta S, Naithani U, Brajesh SK, Pathania VS, Gupta A, et al. (2009) Critical Incident Reporting in Anaesthesia: A Prospective Internal Audit. Indian J Anaesth 53(4): 425- 433.
-
Epstein RH, Dexter F, Brull SJ (2013) Cohort study of cases with prolonged tracheal extubation times to examine the relationship with duration of workday. Can J Anaesth 60(11): 1070-1076.
-
Chen G, Zhou Y, Shi Q, Zhou H (2015) Comparison of early recovery and cognitive function after desflurane and sevoflurane anaesthesia in elderly patients: A meta- analysis of randomized controlled trials. J Int Med Res 43(5): 619-628.
-
Wang Q, Fong R, Mason P, Fox AP, Xie Z, et al. (2014) Caffeine accelerates recovery from general anesthesia. J Neurophysiol 111(6): 1331-1340.
-
Fong R, Wang L, Zacny JP, Khokhar S, Apfelbaum JL, et al. (2018) Caffeine Accelerates Emergence from Isoflurane Anesthesia in Humans: A Randomized, Double-blind, Crossover Study. Anesthesiology 129(5): 912-920.
-
Brown EN, Lydic R, Schiff ND (2010) General anesthesia, sleep, and coma. N Engl J Med 363(27): 2638-2650.
-
Solt K, Cotten JF, Cimenser A, Wong KFK, Chemali JJ, et al. (2011) Methylphenidate actively induces emergence from general anesthesia. Anesthesiology 115(4): 791- 803.
-
Tarnal V, Vlisides PE, Mashour GA (2016) The Neurobiology of Anesthetic Emergence. J Neurosurg Anesthesiol 28(3): 250-255.
-
Kushikata T, Hirota K (2014) Mechanisms of Anesthetic Emergence: Evidence for Active Reanimation. Curr Anesthesiol Rep 4(1): 49-56.
-
Kasai H, Takahashi N, Tokumaru H (2012) Distinct initial SNARE configurations underlying the diversity of exocytosis. Physiol Rev 92(4): 1915-1964.
-
Saifee O, Metz LB, Nonet ML, Crowder CM (2011) A gain-of-function mutation in adenylate cyclase confers isoflurane resistance in Caenorhabditis elegans. Anesthesiology 115(6): 1162-1171.
-
Fong R, Khokhar S, Chowdhury AN, Xie KG, Wong JH-Y, et al. (2017) Caffeine accelerates recovery from general anesthesia via multiple pathways. J Neurophysiol 118(3): 1591-1597.
-
Mayer CA, Haxhiu MA, Martin RJ, Wilson CG (2006) Adenosine A2A receptors mediate GABAergic inhibition of respiration in immature rats. J Appl Physiol 100(1): 91-97.
-
Kim DW, Joo JD, In JH, Jeon YS, Jung HS, et al. (2013) Comparison of the recovery and respiratory effects of aminophylline and doxapram following total intravenous anesthesia with propofol and remifentanil. J Clin Anesth 25(3): 173-176.
-
Gouda NM (2010) Intravenous Caffeine for Adult Patients with Obstructive Sleep Apnea Undergoing Uvulopalatopharyngoplasty: Effects on Postoperative Respiratory Complications and Recovery Profile. The medical journal of cairo university 78(2).
-
European Food Safety Authority (2015) Caffeine: EFSA estimates safe intakes.
-
Willson C (2018) The clinical toxicology of caffeine: A review and case study. Toxicol Rep 5: 1140-1152.
-
Arnaud MJ (2011) Pharmacokinetics and metabolism of natural methylxanthines in animal and man. Handb Exp Pharmacol (200): 33-91.
-
Dorne JL, Walton K, Renwick AG (2001) Uncertainty factors for chemical risk assessment human variability in the pharmacokinetics of CYP1A2 probe substrates. Food Chem Toxicol 39(7): 681-696.
-
Beach CA, Bianchine JR, Gerber N (1984) The Excretion of Caffeine in the Semen of Men: Pharmacokinetics and Comparison of the Concentrations in Blood and Semen. The Journal of Clinical Pharmacology 24(2-3): 120-126.
-
Bonsignore A, Sblano S, Pozzi F, Ventura F, Dell’Erba A, et al. (2014) A case of suicide by ingestion of caffeine. Forensic Sci Med Pathol 10(3): 448-451.
-
Jabbar SB, Hanly MG (2013) Fatal caffeine overdose: a case report and review of literature. Am J Forensic Med Pathol 34(4): 321-324.
-
Banerjee P, Ali Z, Levine B, Fowler DR (2014) Fatal caffeine intoxication: a series of eight cases from 1999 to 2009. J Forensic Sci 59(3): 865-868.
-
Benowitz NL, Jacob P, Mayan H, Denaro C (1995) Sympathomimetic effects of paraxanthine and caffeine in humans. Clinical Pharmacology & Therapeutics 58(6): 684-691.
-
Teekachunhatean S, Tosri N, Rojanasthien N, Srichairatanakool S, Sangdee C, et al. (2013) Pharmacokinetics of Caffeine following a Single Administration of Coffee Enema versus Oral Coffee Consumption in Healthy Male Subjects. ISRN Pharmacol 2013: 147238.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index