Anesthetic Concerns in a Child Presenting with Large Cervical Chordoma A Case Report
Chordomas are rare, low-grade, and slow-growing malignant tumors with an incidence rate of 0.08 in 1,00,000 people. Spinal chordomas can cause back pain, pathological fractures, and myelopathy or radiculopathy due to spinal cord and nerve root compression. Treating these tumors can be challenging owing to their proximity to vital structures and high recurrence rates. We report the anesthesia management of a 10-year-old boy with cervical chordoma posted for laminectomy, and excision was a challenge for airway management.
Introduction
Chordoma is a rare, low-grade malignant tumor arising from the remnants of the embryonic notochord, with a prevalence of 0.08 in 100,000 people [1, 2]. High cervical chordomas are rare but may be associated with difficult airways. Other problems are their proximity to various vital structures and a high recurrence rate. Therefore, it is imperative to formulate an anesthetic plan that considers intubation and extubation with minimal disturbance to the cervical region. To be prepared for the effects of the tumor depending on its infiltration, delayed recovery of respiratory function, and prolonged ventilation in the postoperative period. Anesthesia management, especially the airway component for such cases, for the pediatric age group is lacking in the literature, except for a few case reports on adult clival chordoma [3, 4, 5]. Here, we report the anesthesia management of a 10-year-old boy with cervical chordoma posted for laminectomy, and excision was a challenge for airway management. This manuscript adheres to the applicable EQUATOR guidelines. Written and informed consent was obtained from the patient’s father to publish this case report.
A 10-year-old boy (mass: 30 kg) presented with complaints of swelling on the posterior area of the neck for 8 years, which was gradually increasing in size was considered. There was no associated neurological deficit.
He had adequate mouth opening, normal temporomandibular joint movement, and Mallampati grade III. A neck examination revealed restricted neck movements in extension, not in flexion. There was a non-tender, lobulated mass of approximately 5 × 4 × 4 cm, with no redness or pain in the cervical region (Figure 1). The anterior surface of the neck was hard, and generalized swelling (left > right) was present.

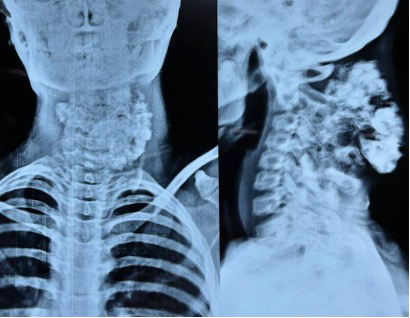
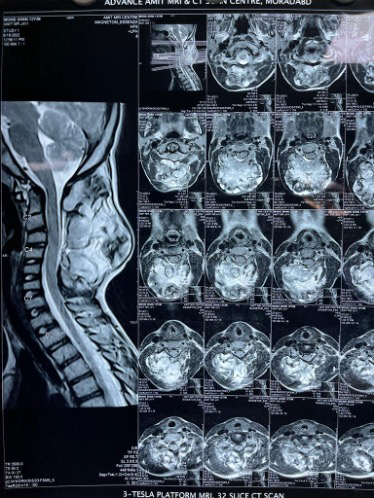
The standard lab test values were within the normal range. X-rays of the head and neck (lateral and anteroposterior) showed a lobulated mass and no obvious airway compromise (Figure 2). Whole-spine magnetic resonance imaging revealed a 10.7 × 5.2 × 7.3 cm lesion involving posterior elements of the C1–C6 vertebra with no intradural extension or involvement of paraspinal muscles (Figure 3). Fine needle aspiration cytology suggested that a cervical chordoma was present. The patient was scheduled for laminectomy and excision of the lesion.
Due to the anticipated difficult intubation, the difficult airway cart was kept ready. Unfortunately, an institutional fiberoptic bronchoscope (FOB) was not in working condition. General anesthesia was instituted using standard induction agents and muscle relaxants. The first intubation attempt was performed using Macintosh blade 3 with manual in-line stabilization, which failed due to immobility of epiglottis (Cormack–Lehane grade IIIB). In the second attempt, we used a video laryngoscope with manual in-line stabilization, which also failed. We decided to proceed with our backup plan for retrograde intubation. Intermittent bag and mask ventilation was continued. Following strict asepsis for using a 16-gage cannula, the trachea was punctured at the levels of the first and second tracheal rings, and the tracheal lumen was identified by free aspiration of air through a saline-filled syringe. A sterile flexible straight-tipped urology guidewire (Devon, Netherlands; length 150 cm, size 0.032’’) was then gently introduced and navigated through the needle bore to be retrieved from the mouth, and the distal end was clamped with artery forceps. Subsequently, we railroaded a pediatric bougie through the guidewire but failed to insert it through the glottic opening. Therefore, we removed the bougie and railroaded the guidewire through the nostril using a suction catheter. Once the guidewire came out through the nostril, we tried to insert a pediatric bougie and railroaded a 6-mm polyvinylchloride endotracheal tube through the bougie using adequate water-based lubricant jelly to prevent any injury. Once the tube was successfully passed through the glottic opening, the bougie was first removed, followed by the guidewire. The endotracheal tube was confirmed using auscultation and capnography.
An invasive arterial line (22-gauge cannula in the left radial artery) and central venous catheter were inserted. Intraoperatively, the patient lost 2.2 L of blood which was replaced with fluids, blood, and blood products. Vasopressor in the form of Nor-adrenaline infusion to maintain mean arterial pressure ≥ 70 mm Hg was started. Considering hemodynamic instability, the patient was shifted to the intensive care unit for elective ventilation. Neurological examination revealed that the patient was quadriplegic on postoperative day 1. Tracheostomy was conducted on postoperative day 2 regarding failed weaning.
Discussion
Chordoma is a relatively rare, low-grade malignant neoplasm. Since a large dural space exists at the C1– C2 location, the tumor usually enlarges before patients experience clinical manifestation, as seen in this study’s patient. The compression of neural tissues and invasion of the brainstem or spinal canal may result in serious neurologic complications. The tumor often encapsulates and/or displaces the vertebral artery and nerve roots [4]. However, neurological deficits or encapsulation of artery/ nerve roots was absent in our patient.
Difficult airway assessment often relies on physical examination indicators, such as inter-incisor gap, thyromental distance, neck circumference, and Mallampati test. However, their accuracy is questionable. Preoperative skeletal X-ray and soft-tissue magnetic resonance imaging measurements are more predictive of difficult airways. We should have relied on these radiological indices or ultrasound assessments to gain insights into the patient’s airways. Chordoma destroys the cervical vertebral body, and cervical stability is impaired near bony elements. Excessive neck extension needs to be avoided to prevent severe spinal cord compression. Awake fiberoptic intubation is the best option to secure the airway in this patient, but the nonavailability of a fiberscope precluded its use. Fiber-optic intubation in pediatric patients is challenging. As fiber-optic intubation depends on the user experience, we have little experience in pediatric patients. Since our senior anesthesiologist was well-versed with the retrograde intubation method, therefore we proceeded with this technique. Fixed epiglottis can be explained by the tumor infiltration of laryngeal muscles, which makes it immobile. The presence of mild and hard generalized swelling in the anterior neck also supports this explanation. Retrograde tracheal intubation, first described in 1960, is an old method [6], which can be useful when all the other airway management techniques have been exhausted? The absence of vessels at the puncture site and fewer chances of subglottic edema or stenosis makes it a good choice of airway maneuver [1]. Due to the nonavailability of the retrograde intubation set, we used a flexible straight- tipped urology guidewire (Devon Guidewire™) because of its hydrophilic coating, which provides good lubricity and kink resistance. Its advantages include fewer chances of airway injury and the extra length of the guidewire safeguards against catheter misplacement or coming out. This approach was described in one case report where the guidewire was removed through the nose, in which the authors managed to easily railroad the endotracheal tube [7]. Anticipating difficult maneuvering of the endotracheal tube through a thin guidewire, we used a pediatric bougie first and then railroaded the definitive airway. Kang RS, et al. [8] reported retrograde fiberoptic transnasal intubation without using a guidewire for a tracheostomy revision procedure [8]. Anesthesiologists can avoid using this technique owing to complications related to retrograde intubation: the inability to locate the cricothyroid membrane, the inability to pass the endotracheal tube through the vocal cords, prolonged procedure time, and hesitancy to use it due to perceived invasiveness. Nevertheless, our purpose of securing the airway was successful in a “cannot intubate” scenario using this rare and underrated method.
Managing the resection of a cervical chordoma involves several anesthetic considerations. Due to the tumor’s proximity to various vital structures, the utmost vigilance must be ensured in the perioperative period. Adequate blood and blood products should be ready in case of massive hemorrhage, and it is ideal to have an arterial line to monitor beat-to-beat arterial blood pressure. Notably, it would have been of great importance if preoperative angiography had been performed to detect the predominant vertebral artery. This warns us regarding arterial involvement and its predominance, like surgery for atlantoaxial instability. Zhang J, et al. [9] explored a literature review and found 12 reported cases of intradural spinal Chordoma [9, 10]. Surgeons can sacrifice C1–4 nerve roots, although postoperative hemidiaphragm may occur [10]. Neuromonitoring using motor evoked potential or somatosensory potential should also be a part of intraoperative management to warn surgeons regarding any nerve injury, even if an apparent intradural extension is absent. Quadriplegia in our patient can be explained by the damage to the spinal cord while tumor dissection. We took measures such as manual in-line stabilization and avoidance of jaw thrust to avoid excessive cervical movement during the airway management. It’s unlikely that it might have contributed to the neurological injury.
We presume that the tumor infiltrated anteriorly, which was not apparent in the radiological examination, thus creating difficulties in securing the airway. The wise decision of using retrograde intubation and timely intervention averted potential morbidity in this patient.
In conclusion, this case report suggests that the residents can learn retrograde intubation method as it is a useful technique in the airway armamentarium. Also, we emphasize the need for careful preoperative workup of expected difficult airway in pediatric patients with spinal chordomas to prevent postoperative morbidity [11, 12, 13, 14].
Acknowledgments: The authors are grateful to the patient’s father for providing informed written consent and to Dr. Gaurav Jain (Associate Professor, All Indian Institute of Medical Sciences, Rishikesh) for teaching us to perform retrograde intubation.
Author’s Contribution
- Nirupa Ramakumar: This author helped in design of the work, substantial contributions to the conceptions, the acquisition of data, drafting the work and revising it critically for important intellectual content. All the authors approved the final version to be published and are accountable for all aspects of the work in ensuring that questions related to accuracy and integrity of any part of the work are appropriately investigated and resolved.
- Shivam Shekhar: This author helped in drafting of work, analysis, interpretation of data for the work and revising it critically for intellectual content.
- Pooja Chandran: This author has substantial contribution to the conceptions and drafting of work and revising it critically for intellectual content.
Conflicts of Interest and Sources of Funding: The authors have no conflicts of interest to declare.
Financial Support: None.
Details of Previous Presentation: No work related to this article is published or presented.
References
-
McMaster ML, Goldstein AM, Bromley CM, Ishibe N, Parry DM, et al. (2001) Chordoma: incidence and survival patterns in the United States, 1973–1995. Cancer Causes Control 12(1): 1-11.
-
Muro K, Das S, Raizer JJ (2007) Chordomas of the craniospinal axis: multimodality surgical, radiation and medical management strategies. Expert Rev Neurother 7(10): 1295-1312.
-
Bhatnagar V, Karmarkar KA, Deepak D (2017) Anesthetic management of excision of recurrent C2 chordoma with extension into posterior pharyngeal wall. Journal of marine medical society 19(2): 128-130.
-
Jiang L, Liu ZJ, Liu XG, Qing JM, Feng W, et al. (2009) Upper cervical spine chordoma of C2-C3. Eur Spine J 18(3): 293-298.
-
Soltanpoor P, Behnaz F, Faresani AH, Seddighi A, Karimian M, et al. (2019) Anesthetic Considerations in a Case with Massive Recurrent Clivus Chordoma. International Clinical Neuroscience Journal 6(2): 76-78.
-
Butler FS, Cirillo AA (1960) Retrograde tracheal intubation. Anesth Analg 39: 333-338.
-
Tiwari T, Sharma B, Rajput SK (2022) A case report of retrograde intubation as rescue procedure in unanticipated difficult airway: an old technique still relevant in low resource settings. Med Gas Res 12(4): 158-160.
-
Kang RS, Hutnik R, Kant I, Zlatopolsky A, Brar C, et al. (2022) Retrograde Intubation Over a Flexible Fiber- Optic Bronchoscope. Anesth Prog 69(1): 42-45.
-
Zhang J, Chuan PG, Liu XJ, Xu WJ (2018) Intradural cervical chordoma with diffuse spinal leptomeningeal spread: case report and review of the literature. Eur Spine J 27(3): 440-445.
-
Ruan H, Mehra RN, Park D, Chou D (2019) Intradural Invasion of Cervical Chordoma in a 34 Year Old Patient. Neurology India 67(6): 1545-1548.
-
Han YZ, Tian Y, Zhang H, Zhao YQ, Xu M, et al. (2018) Radiologic indicators for prediction of difficult laryngoscopy in patients with cervical spondylosis. Acta Anaesthesiol Scand 62(4): 474-482.
-
Gill M, Madden MJ, Green SM (2005) Retrograde endotracheal intubation: an investigation of indications, complications, and patient outcomes. Am J Emerg Med 23(2): 123-126.
-
Vadepally AK, Sinha R, Kumar AVSSS (2018) Retrograde intubation through nasal route in patients with limited mouth opening undergoing oral and maxillofacial surgery. J Oral Biol Craniofac Res 8(1): 30-34.
-
Raval C, Patel H, Patel P, Kharod U (2010) Retrograde intubation in a case of ankylosing spondylitis posted for correction of deformity of spine. Saudi J Anaesth 4(1): 38-41.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index