Co-occurrence of Rheumatoid Arthritis and Pulmonary Tuberculosis: A Diagnostic and Therapeutic Challenge
The co-occurrence of rheumatoid arthritis (RA) and pulmonary tuberculosis (TB) poses diagnostic and therapeutic challenges in patients receiving immunosuppressive therapy. In this case report, we present a 45-year-old male with a history of multiple joint pain for 8 years, suggestive of RA. The patient had been taking NSAIDs for 3 years, but his symptoms worsened in the last month. Laboratory investigations revealed elevated levels of rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti- CCP) antibodies, supporting the diagnosis of RA. He was initiated on methotrexate, hydroxychloroquine, and folate. However, he developed respiratory symptoms, including a productive cough and fever. Physical examination findings indicated respiratory abnormalities and radiographic imaging showed bilateral opacities. Further assessment with HRCT thorax revealed fibrocavitary lung lesions and mediastinal lymphadenopathy. Microbiological confirmation through CBNAAT testing demonstrated the presence of Mycobacterium tuberculosis, leading to the diagnosis of pulmonary Tuberculosis. The patient was promptly started on anti-tubercular treatment. This case highlights the challenges faced in managing patients with both RA and TB under immunosuppressive therapy. A multidisciplinary approach involving rheumatologists and infectious disease specialists is crucial for optimal management and favourable outcomes.
Introduction
Rheumatoid arthritis is a systemic autoimmune disease characterized by chronic inflammation of the synovial membrane in peripheral joints [1]. It predominantly affects women and has a higher incidence in the age range of 30-
50 years, with symmetrical involvement of both small and large joints, especially the hands and feet [2]. In patients with rheumatoid arthritis, tuberculosis (TB) is more commonly found than in those with other forms of arthritis. The use of immunosuppressive agents is the cornerstone of rheumatoid arthritis treatment. However, these medications can increase the risk of reactivating latent TB infection. Hence, it is crucial to exercise caution when administering immunosuppressive agents to individuals who have been infected with tubercular bacilli [3]. We present a case report of a 45-year-old male initially diagnosed with rheumatoid arthritis who commenced immunosuppressive therapy. However, he later developed respiratory symptoms and was ultimately diagnosed with pulmonary tuberculosis. This case emphasizes the challenges encountered when managing two conditions simultaneously, where the treatment of one condition increases the vulnerability and severity of the other.
Case findings
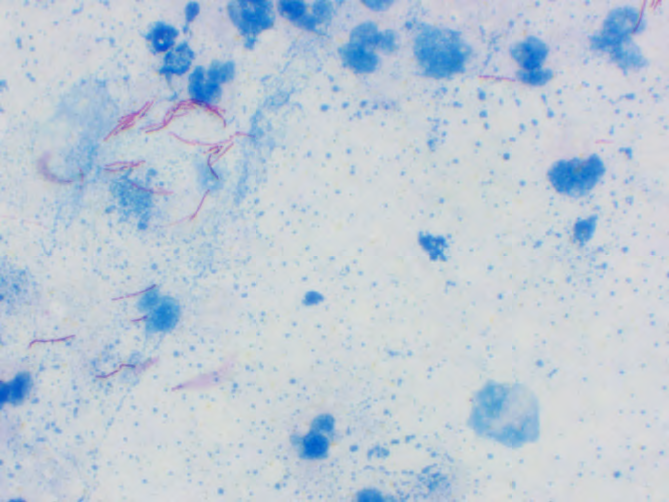
A 45-year-old male presented with multiple joint pains involving both small and large joints for the past 8 years. He had been taking NSAIDs for the last 3 years. However, his joint pain worsened over the last month, prompting an investigation for Rheumatoid factor (RF) and Anti-CCP antibodies. It should be noted that Rheumatoid factor is not specific to Rheumatoid arthritis alone, as it can also be observed in cases of chronic infection and other systemic inflammatory conditions. On the other hand, Citrullinated protein antibodies (Anti-CCP) are highly specific for rheumatoid arthritis. The Rheumatoid factor was measured to be 110, and the Anti-CCP level was 220. In response, the patient was prescribed Methotrexate, Hydroxychloroquine, and Folate. However, he developed a productive cough and fever. During the examination, his pulse rate was 134/ min, respiratory rate was 24/min, blood pressure was 102/70 mmHg, and oxygen saturation (SpO2) was 90% on room air. On auscultation, bilateral rhonchi and coarse wet crepitation’s were detected. Subsequently, a chest X-ray was performed, which revealed non-homogeneous bilateral opacities. Further assessment with HRCT Thorax showed multiple fibro-cavitary lung parenchymal lesions in both lung fields, along with significant-sized superior and middle mediastinal lymphadenopathy. To confirm the diagnosis microbiologically, the patient’s sputum was sent for smear testing, which yielded a positive result for Mycobacterium Tuberculosis (Figure 1). As a result, the patient was started on antitubercular treatment.
Discussion
The presented case report describes a challenging clinical scenario involving a 45-year-old male with established rheumatoid arthritis (RA) who developed an opportunistic pulmonary tuberculosis (TB) infection while under immunosuppressive therapy. This case emphasizes the complexity of managing patients with rheumatoid arthritis who are at an increased risk of developing infectious complications, particularly tuberculosis, due to the use of immunosuppressive agents. Rheumatoid arthritis is a chronic autoimmune disease characterized by systemic inflammation and synovial joint involvement. The hallmark of RA is symmetrical polyarthritis affecting both small and large joints [1]. The diagnosis of RA is supported by the presence of specific serological markers, such as elevated rheumatoid factor (RF) and anti-cyclic citrullinated peptide (anti-CCP) antibodies, as observed in this case [4]. These laboratory findings, along with the clinical presentation of longstanding joint pain, lead to the initiation of disease-modifying ant rheumatic drugs (DMARDs) including methotrexate, hydroxychloroquine, and folate [5]. Tuberculosis is a granulomatous infectious disease caused by Mycobacterium tuberculosis. Reactivation of latent tuberculosis infection (LTBI) is a well-documented complication in patients receiving immunosuppressive therapy, particularly when combined with corticosteroids or tumour necrosis factor- alpha (TNF-α) inhibitors [6].
In this case, the patient’s clinical course was complicated by the development of respiratory symptoms, including a productive cough and fever. Physical examination findings revealed abnormal respiratory sounds, such as bilateral rhonchi and coarse wet crepitation’s, suggesting pulmonary involvement. Radiological imaging, including chest X-ray and HRCT thorax, demonstrated non-homogeneous bilateral opacities and multiple fibro-cavitary lung lesions in both lung fields, respectively. These findings raised concerns regarding a potential pulmonary infection, prompting further investigation [7].
Microbiological confirmation was obtained through the CBNAAT test of the patient’s sputum, which revealed the presence of Mycobacterium tuberculosis, confirming the diagnosis of pulmonary tuberculosis [8]. Prompt initiation of antitubercular treatment was warranted to address the active tuberculosis infection. The management of the patient required a coordinated effort involving rheumatologists and infectious disease specialists to balance the need for immunosuppression in rheumatoid arthritis management while addressing the infectious complication.
The case highlights the importance of considering tuberculosis as an opportunistic infection in patients with rheumatoid arthritis receiving immunosuppressive therapy. Rheumatoid arthritis is associated with an increased risk of developing tuberculosis, and immune suppressive agents further augments this risk. Therefore, a thorough evaluation of latent tuberculosis infection should be performed before initiating immunosuppressive therapy, and appropriate preventive measures should be taken in individuals with latent tuberculosis infection [3].
Close monitoring and early recognition of infectious complications are vital in patients receiving immunosuppressive therapy. Prompt diagnosis and initiation of appropriate treatment for tuberculosis in this case were crucial in preventing disease progression and minimizing potential complications. In conclusion, this case report highlights the challenges faced in managing a patient with rheumatoid arthritis who developed an opportunistic tuberculosis infection while under immunosuppressive therapy. It underscores the importance of diligent evaluation, monitoring, and coordination among healthcare professionals involved in the care of these patients to achieve optimal outcomes. Further research and awareness are needed to improve preventive strategies and management guidelines for tuberculosis in patients with rheumatoid arthritis receiving immunosuppressive therapy.
References
-
Guo Q, Wang Y, Xu D, Nossent J, Pavlos NJ, et al. (2018) Rheumatoid arthritis: pathological mechanisms and modern pharmacologic therapies. Bone Res 6: 15.
-
Kobak S, Bes C (2018) An autumn tale: geriatric rheumatoid arthritis. Ther Adv Musculoskelet Dis. 10(1): 3-11.
-
Ji X, Hu L, Wang Y, Man S, Liu X, et al. (2022) Risk of tuberculosis in patients with rheumatoid arthritis treated with biological and targeted drugs: meta- analysis of randomized clinical trials. Chin Med J (Engl) 135(4): 409-415.
-
Taylor P, Gartemann J, Hsieh J, Creeden J (2011) A Systematic Review of Serum Biomarkers Anti-Cyclic Citrullinated Peptide and Rheumatoid Factor as Tests for Rheumatoid Arthritis. Autoimmune Dis 2011(1): 815038.
-
Lopez-Olivo MA, Siddhanamatha HR, Shea B, Tugwell P, Wells GA, et al. (2014) Methotrexate for treating rheumatoid arthritis. Cochrane Database Syst Rev 2014(6): CD000957.
-
Köhler BM, Günther J, Kaudewitz D, Lorenz HM (2019) Current Therapeutic Options in the Treatment of Rheumatoid Arthritis. J Clin Med 8(7): 938.
-
Kumar A, Verma AK, Kant S, Prakash V, Srivastava A, et al. (2017) A study on Beijing genotype in the clinical isolates of pulmonary drug-resistant tuberculosis. Lung India [Internet] 34(5): 430-433.
-
Raj A, Baliga S, Shenoy MS, Dhanashree B, Mithra PP, et al. (2020) Validity of a CB-NAAT assay in diagnosing tuberculosis in comparison to culture: A study from an urban area of South India. J Clin Tuberc Other Mycobact Dis 21: 100198.
- Are the Vaccines the Only Solution to Prevent the COVID-19 Pandemic? Part Two
- Clinical Characteristics of Women in this New Global Immunodeficiency
- Cell Dynamics in HIV Pathogenesis: Insights and Implications
- Determination of the CDR (CDR1, CDR2) « Complementary- Determining Region Invertebrate Primitive Antibody from Sea Star »
- Prioritizing Care for High-Risk COVID-19 Patients in the EU: 10 Civic Recommendations to the Institutions
- Comprehensive Insights into ModRNA Vaccines: Persistent PP-Spike Recombinant Protein, Hyperimmune/Inflammatory Reactions, Thrombotic Vasculopathy, Chronic Organ Complications and Excess Deaths