The Pattern and Outcome of Obstetric Patients Getting Admitted in Surgical Critical Care Unit of Rural Tertiary Care Unit
Background: Obstetric patients requiring critical care are a significant and growing concern worldwide, particularly in lowand middle-income countries. While obstetric patients are generally young and healthy, they can experience life-threatening complications during pregnancy, delivery, or postpartum period. Surgical critical care units (SCCUs) are often the first-line of care for critically ill obstetric patients, providing specialized care for complex surgical cases. Aims and objectives: This study was conducted to know the pattern and outcome of obstetric patients getting admitted in surgical critical care unit of our rural tertiary care unit. Methodology: In this retrospective study, and we have collected the data from the records of one year duration, starting from 1st November 2021 to 30th September 2022 and statistically assessed. Results: A total of 54 patients were admitted in the study period and most of the patients were aged between 18-25 years. There was equal number of admissions noted between primi and multi gravida. 91% of the patients got admitted in the ICU post LSCS. 72% of the patients had PIH, 39% of the patients received blood and 44% received blood products during ICU care. Nearly 41% had to get ventilator support during the course of the treatment. Average number of the stay in ICU was 3 days. There were 15% of the patients who couldn’t survive. Conclusion: Despite being a tertiary care rural hospital with limited resources, we were able to effectively manage critical obstetric patients.
Introduction
Obstetric patients requiring critical care are a significant and growing concern worldwide, particularly in low- and middle-income countries [1]. According to the World Health Organization (WHO), an estimated 830 women die every day from preventable causes related to pregnancy and childbirth, and about 99% of these deaths occur in developing countries. In addition, for every woman who dies, there are approximately 20 more that experience severe complications during pregnancy or childbirth, leading to long-term health problems or disability.
Surgical critical care units (SCCUs) are specialized units that provide intensive care for patients with life-threatening conditions requiring surgical intervention. Obstetric patients can require admission to SCCUs for a variety of reasons, such as hemorrhage, sepsis, eclampsia, or other medical or surgical complications related to pregnancy or childbirth [2]. However, there is limited data on the pattern and outcome of obstetric patients admitted to SCCUs in rural tertiary care units, particularly in developing countries.
Rural areas in developing countries face unique challenges in providing obstetric care, including limited resources, poor infrastructure, and a shortage of skilled health workers. In addition, the distance and lack of transportation can delay women from seeking or receiving care during emergencies, which can result in poor outcomes [3]. The WHO has identified improving access to emergency obstetric care in rural areas as a key strategy for reducing maternal mortality and morbidity [4, 5].
Understanding the pattern and outcome of obstetric patients admitted to SCCUs in rural tertiary care units can help improve the management and outcomes of these patients. The data can help identify common causes of admission, factors associated with poor outcomes, and potential areas for improvement in the delivery of obstetric care in rural areas. In addition, the data can inform the development of targeted interventions and policies to improve access to emergency obstetric care and reduce maternal morbidity and mortality.
Therefore, this study aimed to evaluate the pattern and outcome of obstetric patients admitted to the SCCU of a rural tertiary care unit. The study was conducted retrospectively using data collected from medical records of obstetric patients admitted to the SCCU over a period of one year.
Materials and Methods
After obtaining institutional ethical committee approval, this retrospective study was conducted. This is a record base study done at rural tertiary care hospital. The data was collected for the duration of one year, starting from 1st November 2021 to 30th September 2022 and statistically assessed. This study aimed to investigate the clinical characteristics and outcomes of obstetric patients aged 18 and over who required admission to the surgical critical care unit (SCCU) during the perioperative period due to various surgical complications. Patients who were referred from outside hospitals or refused further treatment at the study hospital were excluded from the study. A total of 54 obstetric patients were included in the study, and their demographic and clinical information were recorded, including type of admission, gravida, length of ICU stays, medico-legal case registration, antenatal care registration status, type of disease, need for ventilation, treatment modalities, referral status, discharge against medical advice, overall outcomes, and mortality rates.
Results
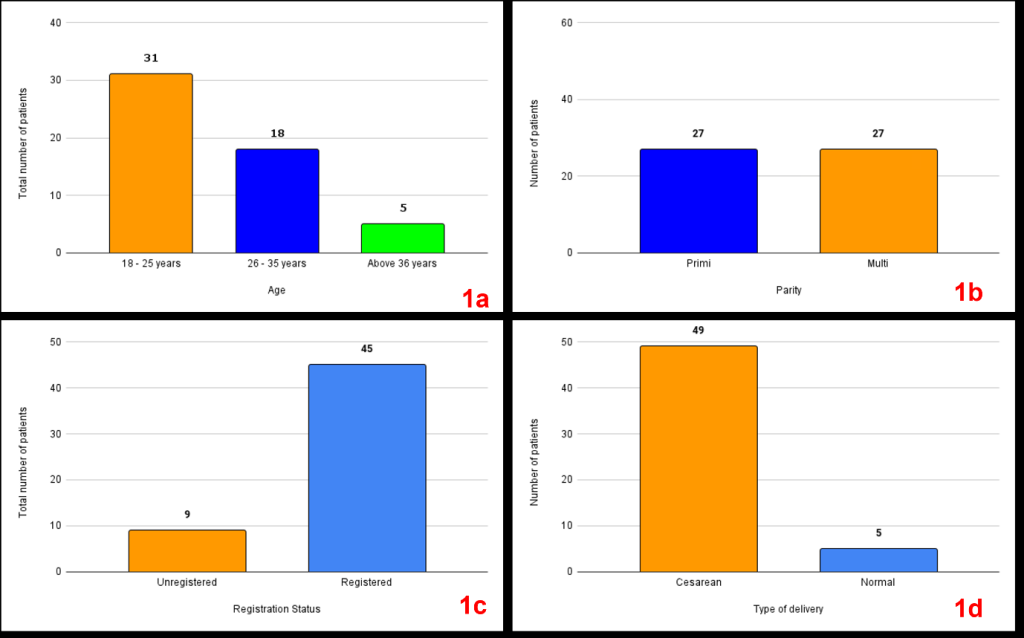
During the aforementioned time period, 55 patients were admitted. Patients of various ages ranging from 18 to 36 were admitted, however the majority of patients were between the ages of 18 and 25 years (Figure 1a). Parity- wise, there were an equal number of patients admitted who were primigravida and multigravida (Figure 1b). Majority of patients were registered during antenatal care as per the government rules (Figure 1c). Post lower segment caesarean sections (LSCS), 91% of patients were admitted to the ICU (Figure 1d).
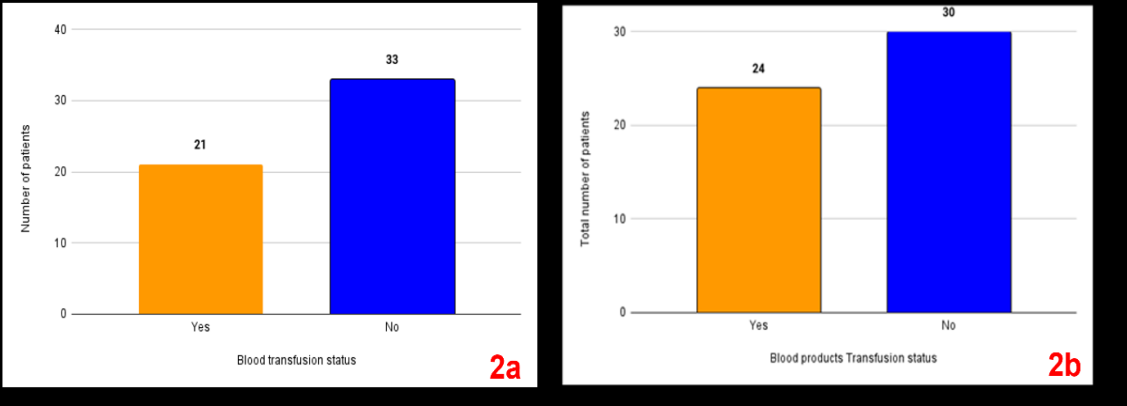
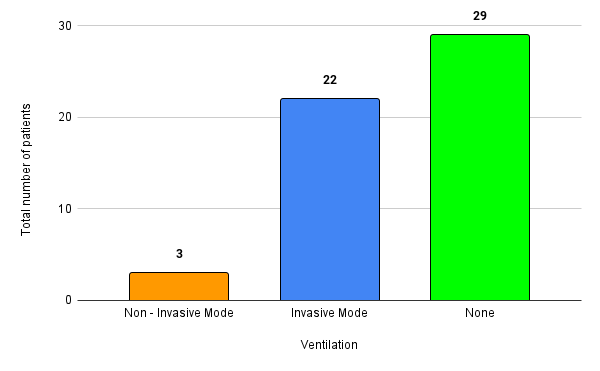
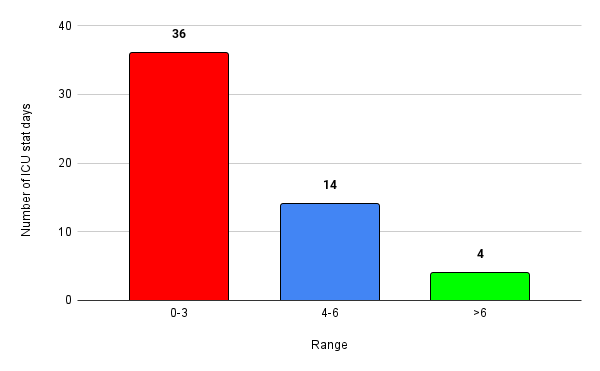
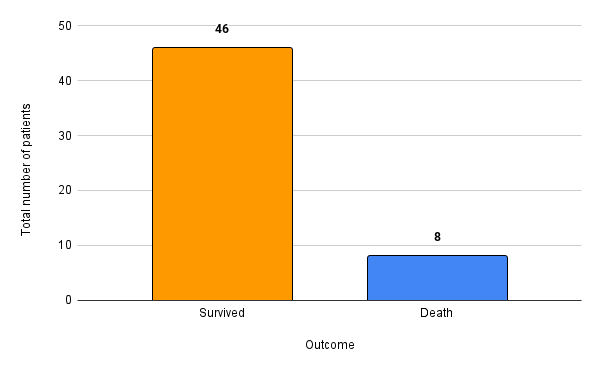
A total of 15 patients had pregnancy induced hypertension out of 54 ICU admissions. 21 patients received blood while 24 patients received blood product (Figure 2). A total of 25 patients required mechanical ventilation out of which 3 were on non-invasive mechanical ventilation and rest 22 were on invasive mechanical ventilation (Figure 3). A total of 36 patients stayed up to 3 days while 4 patients required more than 6 days of stay in the ICU (Figure 4). The survival rate among the 54 patients was 85.2%, with 46 patients making a full recovery and 8 succumbing to their illness (Figure 5).
Discussion
The admission of obstetric patients to surgical critical care units is a complex issue, with a variety of factors contributing to the pattern and outcome of such admissions. In rural tertiary care units, where resources may be limited, understanding these factors is particularly important in order to optimize care for these patients.
One factor that may contribute to the pattern of obstetric admissions to SCCUs is the prevalence of high-risk pregnancies in rural areas. Women in rural areas may be more likely to have limited access to prenatal care, leading to increased rates of maternal and foetal complications. Additionally, rural women may have higher rates of comorbidities such as obesity, hypertension, and diabetes, which can increase the risk of obstetric complications. These factors may lead to a higher rate of obstetric admissions to SCCUs in rural areas. The outcome of obstetric patients admitted to SCCUs in rural areas may also be influenced by a variety of factors. One important consideration is the level of experience and training of the SCCU staff in managing obstetric patients. Obstetric patients have unique physiological and medical needs, and SCCU staff may not be familiar with the specialized care required for these patients. In addition, SCCUs may not have the necessary equipment and supplies to manage obstetric emergencies, such as hemorrhage or eclampsia.
Another factor that may impact the outcome of obstetric patients admitted to SCCUs is the availability of obstetric specialists and consultation services. In rural areas, there may be a shortage of obstetricians and other specialists, making it difficult to provide timely and appropriate care to obstetric patients. This may result in delayed diagnosis and treatment, which can have serious consequences for both the mother and foetus. In our study the maximum number of patients was aged between 18 to 25 years. The possible cause may be early marriage trend in rural area [6]. Parity- wise, there were an equal number of patients admitted who were primigravida and multigravida. It is not uncommon to see multiple pregnancies among rural women [7]. However, in our study we found equal number of primigravida and multigravida patients admitted in surgical critical care unit.
Although it is a rural area, the registration for Antenatal Care (ANC) was surprisingly good. ANC is a vital healthcare service for pregnant women, as it helps to identify and manage potential complications. In this area, the ANC registration rate was about 83.3%, indicating a relatively high level of awareness and utilization of the service. This is a positive development that can contribute to better maternal and child health outcomes in the region [8]. Overall, the good registration rate for ANC in this rural area is a promising sign for the health and wellbeing of both mothers and babies.
In a rural tertiary care setting, we observed a high rate of patients undergoing lower segment caesarean section (LSCS). This high rate of LSCS needs to be examined to ensure that the appropriate indications were used, as overuse of LSCS can increase maternal and neonatal morbidity and mortality, as well as healthcare costs. While LSCS can be a safe and effective intervention for certain medical conditions, such as foetal distress, malpresentation, and previous caesarean section, it is important to consider the potential risks and benefits on a case-by-case basis, taking into account individual patient and clinical factors. These risks can include bleeding, infection, blood clots, longer recovery time, and potential complications in future pregnancies. Due to this it is important to reduce the LSCS rate as low as possible and can be done with regular auditing [9, 10].
Although patients admitted to surgical critical care units require intensive monitoring and management due to the severity of their conditions, it appears that surgical complications such as bleeding may be less common in this population. Our observations suggest that not all patients required blood or blood products during their stay, which may be indicative of a lower incidence of bleeding complications. However, it is important to note that these admissions may not necessarily be related to bleeding diathesis, but may be due to medical problems associated with pregnancy or other conditions. Nevertheless, our observations provide valuable insights into the management and care of surgical critical care patients, and highlight the importance of careful monitoring and management of potential surgical complications, regardless of the underlying cause of admission.
Our study revealed that a significant proportion of patients, approximately 46.3%, required mechanical ventilation support. These findings are consistent with those of a previous study conducted by Sailaja, et al., which reported that 54.9% of their patient cohort required ventilatory assistance [11]. These high rates of mechanical ventilation support highlight the severity of the underlying conditions and the need for effective management and treatment. It is important for healthcare providers to closely monitor and manage ventilated patients to prevent potential complications and to optimize patient outcomes.
The majority of obstetric patients admitted to our surgical critical care unit had an average length of stay of three days, with only a few patients staying for more than six days. These findings suggest that there is a higher likelihood of early discharge from the ICU for this patient population. However, it is important to note that the length of stay in the ICU may be influenced by several factors such as the severity of illness, the need for specialized care, and the availability of resources. Moreover, early discharge from the ICU should be done with caution and based on careful consideration of the patient’s condition and ongoing needs. Further research is needed to identify strategies for optimizing patient care and facilitating safe and timely discharge from the ICU. These efforts should take into account the unique needs and challenges associated with the care of obstetric patients in the surgical critical care setting.
Of the 54 patients admitted to our surgical critical care unit, 46 patients, or 85.2%, survived to discharge. While these results are promising, it is important to note that this study is single-centre and the survival rate may be influenced by a variety of factors such as patient demographics, severity of illness, and treatment modalities. Moreover, this study only accounts for short-term survival and further follow- up is needed to assess long-term outcomes. Despite these limitations, our study provides valuable insights into the management and care of critically ill surgical patients, and highlights the importance of continued efforts to improve patient outcomes in this population. Future multi-centre studies and collaborations may provide further insights into the factors contributing to improved survival rates and guide the development of evidence-based interventions and guidelines for surgical critical care patients.
Limitation of the Study
As a single-centre retrospective study, our findings cannot be generalized to a national or international level. A prospective multicentre study would be valuable in providing additional insights and understanding. Such a study would enable the collection of more comprehensive data from diverse patient populations, and help to identify potential variations in practice and outcomes across different settings. Ultimately, a larger, more comprehensive study would provide greater understanding and insight into the management and care of the patient population of interest.
Conclusion
Despite being a tertiary care rural hospital with limited resources, we were able to effectively manage critical obstetric patients. However, there is still room for improvement in reducing mortality rates. Education can help to ensure that all healthcare providers are knowledgeable about the latest evidence-based practices and guidelines for the management of obstetric emergencies. Additionally, a multidisciplinary approach can facilitate more effective communication and coordination of care among different healthcare professionals involved in the patient’s care. These efforts can ultimately lead to improved patient outcomes and reduce the burden of critical obstetric complications in rural areas.
References
-
Kilpatrick SJ, Matthay MA (1992) Obstetric patients requiring critical care. A five-year review. Chest 101(5): 1407-1412.
-
Pandya ST, Mangalampally K (2018) Critical care in obstetrics. Indian J Anaesth 62(9): 724-733.
-
Tiruneh AG, Asaye MM, Solomon AA, Arega TD (2021) Delays during emergency obstetric care and their determinants among mothers who gave birth in South Gondar zone hospitals, Ethiopia. A cross-sectional study design. Glob Health Action 14(1): 1953242.
-
Bale JR, Stoll BJ, Lucas AO (2003) Reducing Maternal Mortality and Morbidity. In: Bale JR, et al. (Eds.), Improving Birth Outcomes: Meeting the Challenge in the Developing World. National Academies Press, Washington, USA, pp: 372.
-
Fournier P, Dumont A, Tourigny C, Dunkley G, Dramé S, et al. (2009) Improved access to comprehensive emergency obstetric care and its effect on institutional maternal mortality in rural Mali. Bull World Health Organ 87(1): 30-38.
-
Sivaram M, Richard J, Rao PS (1995) Early marriage among rural and urban females of south India. J Biosoc Sci 27(3): 325-331.
-
Vora KS, Koblinsky SA, Koblinsky MA (2015) Predictors of maternal health services utilization by poor, rural women: a comparative study in Indian States of Gujarat and Tamil Nadu. J Health Popul Nutr 33: 9.
-
Rustagi R, Basu S, Garg S, Singh MM, Mala YM, et al. (2021) Utilization of antenatal care services and its sociodemographic correlates in urban and rural areas in Delhi, India. Eur J Midwifery 5: 40.
-
Bhartia A, Dhar RSG, Bhartia S (2020) Reducing caesarean section rate in an urban hospital serving women attending privately in India - a quality improvement initiative. BMC Pregnancy Childbirth 20(1): 556.
-
Pravina P, Ranjana R, Goel N (2022) Cesarean Audit Using Robson Classification at a Tertiary Care Center in Bihar: A Retrospective Study. Cureus 14(3): e23133.
-
Sailaja KB, Renuka MK (2019) Critically Ill Obstetric Admissions to an Intensive Care Unit: A Prospective Analysis from a Tertiary Care University Hospital in South India. Indian J Crit Care Med 23(2): 78-82.
- Editorial on Multimodal Analgesia
- Surgical Incision Site Local Anaesthetic Infiltration and Superior Hypogastric Plexus Block in Total Abdominal Hysterectomy Under General Anaesthesia- A Placebo-Controlled, Randomized Clinical Trial
- Supraglottic Airway Insertion in Semi Fowler Position Due to Severe Thoracic Hyperkyphosis: A Case Report
- Anaesthetic Management of Cardiac Myxoma Patient with Systemic Involvement: A Case Report
- Current Problems in Pulmonary Respiratory Distress Syndrome (Literature Review)
- Evolution of Perioperative Hemodynamic Monitoring from the Hand on Pulse to Hypotension Prediction Index