Application of Complexity and Variability in Physical Therapy: A Mini-Review
The Generalized Motor Program and Dynamical Systems Theories describe different perspectives of variability for developing movements. In this brief review complexity and variability will be introduced. Linear and nonlinear approaches and application of nonlinearity in practice and physical therapy will then be described. Finally, some points are concluded regarding movement variability and clinical applications.
Systems and complexity
System is any object studied in some fields and might be simple or complex. A simple system is one that has a single pathway to a single answer. In contrast, a complex system such as human movement system is a system composed of many components which may interact with each other. The overall system is complex for the reason that the analysis of the system is inaccurate if assessed part by part [1]. For the movement system for example, movements that occur at one instant may affect and/or affected by movements occur either before or after this movement at that instant. It should be noted that disease leads to a loss of complexity. For example, in a research conducted by Moraiti and coworkers [2] complexity was measured in a group of patients with anterior cruciate ligament (ACL) deficiency. Results showed that ACL deficient patients exhibited more rigid and predictable walking patterns compared to healthy people. This shows a decrease in system complexity.
Variability
Variability is one of the most important features of a complex system. Human movement variability comprises normal variations that occur across multiple reiterations of a task [3, 4]. For example, if we try to repeat the same movement twice, the two movements will never be similar. Consider when you walk over sand or snow, your footprints never repeat exactly. This points out to variability from step to step. It is claimed that variability is inherent in any biological system. Because variability ensures survival. Variability permits selections among options and choice of strategies, and flexibility to adjust to variations in the environment [5]. But how much variability is required for movements? If we consider a spectrum, the extremes of variability would be pathologic. This means that the absence of variability in movement leads to abnormal mapping of sensory cortex, which subsequently disturbs motor function. On the other hand, too much variability also can be a problem, such as in individuals with ataxic movement disorder. Therefore, optimal movement variability stands between excessive variability and reduced variability [6, 7].
There are two contrasting points of view regarding variability and complexity; they are linear or reductionist and nonlinear and complexity-oriented approaches. Linear approach is appropriate for usage with single-system problems, such as an acute infection. However, a condition such as diabetes influences many systems that interact with each other. As a matter of fact, very few problems are really single-system because each system interacts with others for optimal function. Many clinical problems observed in physical therapy settings need a nonlinear approach [1, 8, 9].
Complexity and physical therapy
In the field of physical therapy, variability describes behavioral storage possible for a specific function [6]. As an example, assume two physiotherapists want to examine a patient with stroke. One therapist uses a linear approach and the other applies a nonlinear approach. Generally, the therapist who uses a linear approach assumes that reducing variability of movement would be equal to improving function. Therefore, this therapist assumes a correct movement pattern. Also, this therapist decline feedback gradually and provides less guidance. In contrast, the therapist who uses a nonlinear method assumes that general principle is to develop complexity of movement in order to improve function. This includes concept of dynamic equilibrium or disequilibrium. This means that the movement system never completely become stable and fixed. A healthy movement system works with continuous fluctuations. This allows adaptation to any change in the environment. However, the therapist does not offer guidance. Because the patient doesn’t make identical errors but displays a variety of strategies. So, variability is encouraged if the patient search for information independently. Therefore, flexibility would be increased in terms of availability of options [6, 7].
What are differences between these two approaches?
The basic difference is that for the linear approach, therapist attempts to decrease variability of responses and come to a state of whole equilibrium, but for the nonlinear approach, therapist attempts to increase complexity by encouraging small disequilibrium. In the nonlinear approach, therapist shapes complexity into the task using multiple systems such as cognitive, social, motor, and sensory systems. The practice space is also varied and expanded. In addition, the task progress in a manner that the movement components within the task are linked to each other. In the linear approach, each subtask is independent and disconnected from the other parts of the task due to the interruption of the therapist’s instructions. The therapist using the linear approach prevents response flexibility by asking the patient to avoid errors [6, 7]. The difference between these two approaches is shown in (Figure 1).
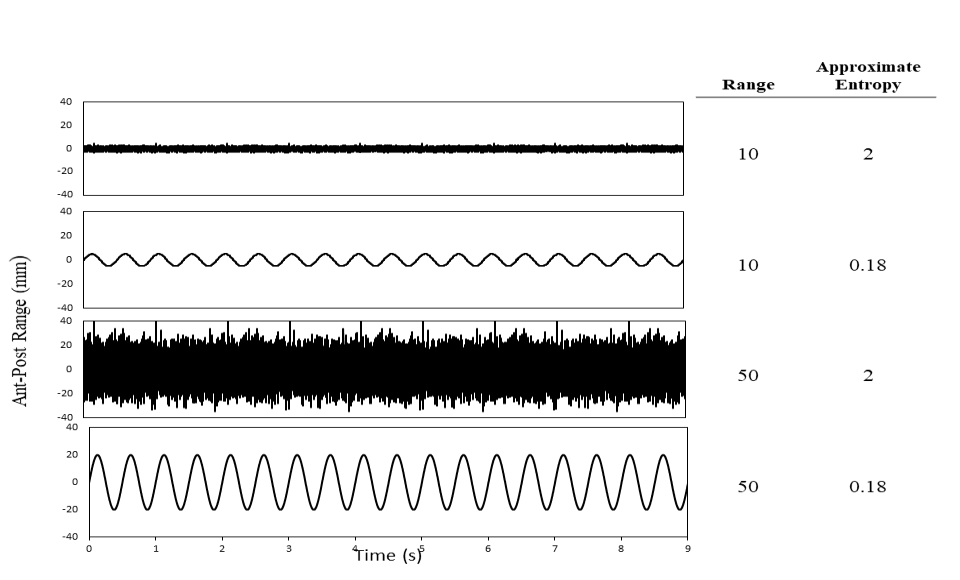
In the right side of the signals, the values of the range or standard deviation as a linear measure and approximate entropy as a nonlinear measure are shown. The last row of the signals shows a high variability in the range but low values of approximate entropy. In the linear approach the goal is to decrease variability. Therefore, the therapist should work toward the signal similar to the second row of the signals. But, if the goal was to enhance the structure of the variability, the therapist should work in a nonlinear method similar to the signal of the third row. As it is observed, considering variability from these different approaches may lead toward opposing types of intervention.
Now let to assume another example. Consider principles of nonlinearity being used for managing movement problems of individuals with Parkinson disease. A well-known program, the BIG training, is considered here. This program emphases on a single attentional parameter which is attention to high- amplitude movements. Principles of management in this approach consist of high intensity, numerous repetitions and complexity. This would result in neuroplasticity and improvement in function. The BIG approach uses complexity because amplitude can enhance adaptability and responsiveness. This approach contains many principles of nonlinearity. In the first place, the overall variability of movement is augmented due to the increase in amplitude. The person with PD previously had been limited to only small movements. But they can now perform large movements and small movements, and all the movement increments in between. Another principle is that a modification in just one movement parameter, that is amplitude, led to a modification in other movement parameters. Another principle is that, the emphasis on executing a “bigger” movement, recalibrates the perceptual system to differentiate between a big versus a small movement. Finally, in this approach, therapist doesn’t teach a specific movement strategy, instead let the individual discover the higher complexity of various movements [6, 10].
Consider another example; The Tscharnuter Akademie for Movement Organization (TAMO) is an intervention that offers a rich perceptual environment. In this approach, the child discovers strategies for execution of a movement using active exploration. The TAMO has several principles; at first, movements are child initiated; because the task has value for child; in addition, the goal is to help the child bring together information about opportunities for movement and adjust to any slight changes; another principle is that errors are anticipated and permitted for learning to occur; finally, increasing variability of movement is favorable and encouraged. Therefore, this approach uses the principles of nonlinearity [11].
Conclusion
There is an optimal amount of variability in the movement system that is associated with health. Therefore, the goal of physical therapy should be to foster the development of this optimal amount of movement variability. Physiotherapists can use principles of nonlinear along with linear methods both for evaluation and therapy. Therefore, it seems that the nature of impairments in the neuromuscular system is less important than the control mechanisms which are adopted by patients for coordinating existing degrees of freedom.
References
-
Rickles D, Hawe P, Shiell A (2007) A simple guide to chaos and complexity. J Epidemiol Community Health 61(11): 933-937.
-
Moraiti C, Stergiou N, Ristanis S, Georgoulis AD (2007) ACL deficiency affects stride-to-stride variability as measured using nonlinear methodology. Knee Surg Sports Traumatol Arthrosc 15(12): 1406-1413.
-
Stergiou N, Decker LM (2011) Human movement variability, nonlinear dynamics, and pathology: Is there a connection? Hum Mov Sci 30(5): 869-888.
-
van Emmerik REA, Ducharme Avelino SWC (2016) Amado, Joseph Hamill. Comparing dynamical systems concepts and techniques for biomechanical analysis. Journal of Sport and Health Science 5(1): 3-13.
-
Stergiou N, Yu Y, Kyvelidou A (2013) A Perspective on Human Movement Variability with Applications in Infancy Motor Development. Kinesiology Review 2(1): 93-102.
-
Harbourne RT, Stergiou N (2009) Perspective on movement variability and the use of nonlinear tools: Principles to guide physical therapy practice. Physical therapy 89(3): 1-15.
-
Stergiou N, Harbourne RT, Cavanaugh JT (2006) Optimal movement variability: A new theoretical perspective for neurologic physical therapy. J Neurol Phys Ther 30(3): 120-129.
-
Cavanaugh JT, Guskiewicz KM, Stergiou N (2005) A nonlinear dynamic approach for evaluating postural control: new directions for the management of sport- related cerebral concussion. Sports Med 35(11): 935- 950.
-
Feldman (2012) Chaos and Fractals, An Elementary Introduction. In: David P (Eds.), 1st (Edn.). https://oxford.universitypressscholarship.com/ view/10.1093/acprof:oso/9780199566433.001.0001/ acprof-9780199566433
-
Farley BG, Koshland GF (2005) Training BIG to move faster: the application of the speed–amplitude relation as a rehabilitation strategy for people with Parkinson’s disease. Exp Brain Res 167(3): 462-467.
-
Tscharnuter I (1993) A New Therapy Approach to Movement Organization. Physical & Occupational Therapy In Pediatrics 13(2): 19-40.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial