Impact of Personal Protective Equipment in the Covid-19 Era: A Study of Health Workers in Ghana
COVID-19 has become well-known in the world. The measures to kill the virus have also become hard to come by. Personal Protective Equipment (PPE) has been using by health workers to contain the virus in Ghana hence the study sought to ascertain the impact of Personal Protective Equipment on Ghanaian health workers in the COVID-19 era. The study used primary and secondary sources of data. Importantly, a simple random sampling technique was used to engage a total of 2,420 health workers in Ghana, and also convenience sampling technique was used to select 150 public hospitals and 150 private hospitals for the study. The study used both questionnaires and in-depth interviews to gather the required information. The information obtained from the participants was analyzed by content and statistical analysis. It was revealed that health workers have been using Personal Protective Equipment frequently to contain the spread of the COVID-19 virus in the health care setting in Ghana. It was recommended that health workers should use the Personal Protective Equipment according to indication. Intensive monitoring was also recommended to check the proper uses of the Personal Protective Equipment by health workers in Ghana. Lastly, a sensitization programme was recommended to give more insight on the importance of using Personal Protective Equipment by health workers in Ghana.
Introduction
In more recent years, scientific personal protective equipment is generally believed to have begun with the cloth facemasks promoted by Wu Lien-teh between the years of 1910 and 1911 mainly to prevent the spread of Manchurian pneumonic plague. In the hierarchy of controls, personal protective equipment is considered the least satisfactory method in the prevention of work-related injury or illness and is only to be used when other measures are not feasible or cannot be implemented immediately [1].
Personal Protective Equipment commonly known as “PPE” refers to a vast group of products designed to protect users against low-level, medium-level, and high-level hazards. Personal protective equipment is the equipment used to minimize exposure to hazards that cause serious workplace injuries and illnesses. These injuries and illnesses may result from contact with chemical, radiological, physical, electrical, mechanical, or other workplace hazards. Personal protective equipment may include items such as gloves, safety glasses, shoes, earplugs, respirators, overalls, safety helmets, safety footwear and harnesses, eye protection, and high-visibility clothing. Personal Protective Equipment is needed when there are hazards present. PPE has the serious limitation that it does not eradicate the hazard at the source and may result in wearers being exposed to the hazard if the equipment fails. Any item of PPE imposes a barrier between the wearer and the working environment. This can create additional strains on the wearer; impair their ability to carry out their work and create significant levels of discomfort. Good ergonomic design can help to minimize these barriers and can therefore help to ensure safe and healthy working conditions through the correct use of PPE.
COVID-19 is an infectious respiratory disease caused by a novel coronavirus [2]. Coronavirus simply called COVID-19 is a large group of viruses that is common among animals. It was first identified amid an outbreak of respiratory illness cases in Wuhan City, Hubei Province, China. It was initially reported to the World Health Organisation on December 31, 2019. On January 30, 2020, the World Health Organisation declared the COVID-19 outbreak a global health emergency. On March 11, 2020, the World Health Organisation again declared COVID-19 a global pandemic [3].
The virus replicates efficiently in the upper respiratory tract and appears to cause a less abrupt onset of symptoms than the common cold, which means that infected health workers carry on usual activities for longer, increasing asymptomatic transmission of infection [4]. The virus is primarily transmitted between people through respiratory droplets and contaminated objects; airborne transmission may be possible in specific circumstances where aerosol- generating procedures (AGP), such as suctioning, are performed [5].
The ability to limit the transmission of COVID-19, the disease caused by the novel coronavirus, in the world setting requires infection prevention and control measures, of which Personal Protective Equipment is a fundamental element [6]. This is essential to limit the acquisition and transmission of the virus to protect health workers and the wider community [7]. Personal Protective Equipment such as gloves, aprons, eye protection, masks, and gowns function as a physical barrier to the transmission of infectious particles present in bodily fluids. When used properly and with other infection control practices such as hand-washing, using alcohol-based hand sanitizers, and covering coughs and sneezes, it minimizes the spread of infection from one person to another [8].
The demand for Personal Protective Equipment has soared globally to unprecedented levels. During the 1st quarter of 2020, UN agencies have collectively delivered over 6.4 million gloves, 1.8 million surgical masks, and 1 million gowns to countries across the world, in addition to several other products to meet the country’s requirements. However, there remains a significant gap between the volumes forecasted for country demands over the coming next few months and the products available in the pipeline [9].
A health worker delivers care and services to the sick and ailing either directly as doctors and nurses or indirectly as aides, helpers, laboratory technicians, or even medical waste handlers. There are approximately 59 million health workers worldwide. The health industry is one of the most hazardous environments to work in. Employees in this industry are constantly exposed to a complex variety of health and safety hazards in the course of their work. Hazards range from biological exposure to disease-causing organisms such as tuberculosis and human immunodeficiency virus (HIV) or exposure to chemicals such as glutaraldehyde and ethylene dioxide. Apart from physical hazards such as exposure to radiation and noise, there are also ergonomic issues such as heavy lifting and standing for long periods. Long working hours and shift work add to the stress of work. A health worker needs protection from these workplace hazards just as much as any other category of workers such as miners or construction workers. The World Health Report 2006 reported a severe health workforce shortage especially in 57 countries, mostly in Africa and Asia. Fear of contracting infectious diseases is primarily responsible for high attrition rates among health workers [10].
Health workers are the backbone of effective health systems – they are often based in the community and come from the community they serve, they play a critical role in providing a local context for proven health solutions, and they connect families and communities to the health system. Health workers are those directly providing services where they are most needed, especially in remote and rural areas. Many are community health workers and midwives, though they can also include local pharmacists, nurses, and doctors who serve in community clinics near people in need. They are the first and often the only link to health care for millions of people, are relatively inexpensive to train and support and are capable of providing many life-saving interventions. Health workers provide immunizations and treat common infections. They also help families identify conditions that require higher levels of care and provide a link to that referral care. Families rely on these workers as trusted sources of information who have valuable skills in preventing, treating, and managing a variety of leading killers including diarrhea, pneumonia, malaria, HIV, and tuberculosis. Health workers are also increasingly critical to addressing diseases like diabetes and heart disease that impact the health and productivity of adults around the world. Primarily women, they have become a true force for good, revered in the communities they serve. Simply put, without health workers, there would be no health services for millions of families in low- and middle-income countries.
According to the World Health Organization, 2020, in the health care settings, the main Infection Prevention and Control (IPC) strategies to prevent or limit COVID-19 transmission include the following; ensuring triage, early recognition, and source control (isolating suspected and confirmed COVID-19 patients); applying standard precautions for all patients and including diligent hand hygiene; implementing empiric additional precautions (droplet and contact and, wherever applicable for aerosol-generating procedures and support treatments, airborne precautions) for suspected and confirmed cases of COVID-19; implementing administrative controls; using environmental and engineering controls.
Standard precautions are meant to reduce the risk of transmission of blood borne and other pathogens from both recognized and unrecognized sources. The basic level of infection control precautions to be used, as a minimum, in the care of all patients. Additional transmission-based precautions are required by health care workers to protect and prevent transmission in the health care setting. Contact and droplet precautions are implemented by health workers caring for patients with COVID-19 at all times. Airborne precautions are applied for aerosol-generating procedures and support treatments. The use of PPE is the most visible control used to prevent the spread of infection. In the absence of effective administrative and engineering controls, PPE has limited benefits [5].
The study covered areas such as categories of PPEs, suitable categories of PPEs use by health workers, the role of the Food and Drug Authority in regulating PPEs for health workers, the efficacy of Personal Protective Equipment by health workers, the limitations of Personal Protective Equipment by health workers and other control measures to supplement the use of Personal Protective Equipment by health workers in the COVID-19 Era in Ghana.
Coronavirus has become the only issue that has captured the general concerns of Nations. This has brought the means to research the impact of PPEs in the COVID-19 era. The
Source: Ghana Health Service DHIMS2, 2017.
gracious institution that has performed unprecedented duty in the fight against COVID-19 is the health fraternity. Therefore, there is the need to link the study to health workers in the hospitals of the previous ten (10) regions of Ghana to ascertain how best the PPEs have contributed to the prevention of COVID-19.
The outcomes of the study could serve as a good step to prompt health workers about the benefits of PPEs at the workplaces in the COVID-19 era. Importantly, the Government of Ghana could also get its share from the study by seeing the realistic recommendations to create suitable policies to encourage and favour both domestic and foreign investors in the production of PPEs in Ghana to make them available to all Ghanaians to prevent the spread of the COVID-19 and also increase the revenue margins of Ghana as investors will be obliged to pay taxes to the government and in so doing job opportunities will also be created to employ Ghanaians and reduce the unemployment rate as well.
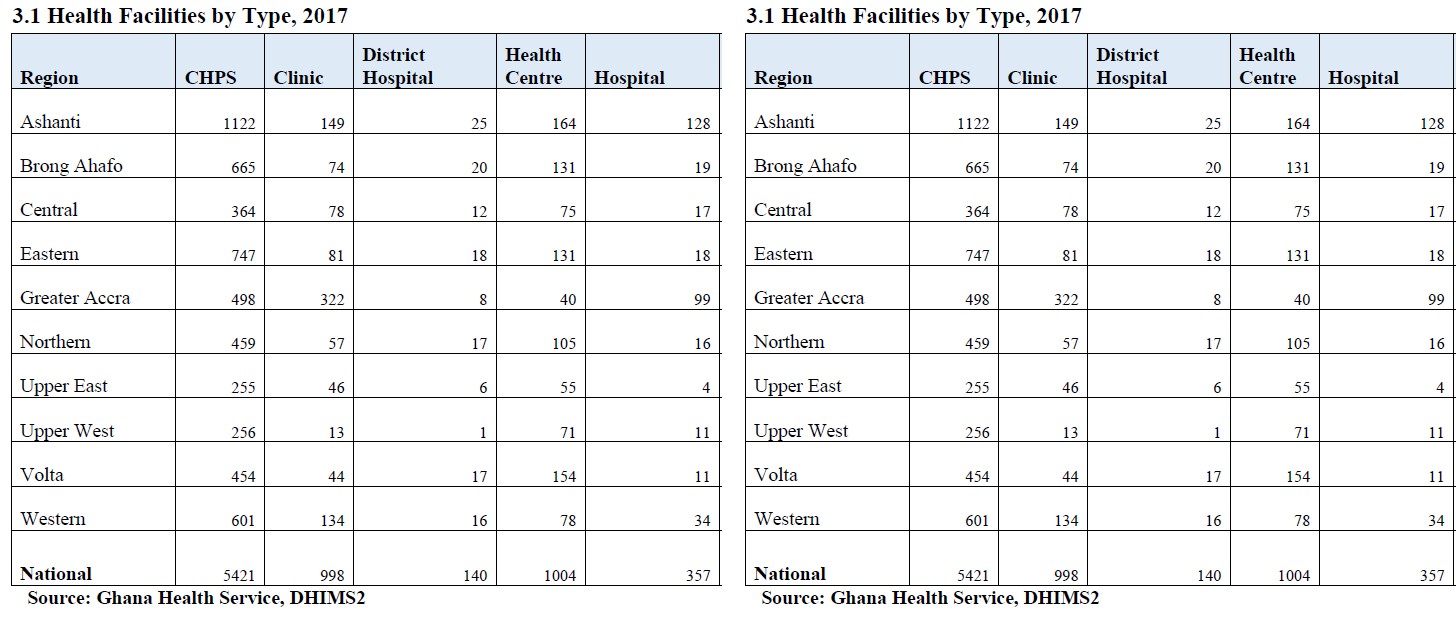
Data on Hospitals in Ghana
According to the Ghana Statistical Service 2010 Population Census, Ghana had a projected population of 29,614,337 with diversified people with unique common goals and objectives. Ghanaian engage in all the economic activities namely primary, secondary, and tertiary. For Ghanaians to be protected healthily there must be well- built hospitals that could provide health services to them. Statistically, concerning Ghana Health Service DHIMS2 in 2017 that revealed the health facilities by type, Ghana had 357 hospitals with the below regional breakdown;
Data on Health Workers in Ghana
There are about 52,258 individuals currently formally working in the health sector in public, CHAG, private, Islamic Missions, quasi-government and other organizations in Ghana. The MOH employs 42,299 staff in GHS, teaching hospitals, CHAG, and health training institutions, regulatory bodies, and headquarters. This number represents about 81.5% of the total health sector workforce. Non-clinical support staff, including administrators, accountants, drivers, and technicians; and clinical support staff including health aides and ward assistants constitute about 38% of the total workforce officially employed. Apart from the total workforce informal employment, about 21,791 people countrywide are registered as engaged in traditional medicine, while 367 persons are registered as traditional birth attendants (TBAs). This indicates that about 69,000 people are known to be involved in health care delivery country-wide [11].
Distribution of Health Workers in Ghana
The distribution of health workers is skewed in favour of the more affluent regions, most of which are in the southern half of the country. The highly skilled professionals like medical doctors and specialized personnel (nurses, pharmacists, allied health professionals, etc) are concentrated in the Greater Accra region, as well as in Korle Bu and Komfo Anokye Teaching Hospitals. The two teaching hospitals (Korle Bu and Komfo Anokye) employ more than 45% of the country’s doctors while less than 15% are present in the district hospitals. The southern sector of the country where social amenities are concentrated, attracts most of the trained health staff, thus reducing further the possibilities of enhancing service delivery in the rural areas where more than 65% of the population live. The quality of health care delivery at this level is compromised by low staff competencies in maternal and child health management, poor lifesaving skills of midwives, poor record-keeping on ANC clients, and non-follow-up of post-natal care clients. Majority of the highly skilled health staff are in the public sector. The private self-financing sector, however, employs 10% of Ghana’s health workforce, mostly in urban areas. The private sector has a large number of health facilities, yet they appear to have a proportionately smaller number of staff than the public sector [11].
The Current State of Supply of Personal Protective Equipment in the World
China is the largest producer of Personal Protective Equipment finished products, as well as of many of the raw materials needed to manufacture these products. China produced an estimated 50 percent of surgical masks globally (estimated to be 20 million masks a day, pre-pandemic).
Taiwan alone makes up 20 percent of the global supply of face masks, while other countries with PPE production capacity include India, Japan, Korea, Malaysia, Mexico, Thailand, United States (US), and several European countries. China reportedly boosted the production of masks more than five- fold earlier this year, providing a daily production capacity of 110 million units, and has likely increased production further since that time. Face masks, including surgical masks and N95 respirators, have been facing the largest supply constraints since the COVID-19 outbreak has worsened. The majority of stocks normally held by manufacturers, wholesalers, and distributors have been depleted in addition to an increasing order backlog [9]. Due to the extremely high demand for IPC and Personal Protective Equipment supplies and limited supply availability, existing UNICEF suppliers are not able to meet UNICEF’s demand. From the beginning of March 2020, there have been signs of improvement in PPE supply availability, in part as a result of China’s production normalizing. Manufacturers in China have indicated that their production lines are up and running but depend on access to raw materials, highlighting the concern and the importance of securing the raw materials for face masks, gowns, and coveralls. On the other hand, the government of India has extended its export ban to all Personal Protective Equipment products including raw materials, such as non-woven fabrics used to manufacture face masks and other protective clothing. That has been followed by an export ban in many other countries. During March and April 2020, UNICEF increased its ‘pipeline’ of contracted supply from thousands of units to the scale of millions of units of Personal Protective Equipment products scheduled for delivery in March, April, and May 2020. Despite markets now facing severe disruptions and significantly increased pricing pressure, UNICEF has been able to maintain reasonable prices across the different PPE commodities [9].
UNICEF has reached out to more than 1,000 suppliers (including manufacturers and wholesalers) and industry leaders globally, to find a solution to current market constraints. Despite the extreme market conditions, including aggressive buying, since the end of January, UNICEF has successfully managed to secure availability from suppliers for key products, such as 50 million surgical masks, 24 million respirators, 6.9 million coveralls, 3.6 million surgical gowns, 1.9 million goggles, 110,000 infrared thermometers, and 31.6 million face shields, among many other items, of which a portion has already been delivered and supplied to countries. However, the majority of PPE that has been procured are scheduled for delivery from April - June 2020, of which over 90 percent are being produced and shipped out of China. UNICEF has noted many new market entrants have been seeking to supply through UN aid agencies. These manufacturers and sellers are unfamiliar with UN procurement guidelines and many have offered unfavorable commercial terms (e.g., very high prices, significantly advanced payments, with offer validity for 24 hours) to secure production capacity. Despite advance payments, UN aid agencies have noted that some suppliers are failing to deliver on supplies after confirming orders or are canceling purchase orders – causing further disruptions to the COVID-19 response efforts in low-income and middle- income countries [9].
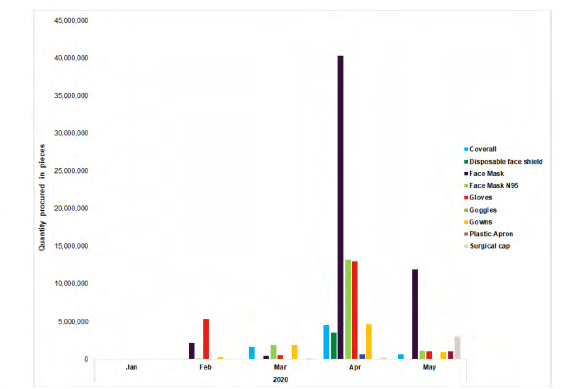
Source: UNICEF, 2020 Figure 1: Supply contracted through UNICEF (January-May 2020). The COVID-19 outbreak has had a major impact on global logistics in part due to reduced air freight capacity but also reduced workforces at airports, ports, and warehouses. Logistics services have also been impacted by decisions of local authorities to shut down logistics infrastructure to enforce movement restrictions or put in place additional requirements to suppress virus transmission. This has considerably hindered UNICEF’s supply operations. While humanitarian waivers and exceptions have been negotiated by UNICEF and its partners for either export permits or chartered flights, this has added further costs and delays to supply pipelines. Despite the international transport challenges, UNICEF’s freight forwarding service partners in China have fully resumed facilitating the international shipment of goods produced in China [9].
Disruptions in The Global Supply Chain of Personal Protective Equipment
The current global stockpile of PPE is insufficient, particularly for medical masks and respirators, and the supply of gowns, goggles, and face shields is now insufficient to satisfy the global demand. Surging global demand- driven not only by the number of COVID-19 cases but also by misinformation, panic buying, and stockpiling has resulted in further shortages of PPE globally. The capacity to expand PPE production is limited, and the current demand for respirators and masks cannot be met, especially if widespread inappropriate use of PPE continues. However, with manufacturing companies in some of the main exporting countries restarting their production and an established global coordination mechanism that WHO anticipates will contribute to addressing the global shortage. Dedicated assistance and international solidarity mechanisms are required to meet the needs of the most vulnerable countries, which may face affordability issues in the context of rising prices determined by an unprecedented surge in demand, coupled with supply and distribution disruptions [5].
Preventive Measures for COVID-19 Disease
Based on current evidence, the COVID-19 virus is transmitted between people through close contact and droplets. Airborne transmission may occur during aerosol- generating procedures and support treatments [12]; thus, WHO recommends airborne precautions for these procedures. For all, the most effective preventive measures include:
• Maintaining physical distance (a minimum of 1 meter) from other individuals;
• Performing hand hygiene frequently with an alcohol- based hand rub if available and if your hands are not visibly dirty or with soap and water if hands are dirty;
• Avoiding touching your eyes, nose, and mouth;
• Practicing respiratory hygiene by coughing or sneezing into a bent elbow or tissue and then immediately disposing of the tissue;
• Wearing a medical mask if you have respiratory symptoms and performing hand hygiene after disposing of the mask;
• Routine cleaning and disinfection of environmental and other frequently touched surfaces.
The Role of the Food and Drug Authority in Regulating Personal Protective Equipment for Health Workers in the COVID-19 Era in Ghana
All Personal Protective Equipment (PPE) that is intended for use as a medical device must follow the FDA’s regulations and should meet applicable voluntary consensus standards for protection. This includes surgical masks, N95 respirators, medical gloves, and gowns. The consensus standards and the FDA’s requirements vary depending on the specific type of PPE. When these standards and regulations are followed, they provide reasonable assurance that the device is safe and effective. Some PPEs are reviewed by the FDA before they can be legally sold [13, 14, 15, 16, 17]. In this review, known as Premarket Notification or 510(k) clearance, the manufacturers have to show they meet specific criteria for performance, labeling, and intended use to demonstrate substantial equivalence.
Materials and Methods
Case study research design was used to get concrete information from the field of the study. Importantly, a case study was selected to deliver richer facts to substantiate the study. Qualitative and quantitative approaches were used to gather both qualitative and quantitative data to support the study strategically. Methodologically, random, and non-random sampling techniques were used to select respondents and hospitals respectively for the study. A simple random sampling technique was employed to choose 2,240 respondents from the health fraternity in Ghana. The convenience sampling technique was also used to select three hundred (300) hospitals in Ghana thus, one hundred and fifty (150) public hospitals and one hundred and fifty (150) private hospitals. The researchers took the opportunity to travel to all the previous ten (10) regions.
The data analysis was done through qualitative and quantitative methods. Qualitative data analysis was done through content analysis whiles quantitative data analysis was executed through the aid of Statistical Packages for Social Sciences (SPSS) computer software. Respondents’ expressions were presented in italics with quotation marks. Numerically, 1,120 health workers were scheduled to participate in the questionnaire administration. Again, another 1,120 health workers were also selected to involve in the interview section.
The target population of the study was health workers in the various hospitals in Ghana but the accessible population was also biomedical scientists, community health nurses, health assistants, medical assistants, medical officers, midwives, pharmacists, professional nurses, and specialists. The study used both primary and secondary sources of data. The primary data were gathered through questionnaires and in-depth interviews. The questionnaires were drawn from the following sections; • Categories of Personal Protective Equipment.
• Categories of Personal Protective Equipment for COVID-19.
In-depth interviews were granted by the researchers on the below aspects; • Efficacy of Personal Protective Equipment by health workers in the COVID-19 Era in Ghana.
• Limitations of Personal Protective Equipment by health workers in the COVID-19 Era in Ghana. Secondary data for the study was gathered from published and unpublished articles on PPEs in the COVID-19 era. The study was executed between March 2020 and March 2021 but the field data collection was carried out within February 2021. This means that the study was completed within twelve (12) months. Factually, the study was self- financed by the researchers hence this instigated the use of convenience sampling technique in the selection of hospitals in the previous ten (10) regions where hospitals that were closed to the researchers’ bus stop were conveniently engaged in the study.
Results and Discussions
| Frequency | Percentage | |
|---|---|---|
| Sex | ||
| Male | 1129 | 53% |
| Female | 1141 | 47% |
| Total | 2420 | 100% |
| Marital Status | ||
| Married | 1000 | 41% |
| Single | 1321 | 55% |
| Divorced | 2420 | 100% |
| Age | ||
| 18-30 | 422 | 17% |
| 31-60 | 1198 | 83% |
| Total | 2420 | 100% |
| Length of Service | ||
| 1-20 | 1116 | 46% |
| 21-40 | 1304 | 54% |
| Total | 2420 | 100% |
| Educational background | ||
| Degree | 980 | 40% |
| Diploma | 890 | 37% |
| Certificate | 550 | 23% |
| Total | 2420 | 100% |
| Region | ||
| Ashanti | 480 | 20% |
| Brrong Ahanfo | 130 | 5% |
| Central | 180 | 7% |
| Eastern | 170 | 7% |
| Greater Accra | 600 | 25% |
| Northern | 120 | 5% |
| Upper East | 100 | 4% |
| Upper West | 130 | 5% |
| Volta | 110 | 5% |
| Western | 400 | 17% |
| Total | 2420 | 100% |
| Categories of health workers | ||
| Biomedical scientist | 120 | 5% |
| Community health nurse | 210 | 9% |
| Health assistant | 80 | 7% |
| Medical assistant | 110 | 5% |
| Medical officer | 210 | 9% |
| Midwife | 160 | 27% |
| Pharmacist | 180 | 7% |
| Professional nurse | 560 | 23% |
| Specialist | 200 | 8% |
| Total | 2420 | 100% |
Table 1: Socio-economic characteristics of health workers used in the study. Source: Field data (2021)
From Table 1, 1,279 health workers engaged were males represented 53%. Female health workers engaged were 1,141 denoted 47%. It can be seen that the majority of the health workers who availed themselves to participate in the study were males. Most of the female health workers were not eager to engage in the research which led to the reduced figure shown above. Those female health workers who partook in the questionnaire and interview sections received a lot of encouragement before the interview became successful because they believed the information gathered will be used to take decisions against them. Again, others assumed that their credentials will be revealed to the Ministry of Health that could bring the public dialogue to result in dismissal. Most of the respondents explained that “the PPEs are mostly used more appropriately by females than males”. This is naturally because females have the heart to pay attention to instructions.
Concerning Table 1, 1,000 health workers were married personalities represented 41%. These health workers stressed that “marriage has contributed to good standards of the job because the home becomes sweet and mentally stable when they see their wives and husbands at home waiting for them. They also emphasized that their husbands and wives always advise them to wear PPEs whiles working.” 1,321 health workers represented 55% were singles whiles 99 health workers denoted 4% were divorced. Still Table 1 under the spotlight, 422 health workers were found between the ages of 18-30 represented 17%. Most of the health workers in this age group were singles because they could see “marriage as a lifetime journey that demands adequate preparations. A section of them also lamented that “sometimes they refuse to take their nose masks and hand sanitizers of which they suggested that if married their partners could be remainders in this regard”. Moreover, 1,998 health workers represented 83% were seen between the years of 31-60. This age range frankly expressed that “PPEs have been the major tools in their work to prevent the contraction of the virus because their immune systems have been becoming weak as they grow”. One of the respondents cleared the air that “as they grow their levels of forgetfulness to use the PPEs increase rapidly”. The Health system deals with the general activeness of one’s life therefore lives are given once hence experiences are gotten from the length of services offered.
From Table 1, health workers were tested on the number of years served, 1,116 health workers represented 46% have served between 1-20 years. 1,304 health workers denoted 54% have been able to serve between 21-40 years. It was said that the length of service has a “positive impact on the uses of PPEs because they have been in the system for long and that they understand the dynamisms of using the PPEs. The health workers with 21-40 years of experience indicated that “they have been doing a great job by orienting the newly recruited staff on the impact of PPEs in preventing and containing virus”.
About Table 1, 980 health workers constituted 40% were degree holders. These degree holders comprised the BSc, MSc, MPhil, and Ph.D. Diploma holders were 890 denoted 37%. Many of the respondents were degree holders and males. The degree holders had the confidence to answer interview questions critically and realistically because they have the essence of research in mind. Certificate health workers were proven difficult to be engaged because they presumed the study as a way of gathering their bio- data to the government for unknown decisions but upon counseling, those who were around presented themselves to the researcher. It was revealed that the level of education sometimes determines the absolute observance of the PPEs user instructions in the COVID-19 era. Most of the health workers juxtaposed that education is very important as far as human lives are concerned and that numerous intensive in-service training is ongoing to sensitize health workers on the uses of PPEs in the COVID-19 pandemic.
According to Table 1, 480 health workers represented 20% were engaged in the Ashanti region. Health workers in the Ashanti region were eager to participate in the study because “COVID-19 is seen as a satanic tool to wipe out humankind from the earth”. This assertion motivated them to take part a lot in the study. The Ashanti region recorded the highest diploma holders because “Kwame Nkrumah University of Science and Technology has been their center of learning and also an examining body”. Brong Ahafo region recorded 130 health workers represented 5%. Health workers who met at the Brong Ahafo region were few since on the day of the questionnaire and interview sections turnout was low. A response was written that “most of the health workers were on casual leave”. 180 health workers were recorded for the central region represented 7%. Health workers in the central region were happy to welcome the researcher and provided the required information. The central region recorded the highest degree holders because “The University of Cape Coast has been their Centre of Study in medical programmes”. The Eastern region had 170 health workers who participated in the study represented 7%. Eastern region has nice and prominent health workers who have the work at heart. Health workers in the Eastern region revealed that “management of the health service in the region has put measures in place that encourage the supervision and monitoring of PPEs used by health workers”. Greater Accra had the highest number of health workers of 600 denoted 25%. Greater Accra has the greatest and most eminent health workers who are monitored and supervised by experienced health professionals as in the uses of the PPEs in the COVID-19 era. It was found that “supervision and monitoring are keeping health workers in the Greater Accra region on their toes to strictly adhere to the user instructions of the PPEs”.
Regarding Table 1, the Northern region recorded 120 health workers represented 5%. Health workers in the Northern region were eager to provide more required information on the study. These health workers demonstrated that the “Northern region does not joke with lives in the COVID-19 era”. 100 health workers were recorded in the Upper East region represented 4%. Health workers in the Upper East region were hard to be reached but few who participated did it wholeheartedly. Upper East region has dedicated health workers who have devoted their time to work seriously to prevent and contain the spread of COVID-19. Respondents also revealed that “all human races have been oriented on the use of PPEs to prevent the spread of the virus”. Upper West region recorded 130 health workers represented 5%. Health workers in the Upper West region presented themselves nicely to partake in the questionnaire and interview sections. Respondents politely ordered, “the researcher to put on the nose and face masks appropriately”. This instruction denotes that “health workers in the Upper West region are doing yeoman job to prevent the spread of the COVID-19” . About Table 1, the Volta region recorded 110 health workers represented 5%. Health workers in the Volta region are hardworking as they availed themselves to contribute excessively to the outcome of the study. These health workers are productive in the usage of the PPEs. This is because they revealed that “the spread of the COVID-19 has been controlled in the region through the uses of PPEs”. Western Region had 400 health workers to participate in the questionnaire and interview sections represented 17%. The western region was revealed as “very good in sponsoring health professionals in education. This has made the region receive more health workers during public health service recruitment”. Health workers in the western region are tactically using the PPEs in the right direction since orientations have been organized on the uses of PPEs in the COVID-19 era. The previous ten regions were used instead of 16 regions. This is because health facilities remained in the ten regions since the newly created 6 regions did not have regional health facilities such as regional health directorates as at the time the study was conducted.
From Table 1, 120 biomedical scientists represented 5% were interrogated on the impact of PPEs in the COVID-19 era. It was found that “these health workers have been able to use PPEs as required”. The activity of biomedical scientists requires the use of PPEs in all forms. Community health workers had 210 respondents represented 9%. This category of health workers emphasized that “particularly PPEs cannot be untouched in their services”. This means that PPEs are frequently used in all levels of work. 180 health assistants represented 7% were used in the questionnaire and interview sections. These health workers proved that “PPEs are monumental artifacts to prevent the spread of the COVID-19”. 110 medical assistants denoted 5% were engaged in the questionnaire and interview sections. The medical assistants demonstrated that “they work under the assistance of heads hence PPEs are used instructively to prevent the COVID-19”. Medical officers constituted 210 who partook in the questionnaire and interview sections. These medical officers uncovered that “all works in the department require PPEs hence they are unique”.
Regarding Table 1, 650 midwives represented 27% were involved in the study. The midwives made inputs that “their unit always receive patients from all walks of life, therefore, PPEs are used intensively to prevent the spread of the virus”. 180 pharmacists denoted 7% were engaged in the study. These pharmacists believed that “COVID-19 can be contained by using the PPEs”. 560 professional nurses represented 23% were the second-highest health workers engaged in the study. Professional nurses who took part in the questionnaire and interview sections stressed that “every responsive health care demands the usage of PPEs to prevent virus”. 200 specialists denoted 8% were used in the questionnaire and interview sections. The specialists disclosed that “PPEs are crucial in the execution of their responsibilities hence they cannot be left behind” .
| Frequency | Percentage | |
|---|---|---|
| Respiratory protection | 670 | 28% |
| Eye and face protection | 530 | 19% |
| Hand protection | 450 | 19% |
| Body protection | 200 | 8% |
| Foot protection | 170 | 7% |
| Hearing protection | 150 | 6% |
| Head protection | 120 | 5% |
| Height and access protection | 130 | 5% |
| Total | 2420 | 100% |
Table 2: ** Categories of Personal Protective Equipment.
Source: Field data (2021). Table 2: Categories of Personal Protective Equipment.
According to Table 2, 670 health workers represented 28% pointed out respiratory protection PPEs. Eye and face protection PPEs were selected by 530 health workers represented 22%. 450 health workers denoted 19% chose hand protection PPEs. Body protection PPEs were chosen by 200 health workers connoted 8%. 170 health workers represented 7% selected foot protection PPEs. Hearing protection PPEs were chosen by 150 health workers denoted 6%. 120 health workers represented 5% chose head protection PPEs. Height and access protection PPEs were selected by 130 health workers connoted 5%. It was revealed that there are eight types of personal protective equipment critical for the defense of users. Health workers specified that PPEs can be grouped based on their “uses and defense of users”.
| Frequency | Percentage | |
|---|---|---|
| Eye and face protection | 980 | 40% |
| Hand protection | 460 | 19% |
| Respiratory protection | 430 | 18% |
| Body protection | 280 | 12% |
| Foot protection | 270 | 11% |
Table 3: ** Categories of Personal Protective Equipment for COVID-19.
Source: Field data (2021) Table 3: Categories of Personal Protective Equipment for COVID-19.
Concerning table 3,980 health workers represented 40% selected eye and face protection as a suitable protective body for preventing COVID-19. Hand protection PPEs were chosen by 460 health workers represented by 19%. 430 health workers represented 18% selected respiratory protection PPEs. Body protection PPEs were selected by 280 health workers represented 12%. 270 health workers represented 11% chose foot protection PPEs. It can be induced that PPEs could be used generally for the safety of users. Every organization has its categories of PPEs to be used. Health workers for the sake of the pandemic emphasized that “eye and face protection, hand protection, respiratory protection, body protection, and foot protection are the certified PPEs for preventing COVID-19”.
Health workers engaged in the study were able to give the following expressions for each type of PPE’’s outlined in Table 3.
Hand protection: “The hand protection equipment can ensure protection against viral, bacteriological risks and chemical contamination resulted from COVID-19. Examples are work gloves and gauntlets”. Eye and face protection: Examples are safety glasses and goggles, eye and face shields. Respiratory protection: “The respiratory protection covers a broad group of PPE: breathing apparatus, full face or half- mask respirators, powered respirators, protective hoods, disposal face masks, detectors, and monitors”. Foot protection: “The foot protection equipment is designed to protect the feet and legs against COVID-19. Examples are boots, shoes, anti-static and conductive footwear”.
Body protection: “Ensuring protection against infection, and chemical contamination resulted from COVID-19. For example, overall, and gown” (Figures 1 & 2).
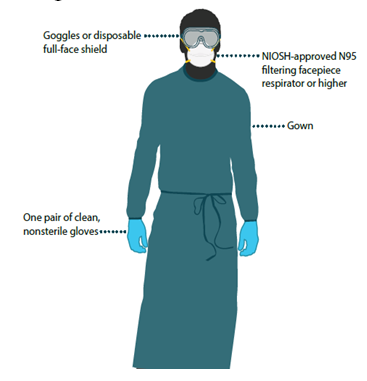
Source: Department of Health and Human Services, US (2020). Figure 1: Image of a health worker with Personal Protective Equipment.

Source: Respirators, 2020 Figure 2: Images of Air-purifying and N95 Respirators.
The Efficacy of Personal Protective Equipment by Health Workers in the COVID-19 Era in Ghana.
Health workers engaged in the study stressed that the efficacy of PPEs is “dependent by conforming to the consensus standards for barrier performance and resistance to tears and snags. Consensus standards may also be used to demonstrate sterility, biocompatibility, fluid resistance, and flammability”. It was also learned that “manufacturers could also contribute to PPEs efficacy by validating or authenticating the methods used to test conformance to standards and also support each product with appropriate performance test data”.
| Frequency | Percentage | |
|---|---|---|
| Discomfort | 1,310 | 54% |
| Inconvenience | 840 | 35% |
| Inadequate selection | 270 | 11% |
| Total | 2420 | 100% |
Table 4: ** The limitations of Personal Protective Equipment by health workers in the COVID-19 Era in Ghana From Table 4, 1,310 h
Source: Field data (2021) Table 4: The limitations of Personal Protective Equipment by health workers in the COVID-19 Era in Ghana From Table 4, 1,310 health workers represented 54% were able to lament that “PPEs have been making them feel very uncomfortable at the workplaces”. The study engaged 840 health workers denoted 35% asserted that PPEs have caused inconveniences at their workplaces in the COVID-19 era simply because “the virus has made PPEs to be used compulsorily at all units in the health fraternity”. The inadequate selection was emphasized by 270 health workers represented 11%. Health workers lamented that “sometimes they choose unmeasured PPEs because they cannot be tested by users based on their suitability”. PPEs have numerous merits to users but there are also limitations that they pose to users. According to the health workers, limitations of PPEs include discomfort, inconvenience, and inappropriate or poorly maintained equipment. Limitations instigated by the inadequate selection, fit, and maintenance will not sabotage the efficacy of the equipment.
Conclusion
Health workers are coping with the Personal Protective Equipment in a way to contain the COVID-19 virus in the various hospitals in Ghana.
Ethical Approval Statement
The research respondents were given a detailed notice that their information are confidential and as such data obtained will not bring any harm to their profession as the researchers will analyses the obtained data professionally. Respondents agreed to provide all the required information to be analyzed by the researchers.
Competing Interest Declaration
Author declares that there are no competing interests in the study.
Recommendations
• The Health workers involved in the direct care of patients should use PPE according to indications.
• The Government of Ghana should make PPEs available to all patients to contain the spread of the COVID-19 in the hospitals.
• Sensitization Programme should be organized on the uses of PPEs for all health workers in Ghana.
• Intensive monitoring should be undertaken to check the uses of PPEs by health workers in Ghana.
References
-
University of Western Australia (2018) Personal protective equipment guidelines: Safety, Health, and Wellbeing_._
-
Public Health England. Guidance (2020) Introduction and organizational preparedness.
-
Gyimah N (2020) Lessons Learnt from Coronavirus (COVID-19) in the World.
-
Heymann DL, Shindo N (2020) WHO Scientific and Technical Advisory Group for Infectious Hazards. COVID-19: what is next for public health?.
-
World Health Organization (2020) Modes of transmission of the virus causing COVID-19: implications for IPC precaution recommendations.
-
Public Health England COVID-19 (2020) epidemiology, virology, and clinical features.
-
Charlotte G, Abigail T (2020) Use of personal protective equipment during the COVID-19 pandemic. British Journal of Nursing 29: 13.
-
Brown L, Munro J, Rogers S (2019) Use of personal protective equipment in nursing practice. Nurs Stand 34(5): 59-66.
-
UNICEF (2020) COVID-19 impact assessment and outlook on personal protective equipment.
-
Bobby J, Merlyn J (2016) The health of healthcare workers_._ Indian Journal of Occupational and Environmental Medicine 20(2): 71-72.
-
Ghana Health Workforce Observatory (2010) Human Resources for Health Country Profile.
-
Tran K, Cimon K, Severn M, Pessoa Silva CL, Conly J (2012) Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: A systematic review.
-
CDC (2020) Department of Health and Human Services, US.
-
Gyimah N (2020) Effect of Partial Lockdown on Food Security during the Coronavirus (COVID-19): The Case of Capital City of Ghana, Accra_._
-
N95 Respirators and Surgical Masks and barrier face coverings (2020).
-
The FDA’s role in regulating Personal Protective Equipment (2021).
-
World Health Organisation (2020) Rational use of personal protective equipment for coronavirus disease (COVID-19) and considerations during severe shortages_._
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths