Non-Pharmacological Pain Self-Management in an Inpatient Rehabilitation Setting: An Exploratory Quality Improvement Study
Background: Pain neuroscience education (PNE) is well-studied and described in outpatient clinical settings but not inpatient clinical environments. Objective: To assess if PNE nursing education in an inpatient rehabilitation setting would yield positives shifts in patient choices for non-pharmacological treatment choices for pain and increase self-efficacy and self-management of pain. Design: Quality improvement study Methods: Nursing staff at an inpatient rehabilitation facility underwent training in PNE, non-pharmacological approaches to pain and emotional/spiritual support, guided imagery/relaxation techniques and therapeutic presence/touch. Prior to implementation of the training, and following training, a convenience sample of 25 patients (50 total) charts were reviewed to determine if patients received a Pain Control and Comfort menu showcasing various non-pharmacological and selfmanagement strategies for their pain. Additionally, patients’ beliefs and self-efficacy was measured at the time of admission and discharge to determine if exposure to trained nurses altered their self-efficacy during the course of inpatient care. Results: Following training there was a 50.2% increase in non-pharmacological choices to manage pain and specific to the nursing education, there was a 347% increase in utilization of emotional/spiritual support, guided imagery/relaxation techniques, and therapeutic presence/touch to self-manage pain. For pain self-efficacy for dressing, bathing and ability to go to the bathroom, during the pre-improvement period, the mean score at admission for these tasks was at 7.27 and at discharge 9.16, showcasing a 26% positive shift. In the post-improvement period, the mean at-admission score for the 3 functional tasks was 5.69 points but at discharge increased to 9.11 points (61% increase). Conclusion: PNE training to nurses in an inpatient rehabilitation setting yield various positive changes including increased exposure to and use of a pain menu designed to foster increased use of non-pharmacological treatments for pain and foster increased self-efficacy and self-management by the patients.
Introduction
Multiple regulatory bodies for hospital-based health systems have instituted stricter standards for reduction in opioid utilization and require promotion of non- pharmacological approaches to pain, including focusing more on patients’ functional goals [1, 2]. A review of current nursing guidelines for pain management reveals that many of the pain models, and treatment, may be ouzdated and based on biomedical models which only ties tissue health to pain, which is not in line with modern pain science [3, 4, 5]. Furthermore, multimodal pharmacological versus non- pharmacological pain treatment methods are being re- enforced, with a lack of non-pharmacological knowledge by nurses [6, 7]. This stands in stark contrast to a myriad of best- practice guidelines that promote treating pain utilizing the tenants of the biopsychosocial model, as well as multi-modal analgesia including physical, cognitive, psychological, and other mind-body pain treatment interventions [8, 9]. Some large healthcare systems have employed a “pain control and comfort menu” to promote the increased awareness and utilization of non-pharmacological pain treatment methods by nursing for pain management but lack following a true bio psychosocial model [10, 11].
An emerging biopsychosocial approach to pain, based on modern pain science, is pain neuroscience education (PNE) [12]. PNE aim to teach patients more about the underlying biology and physiology of their pain experience including sensitization of the peripheral and central nervous system, inhibition and facilitation, the brain’s role in a pain experience and also strategies to help calm the nervous system, easing pain and improving function [13, 14, 15]. Current best-evidence supports PNE as a non-pharmacological, evidence-based approach to pain, including reduction in self-reported pain, disability, fear-avoidance, pain catastrophizing, physical movement and healthcare cost [16, 17, 18]. Additionally, it is now believed that PNE plus (PNE+) additional evidence- based, self-help techniques such as mindfulness, breathing, relaxation, pacing, sleep hygiene, etc., forms part of a powerful intervention patients should be taught to help manage their pain, with less reliance on a pharmaceutical- only approach [17, 18, 19, 20]. Important to note is that PNE was originally designed by and utilized by physical therapists, but now span many different healthcare providers including physicians, nurses, occupational therapists, psychologists and more [12, 21] thus priming it for its expansion into acute care, inpatient rehabilitation, etc.
This biopsychosocial, non-pharmacological approach to pain is seen in recent shifts by healthcare systems to include “pain menus” including use of the Clinically Aligned Pain Assessment (CAPA) tool for functional pain assessment [22, 23]. Prior settings for the “pain control and comfort menu” were only acute care hospitals, versus inpatient rehabilitation settings [24]. The primary aim of this quality improvement project was to provide nurses education in PNE and PNE+ as a means to promote non-pharmacological treatments for pain in an inpatient rehabilitation setting, thus fostering a safer approach to pain management and promoting self-management [25]. Secondary aims included increased presentation of the “pain control and comfort menu” to patients as well as potential increased self-efficacy related to pain and function.
Methods
Initial Program
In September of 2018, a pain committee of an inpatient rehabilitation hospital attached to a larger non-profit health system was formed to implement a “pain control and comfort menu” in response to the need to fulfill regulatory body guidelines to promote non-pharmacological pain management for patients. (Table 1) showcases the menu used for non-pharmacological pain interventions. Addendum 1 showcases an example of the actual menu.
| Ice pack/IceMan™ machine | Heat (K-Pad™ Machine) |
| Warm blankets | Patient repositioning |
| Relaxing music/imagery on TV channel 125 | Aroma tablets or personal essential oils (no diffusers) |
| Comfortable sleeping position | Mindfulness/meditation |
| Exercises in the room (i.e., ambulation) | Deep breathing/relaxation techniques |
| Leisure (puzzles, games, books, etc.) |
Table 1: Pain Control and Comfort Menu.
These menus were placed as a paper copy, intended for patients to mark off choices, in their personal home education binders, as well as a laminated copy in each room for nursing and therapy staff to refer patients to. This non-pharmacological training became required for all new hire nursing staff (registered nurses and certified nursing assistants) during their initial orientation, to complement and expand upon the menu, and this has continued for every new orientation cycle. Nursing training focused on current bio psychosocial and pain science concepts, well- described in the literature, including sensitization of the nervous system, endogenous mechanisms associated with pain, fear-avoidance, sympathetic stress responses and pain, etc. [12, 14, 15, 16, 26, 27]. The training was supplemented with education on the non-pharmacological pain menu with emphasis on promoting patient pain self-management and self-efficacy. In June 2019, an initial internal assessment of nursing utilization of this program, as well as anonymous surveys completed by nursing staff, revealed inconsistent use of the menu and non-pharmacological pain interventions (Figure 1). However, per formal survey, nursing interest in providing non-pharmacological pain interventions remained high. It was determined at that time to initiate a formal quality improvement project to address these inconsistencies, and support nursing staff in providing non-pharmacological pain interventions.
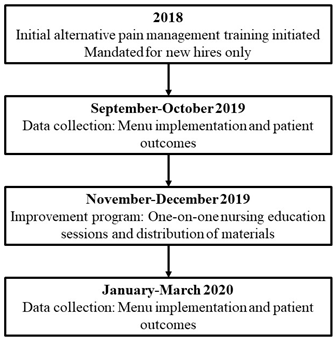
Formal Implementation
Prior to formal implementation of the project, the project was officially reviewed by the affiliated health system’s Institutional Review Board (IRB) and was determined to qualify as a performance improvement project and did not meet criteria for human-subjects research. The pre- improvement period was determined to start mid-September 2019 with a convenience sample of patients admitted to both the inpatient rehabilitation unit and sub-acute rehabilitation unit of an urban 36-bed inpatient rehabilitation hospital that is part of a larger health system. To collect patient data, patients were contacted prior to pain intervention from nursing staff on their day of admission. Patients provided consent to complete questionnaires and patients were informed the questionnaires were part of a pain management improvement project. Ultimately, 25 patients were able to complete both pre- and post- questionnaires, collected by the discharge of the twenty-fifth patient. Discharge questionnaires were completed within 24 hours of pending discharge.
The period of November 2019 through late January 2020 was then designated as the “improvement period”, with two primary objectives established - to increase the number of nursing staff to have completed the alternative pain management training, and to provide an opportunity for nursing staff to learn how to implement diaphragmatic breathing and guided imagery with patients as a non- pharmacological pain intervention [28, 29]. Current nursing staff rosters were consulted to determine which nursing staff, per their hire date, had already gone through the training that was initiated in November 2018. In November 2019, 9 registered nurses and 14 certified nursing assistants had not yet completed the training and per administration’s direction, the nursing staff members who had not yet received training were offered voluntary individual training sessions. Additionally, all nursing staff was offered the opportunity to participate in a one-on-one diaphragmatic breathing and guided imagery training session. Five staff members elected to receive the training, bringing the percentage of nursing staff trained up to 68%. Of the 62 total nursing staff members contacted regarding the additional opportunity to explore it, 9 (8 registered nurses and 1 nurse assistant) scheduled time to be trained in diaphragmatic breathing and guided imagery by late January 2020. To increase carryover of the material learned via the “Alternative Pain Management” training, supplemental documents were provided to all nursing staff related to approved guided imagery, deep breathing, mindfulness, body scan, progressive muscle relaxation and PNE patient education handouts). E-mails were sent to all nursing staff on how to access these handouts and print them for use with patients. Additional training material copies were also placed in nursing break rooms for increased visibility and carryover of training.
The established sample size of 25 patients during the pre-improvement period was then replicated via the same methods in the post-improvement period, again via convenience sampling to obtain 25 additional patients, starting late January 2020. During late March to Early May 2020, chart reviews were completed of the electronic medical record of all fifty patients, noting the number of times pain was recorded, the number of times non-pharmacological intervention-only was utilized (with or without scheduled medications, indicating a choice) and non-pharmacological pain interventions with as-needed pain medications. The only identifiers used to complete a retrospective chart review were the admission to discharge date ranges and room number for each of the fifty patients, however this information was DE identified and ultimately individual pain occurrences and non-pharmacological pain interventions were utilized as totals across all fifty patients to create averages and percentages of total information collected. A similar process was used for deidentifying and totaling the questionnaire responses.
Measures
In order the answer the primary and secondary research questions, various measures were taken: • Number and choice of non-pharmacological treatments: Patient charts were reviewed to extract information on the total number of times patients opted for a non-pharmacological treatment for their pain, including the specific choices. These choices were recorded at the time of admission and discharge to allow for comparison of the choices over the course of the inpatient stay.
• Patient self-reported confidence in pain self- management and use of non-pharmacological pain interventions: Patient confidence in pain self- management and use of non-pharmacological pain interventions were measured using a Likert Point Scale anchored between 1 (not confident) and 10 (confident):
o “How confident do you feel in understanding and managing your pain?” o How confident are you in being able to treat your pain in ways other than pain medications?” • Patient pain self-efficacy: Patient pain self-efficacy (engaging in functional activities despite having pain) was measured using a Likert Scale anchored between 1 (completely limits) and 10 (does not limit):
o How much does your pain limit your ability to dress yourself?” o How much does your pain limit your ability to bathe yourself?” o How much does your pain limit your ability to get to the bathroom?
• CAPA tool: To adopt in part the methodology established by Moore et al. (2019) [10], the CAPA tool was used to track changes in overall pain management and pain related factors from admission to discharge. The CAPA tool contains questions regarding comfort, change in pain, pain control, functioning, and sleep, to improve upon subjective pain assessment from simply using the Numeric Pain Rating Scale (NPRS) [11, 22]. Confidence in pain management, use of non-pharmacological pain interventions, and pain self-efficacy was measured via Likert Scale questionnaire. An additional “yes” or “no” question of “Have you been shown the pain control and comfort menu”? was also asked.
Analysis
Descriptive statistics of means, standard deviations, ranges, and percentages were reported for the various non- pharmacological treatments.
Results
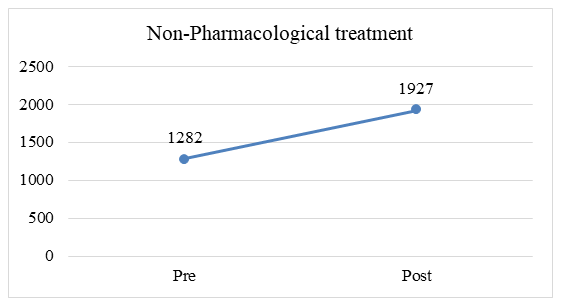
In the two cohorts of 25 patients, prior to (pre) and following (post) training, there was a substantial increase in non-pharmacological choices to manage pain (50.2%) (Figure 2).
Choices
Figure 3 showcases the most frequently chosen non- pharmacological choices by patients prior to and following nurse training in pain science (Figure 3).
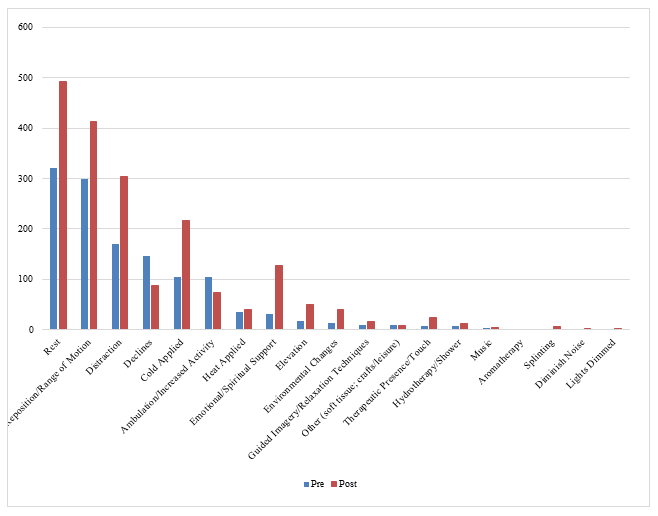
A secondary objective of the project was to increase the utilization of emotional/spiritual support, guided imagery/ relaxation techniques, and therapeutic presence/touch. Combined, in the pre-training period 48 choices related to these 3 approaches were made by patients in pain. In the post-training period, the combined total increased to 167 choices that include these three approaches (347% increase).
Frequency of Use of the “Pain Control & Comfort Menu”
Figure 4 showcases how many patients reported being shown the pain control and comfort menu at admission and discharge. Post-training, 20% more patients were introduced and shown the pain control and comfort menu upon discharge than prior to training (Figure 4).
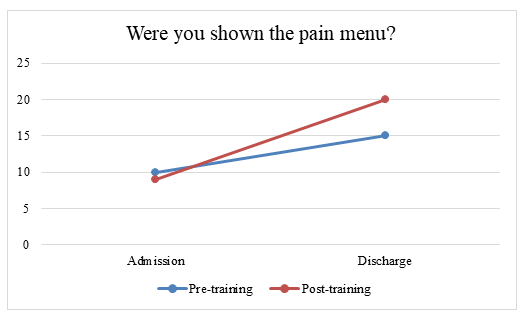
Figure 4: Patient reports of being shown the pain control and comfort menu prior to and following training Patient Reported Confidence in Pain Management and Self-Efficacy with Functional Tasks Prior to and following training, patients reported increased confidence in pain self-management and use of non-pharmacological pain interventions (Figure 5).
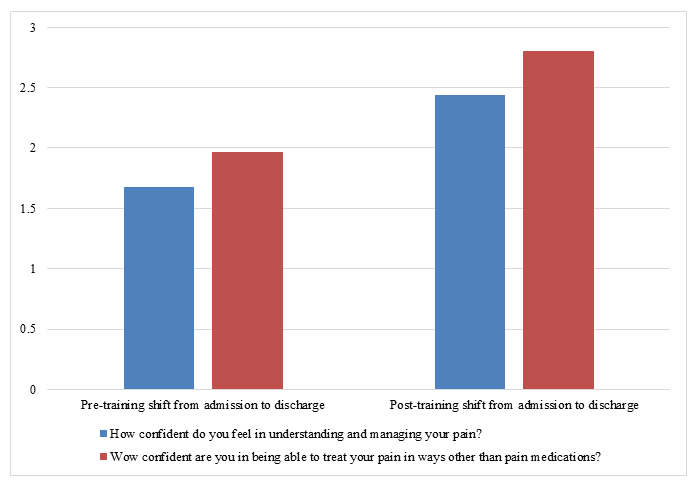
For pain self-efficacy for dressing, bathing and ability to go to the bathroom, during the pre-improvement period, the mean score at admission for these tasks was at 7.27 and at discharge 9.16, showcasing a 26% positive shift. In the post- improvement period, the mean at-admission score for the 3 functional tasks was 5.69 points but at discharge increased to 9.11 points (61% increase).
Discussion
To our knowledge, this is the first study examining the effect of training nursing staff in PNE in an inpatient rehabilitation setting. Results show that PNE training to nurses in this setting yield various positive changes including increased exposure to and use of a pain menu designed to foster increased use of non-pharmacological treatments for pain and foster increased self-efficacy and self-management by the patients.
The ultimate goal of education for healthcare providers is to impact clinical care and improve patient outcomes. To date, it has been proposed that education for healthcare providers (continuing education/continuing medical education) has limited efficacy on altering clinical behavior [30, 31, 32, 33, 34]. In regards to pain, and specifically PNE, there seem to be some potential positive clinical shifts, be it self- reported changes in clinical behavior [12] or direct measures of impact on patient treatments [35]. In this study, teaching nursing staff about PNE and PNE concepts aligning with non-pharmacological and a bio psychosocial approach led to meaningful changes in patient choices and experiences. Following the education, there was a 20% increase in patient exposure to the pain menu and a resultant increase of 50% more choices by patients. This finding is important, in lieu of the current pain and opioid epidemic. It has been shown that early medical exposure to opioids is often the entry point into opioid addiction and all healthcare providers need to educate patient and promote non-pharmacological choices [36]. This is in line with current nursing guidelines in lieu of the opioid epidemic driving increased responsibility for safe and effective pain management [37]. These results concur with various PNE-focused educational initiatives to various healthcare providers. For example, Louw, et. al showed that physician assistant students being taught PNE shift from predominantly pharmaceutical options for pain, including opioids, towards less pharmacological choices for pain [38]. Even though the perspective of the nursing staff themselves were not part of this study, the results suggest the education impact patient experiences. This concurs with a large-scale study, entailing various healthcare providers, taught PNE and at 1-year follow-up 68.3% reported changing their treatment choices based on the educational session [12]. The results from this study thus adds to a growing body of evidence that educating healthcare providers with PNE indeed may trickle down and impact patient care for the better.
This study is the first, to our knowledge, specifically and only assessing PNE education for nurses, and in an inpatient rehabilitation setting. To date, the majority of PNE educational studies have been conducted for physical therapists [16, 39, 40]. Some PNE educational studies has specifically targeted physician assistants [21, 38], but also multidisciplinary audiences [12, 39]. This study, however, specifically targeted nurses, who play a significant role in patient education, especially in acute, surgical and rehabilitation settings. In these roles they significantly impact patient choices when it comes to pain management and self-management of pain [41, 42]. The clinical setting in this study is also new and novel. To date, most PNE research, driven by physical therapy, has focused on outpatient care, be it private practice or hospital-based outpatient clinics [12, 16, 35]. Very little is known or studied about the use of and clinical value of PNE in other clinical settings, especially inpatient environments, be it acute care, rehabilitation, skilled nursing or others. In these controlled medical environments, patients often receive very structured, formal schedules for the delivery of their pharmaceuticals for pain, as opposed to outpatient practice [37, 43]. These results plus various studies showing the benefits of preoperative PNE indicate PNE may have significant benefits for patients in different hospital-based settings, be it acute care, rehabilitation, emergency medicine, perioperative or more [43, 44].
The results from this study show that education of nursing staff alter clinical behavior, which in turn alter patient choices, i.e., non-pharmacological choices to manage pain. Furthermore, the results also show that the nursing education led to changes in patient beliefs including self- efficacy and a push towards functional goals and focus. Self-efficacy has been shown to powerfully impact pain and disability, thus underscoring the relevance of the positive shift in this study [25, 45]. Additionally, a recent update of the fear-avoidance model has shown that patients who focus more on function and is goal-oriented do better than those who focus primarily on their pain [26]. The various positive self-efficacy shifts related to functional tasks of dressing, bathing and ability to go to the bathroom indicate an important clinical effect of educating nursing staff as a means to foster positive affect, optimism and recovery [26].
This study has various limitations. First, this was designed as a quality-improvement study and thus yield limitations in it’s design and data collection, thus not allowing for in-depth statistical analysis, versus trends. Second, it would have been valuable for the study to provide additional information describing the patient population to develop a true sense of the patients being impacted by the nursing educations. Additionally, it would have been helpful to do some qualitative or mixed-method study of the nursing staff themselves and their perspectives of the PNE education or even their perceived expectation of potential clinical impact, versus the actual impact reported in this study. Lastly, the true impact of these interventions cannot be determined by this study – long-term outcome, use of medication including opioids, etc., would be valuable for future studies.
Conclusion
PNE training to nurses in an inpatient rehabilitation setting yield various positive changes including increased exposure to and use of a pain menu designed to foster increased use of non-pharmacological treatments for pain and foster increased self-efficacy and self-management by the patients.
References
-
Busse JW, Wang L, Kamaleldin M, Craigie S, Riva JJ, et al. (2018) Opioids for Chronic Noncancer Pain: A Systematic Review and Meta-analysis. JAMA 320(23): 2448-2460.
-
Weeks J (2015) “Never Only Opioids” and the Joint Commission: toward a Conservative, Whole-system treatment standard for pain. Glob Adv Health Med 4(1): 8-10.
-
Cooney MF, Czarnecki M, Dunwoody C, Eksterowicz N, Merkel S, et al. (2013) American Society for Pain Management Nursing position statement with clinical practice guidelines: authorized agent controlled analgesia. Pain Manag Nurs 14(3): 176-181.
-
Moseley GL (2007) Reconceptualising pain acording to modern pain sciences. Physical Therapy Reviews 12(3): 169-178.
-
Nijs J, Roussel N, Wilgen CP, Koke A, Smeets R (2013) Thinking beyond muscles and joints: therapists’ and patients’ attitudes and beliefs regarding chronic musculoskeletal pain are key to applying effective treatment. Man Ther 18(2): 96-102.
-
Brant JM, Mohr C, Coombs NC, Finn S, Wilmarth E (2017) Nurses’ Knowledge and Attitudes about Pain: Personal and Professional Characteristics and Patient Reported Pain Satisfaction. Pain Manag Nurs 18(4): 214-223.
-
Goode VM, Morgan B, Muckler VC, Cary MP, Zdeb CE, et al. (2019) Multimodal Pain Management for Major Joint Replacement Surgery. Orthop Nurs 38(2): 150-156.
-
Booth J, Moseley GL, Schiltenwolf M, Cashin A,Davies M, et al. (2017) Exercise for chronic musculoskeletal pain: A biopsychosocial approach. Musculoskeletal Care 15(4): 413-421.
-
Jull G (2017) Biopsychosocial model of disease: 40 years on. Which way is the pendulum swinging? Br J Sports Med 51(16): 1187-1188.
-
Moore M, Schuler M, Wilson S, Whisenhunt M, Adams A, et al. (2019) More than pills: alternative adjunct therapies to improve comfort in hospitalised patients. BMJ Open Qual 8(2): e000506.
-
van Boekel RLM, Vissers KCP, Sande RVD, Bronkhorst E, Lerou JGC, et al. (2017) Moving beyond pain scores: Multidimensional pain assessment is essential for adequate pain management after surgery. PLoS One 12(5): e0177345.
-
Louw A, Vogsland R, Marth L, Marshall P, Cox T, et al. (2019) Interdisciplinary Pain Neuroscience Continuing Education in the Veteran’s Affairs: Live Training and Live-Stream with 1-year Follow-up. Clin J Pain 35(11): 901-907.
-
Romm MJ, Ahn S, Fiebert I, Cahalin LP, et al. (2021) A Meta-Analysis of Therapeutic Pain Neuroscience Education, Using Dosage and Treatment Format as Moderator Variables. Pain Pract 21(3): 366-380.
-
Louw A, Zimney K, OHotto C, Hilton S (2016) The clinical application of teaching people about pain. Physiotherapy Theory and Practice 32(5): 385-395.
-
Moseley GL, Hodges PW, M.K. Nicholas MK (2004) A randomized controlled trial of intensive neurophysiology education in chronic low back pain. Clinical Journal of Pain 20(5): 324-330.
-
Louw A, Kory Zimney, Puentedura EJ, Ina Diener (2016) The Efficacy of Therapeutic Neuroscience Education on Musculoskeletal Pain A Systematic Review of the Literature. Physiotherapy Theory and Practice 32(5): 332-355.
-
Wood L, Hendrick PA (2019) A systematic review and meta-analysis of pain neuroscience education for chronic low back pain: Short-and long-term outcomes of pain and disability. Eur J Pain 23(2): 234-249.
-
Watson JA, Ryan CG, Cooper L, Ellington D, Whittle R, et al. (2019) Pain Neuroscience Education for Adults with Chronic Musculoskeletal Pain: A Mixed-Methods Systematic Review and Meta-Analysis. J Pain 20(10): 1140.e1-1140.e22.
-
Louw, A, Sluka KA, Jo Nijs, Courtney CA, Zimneyet K (2021) Revisiting the Provision of Pain Neuroscience Education: An Adjunct Intervention for Patients but a Primary Focus of Clinician Education. J Orthop Sports Phys Ther 51(2): 57-59.
-
Agarwal V, Louw A, Puentedura EJ (2020) Physician- Delivered Pain Neuroscience Education for Opioid Tapering: A Case Report. Int J Environ Res Public Health 17(9): 3324.
-
Zimney Z, Louw A, Johnson J, Peppers S, Farrell K, et al. (2018) Effects of Pain Science Education on Physician Assistant Students Understanding of Pain and Attitudes and Beliefs about Pain. South Dakota Medical Journal 71(11)): 506-511.
-
Topham D, Drew D (2017) Quality Improvement Project: Replacing the Numeric Rating Scale with a Clinically Aligned Pain Assessment (CAPA) Tool. Pain Manag Nurs 18(6): 363-371.
-
Vitullo M, Holloway D, Tellson A, Nguyen H, Estimon K, et al. (2020) Surgical patients’ and registered nurses’ satisfaction and Perception of Using the Clinically Aligned Pain Assessment (CAPA(c)) Tool for Pain Assessment. J Vasc Nurs 38(3): 118-131.
-
Twining J, Padula C (2019) Pilot Testing the Clinically Aligned Pain Assessment (CAPA) Measure. Pain Manag Nurs 20(5): 462-467.
-
Ndosi M, Johnson D, Young T, Hardware B, Hill J, et al. (2015) Effects of needs-based patient education on self- efficacy and health outcomes in people with rheumatoid arthritis: a multicentre, single blind, randomised controlled trial. Annals of the rheumatic diseases 75(6): 1126-32.
-
Vlaeyen JW, Crombez G, Linton SJ (2016) The fear- avoidance model of pain. Pain 157(8): 1588-1589.
-
Agnati LF, Tiengo M, Ferraguti F, Biagini G, Benfenati F, et al. (1991) Pain analgesia and stress: An integrated view. Clinical Journal of Pain 7(Suppl 1): S23-S37.
-
Forward JB, Greuter NE, Crisall SJ, Lester HF (2015) Effect of Structured Touch and Guided Imagery for Pain and Anxiety in Elective Joint Replacement Patients--A Randomized Controlled Trial: M-TIJRP. Perm J 19(4): 18- 28.
-
Topcu SY, Findik UY (2012) Effect of relaxation exercises on controlling postoperative pain. Pain Manag Nurs 13(1): 7-11.
-
Brennan GP, Fritz JM, Hunter SJ (2006) Impact of continuing education interventions on clinical outcomes of patients with neck pain who received physical therapy. Phys Ther 86(9): 1251-1262.
-
Leahy E, Chipchase L, Calo M, Blackstock FC (2020) Which Learning Activities Enhance Physical Therapist Practice? Part 1: Systematic Review and Meta-analysis of Quantitative Studies. Phys Ther 100(9): 1469-1483.
-
Chipchase LS, Cavaleri R, Jull G (2016) Can a professional development workshop with follow-up alter practitioner behaviour and outcomes for neck pain patients? A randomised controlled trial. Man Ther 25: 87-93.
-
Stevenson K, Lewis M, Hay E (2006) Does physiotherapy management of low back pain change as a result of an evidence-based educational programme? J Eval Clin Pract 12(3): 365-375.
-
Cleland JA, Fritz JM, Brennan GP, Magel J (2009) Does continuing education improve physical therapists’ effectiveness in treating neck pain? A randomized clinical trial. Phys Ther 89(1): 38-47.
-
Louw A, Puentedura EJ, Denninger TR, Lutz AD, Cox T, et al. (2022) The clinical impact of pain neuroscience continuing education on physical therapy outcomes for patients with low back and neck pain. PLoS One 17(4): 0267157.
-
Zheng P, Kao MC, Karayannis NV,Smuck M (2017) Stagnant Physical Therapy Referral Rates Alongside Rising Opioid Prescription Rates in Patients With Low Back Pain in the United States 1997-2010. Spine (Phila Pa 1976) 42(9): 670-674.
-
Jungquist CR, Colwell AQ, Vallerand A, Carlisle HL, Cooney M, et al. (2020) American Society for Pain Management Nursing Guidelines on Monitoring for Opioid-Induced Advancing Sedation and Respiratory Depression: Revisions. Pain Manag Nurs 21(1): 7-25.
-
Louw A, Schmieder A, Peppin E, Farrell K, Zimney K, et al. (2020) Can a pain neuroscience edcuation lecture alter treatment choices fro chronic pain in physician assistant students? Psychological Disorders and Research 3(2): 1-5.
-
Moseley GL (2003) Unravelling the barriers to reconceptualisation of the problem in chronic pain: the actual and perceived ability of patients and health professionals to understand the neurophysiology. J Pain 4(4): 184-189.
-
Cox T, Puentedura E, Louw A (2017) An Abbreviated Therapeutic Neuroscience Education Session Improves Pain Knowledge in First Year Physical Therapy Students But Does Not Change Attitudes or Beliefs Journal of Manual & Manipulative Therapy 25(1): 11-21.
-
Oshodi TO (2007) The impact of preoperative education on postoperative pain. Part 1. Br J Nurs 16(13): 790-797.
-
McDonald S, Hedrick S, Green S (2004) Pre-operative education for hip or knee replacement. Cochrane Database Syst Rev (1): CD003526.
-
Louw A, Puentedura EJ, Reed J, Zimney K, Grimm D, et al. (2019) A controlled clinical trial of preoperative pain neuroscience education for patients about to undergo total knee arthroplasty. Clin Rehabil 33(11):1722-1731.
-
Louw A, Diener I, Landers MR, Puentedura EJ (2014) Preoperative pain neuroscience education for lumbar radiculopathy: a multicenter randomized controlled trial with 1-year follow-up. Spine, 2014. 39(18): 1449-1457.
-
Chester R, Khondoker M, Shepstone L, Lewis JS, Herold CJ, et al. (2019) Self-efficacy and risk of persistent shoulder pain: results of a Classification and Regression Tree (CART) analysis. Br J Sports Med 53(13): 825-834.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial