The Utility of an Occupational Therapy Intervention Using Information and Communication Technology during the COVID-19 Infection: An Intervention Report of a University Student with Autism Spectrum Disorder
A client living with autism spectrum disorder (ASD) went to the university and lived alone for the first time. Given the coronavirus situation, he participated in on-demand classes from his apartment from the beginning of his enrollment, and as a result over time he became unable to sustain a distinction between his academic and personal time. As a consequence, he was no longer able to complete his class assignments and, therefore, asked us for help. We implemented remote occupational therapy (OT) using information and communication technology (ICT). We emphasized teaching instrumental daily activities, daily scheduling, communication, and mental health maintenance. We implemented an OT program that encouraged the client to re-establish his daily rhythms. The program improved the client’s daytime routine and allowed them to work on assignments for on-demand classes at the university. We show that using ICT to work on the study of this case (1) does not depend on physical distance, (2) can work when needed, (3) can work as many times as needed in a day, and (4) can provide continuous support in place of face-to-face contact. These findings suggest that regular remote OT visits may help students living with ASD to continue with their university life.
Introduction
The declaration of a state of emergency due to the coronavirus infection (COVID-19) has placed restrictions on all aspects of daily life. Many universities have responded to this situation by implementing distance learning using information and communication technology (ICT). The advantages and disadvantages of such remote classes have been verified [1, 2, 3]. For example, students see advantages in distance learning, such as “I do not have to get up early to go to school anymore. Learning in your own room allows you to concentrate, and the on-demand format allows you to watch multiple times.” On the other hand, some of the stated disadvantages include the following: “The internet connection is unstable, making it difficult to concentrate. Eyes get tired from looking at the screen all the time. The number of assignments increased from previous years because I could not take exams on campus.” On-demand classes tend to disrupt the lifestyle because of the need for self-management of one’s schedule, so their lives tend to be reversed from day to night [3].
Japan’s Ministry of Education, Culture, Sports, Science, and technology reported that 1, 033 undergraduate and graduate students dropped out of school and 4, 205 students took a leave of absence from school between April and October 2020 due to the increase of the COVID-19 infection rate, with 378 (about 37%) first year undergraduate students dropping out and 759 (about 18%) students taking a leave of absence [4]. Kyushu University reported that 40% of students answered “yes” or “somewhat” to the question “Do you feel lonely or isolated?” This indicated the limitations of distance learning and also the need for support for students’ anxiety, [5] and it has been reported that college students living with an autism spectrum disorder (ASD) are prone to anxiety due to thoughts associated with cognitive distortions [6], but their current status owing to the COVID-19 infection rate is unclear.
The Japanese Telemedicine and Telecare Association defined telemedicine as “the act of using telecommunications technology to contribute to health promotion, medical care, and nursing care,” and advocated the use of telemedicine [7]. In occupational therapy (OT), the term “telehealth denotes the use of ICT to provide health-related services even when the service provider and user are in physically different locations” [8]. Other terms used to describe this service delivery model include “tele-OT” and “tele-rehabilitation” [8]. Remote OT holds promise as a model for improving OT utilization and promoting well-being and recovery [9].
At the 54th Japanese Occupational Therapy Congress & Expo in Niigata, there were presentations on “A case study of remote cognitive behavior therapy for parents with internet addiction’s minors” [10] and “Cognitive orientation to daily occupational performance (CO-OP) based tele-occupational therapy for children with reading and handwriting difficulties,” however, there are relatively few existing reports of occupational therapists (OTR) using ICT for remote OT [11].
The authors provide on-site OT for children (and adults) with developmental disabilities and also for truant children. One of the target young adults was a service user, who entered university through home-visit OT. He entered university during the COVID-19 outbreak and began living alone, in a city about 1, 000 km from his home. The university offered on-demand classes to prevent infection from the beginning of his enrollment. As a result, over time he could no longer make a distinction between his academic and personal time and also could no longer attend classes from his apartment. After moving far from home, he sought assistance from the authors.
Therefore, we decided to provide OT as requested using ICT. This was our trial and not a system in place in Japan. We report the usefulness of this trial OT intervention.
Methods
Participant
Case A (teenage, male), whose parents divorced before his birth, lived with his mother and older brother. At five years old, he was diagnosed with ASD. He started using after-school daycare services when he was nine years old and started OT with our OT center in August of his second year of junior high school. When he started home-visit OT, his doctor’s instructions were to provide him with mental support, help him acquire personal organization and social skills, and improve his interpersonal relationships (including those with his family).
Ethical Considerations
The participant and his mother read and understood the instructions for the study and participated voluntarily. Ethical approval for this study was granted by the Ethics Committee of the Kanon Co. Ltd. (approval date: May 25, 2022; approval number: E-004).
OT Evaluation
From the second year of junior high school to the third year of high school: At the beginning of OT visit, Case A had difficulty organizing his personal affairs, poor interpersonal interaction skills, and issues of self- control. His sensory characteristics were characterized by restlessness and impulsive behavior and thus needs vestibular sensory stimulation. In terms of interpersonal relationships, he lied to his family and then justified his lies, which caused many problems with his older brother and mother. His interactions with a limited number of other people outside his family were superficially normal, and he was able to tolerate disagreeable situations. Additionally, he had low motivation to learn and lived without daily goals, and thus an OTR was involved with the goals of helping him acquire personal management skills and improve his interpersonal relationships (including those with his family) while supporting his mental health.
After two months had passed, Case A said to his OTR partner, “I want to get 100 on the test!” With this goal, the OTR guided his motivation toward academics, and he was able to study the salient subjects in junior high school and high school as well and finally was accepted into the university of his choice. During this period, the OTR supported him in performing the instrumental activities of daily living (IADLs), such as managing submissions, cleaning up his room, setting goals, accomplishing tasks on his own, and planning and accomplishing schedules—tasks that were difficult for him to accomplish. The frequency of support was once a month which continued until he graduated from high school.
The situation before entering the university: On entering university, he lived alone in a 1DK (one bedroom + dining room and kitchen). The university’s regular curriculum and semi-regular activities were delivered on- demand, and extracurricular activities, such as clubs, circles, and independent seminars, were suspended. He was unable to work on class assignments at the university, and his social interactions with friends were limited, so he led a solitary life. As a result, he was unable to work on class assignments and submissions until the due date was approaching but he was able to talk to his mother and OTRs about his problems.
Two weeks after he had begun living alone, the Vineland- II Adaptive Behavior Scale was administered to determine his adaptive behavior and behavioral characteristics. Vineland- II can be converted to standard scores similar to those used in numerous standardized tests, starting from a crude score calculation for each sub-domain. In the “Adaptive Behavior Assessment,” standard scores of M = 100 and SD = 15 were obtained for the domains of “Communication,” “daily living skills,” “Social Skills,” and “Motor Skills.” The “Adaptive Behavior Composite Score” (M = 100, SD = 15) was calculated by integrating these domains. In each sub-area, a standard score (M = 15, SD = 3), called the v-score, was obtained. In the Maladaptive Behavior Assessment, v-scores were obtained for the Internalizing Problem, Externalizing Problem, and the maladaptive behavior index, which was the sum of the three. In the “Maladaptive Behavioral Criteria,” the standard score was not calculated, and the frequency and intensity of the behavior were evaluated with each question item. A higher score in the “Adaptive Behavior Index” indicates a higher level of adaptive behavior, while a higher score in the “maladaptive behavior index” indicates that the subject had more maladaptive elements in their life [12]. The adaptation level of each item was “slightly low” for “housework” (daily living skills) and “interpersonal relationships” (social skills). The corresponding ages were 11 years and 6 months for “housework” and 9 years and 2 months for “interpersonal relationships.” The maladaptive behavior index was “slightly high” for both internalizing and externalizing problems.
Methods and Goals of Intervention
The short-term goals were to establish a sustainable solitary lifestyle, including working on interpersonal relationships and to be able to engage in tasks in a planned manner. Telephone contact was made once a month to check on the living conditions. The long-term goal was to complete remote OT by using Zoom and LINE two to three times a month, according to the subject’s daily rhythm, the severity of ADL, and university study status. His subjective and objective situations were extracted from the progress records, and the subject’s issues and OTR support at that time were summarized. In addition, the Japanese version of the Vineland-II Adaptive Behavior Scale was used to compare the subject’s standard scores on each item at the time of university enrollment and then one year later.
Results
The OT approach beginning from April of the first year of university to April of the second year is divided into five periods (Table 1).
| Month | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 1 | 2 | 3 | 4 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Phase | Ⅰ→ | Ⅱ→ | Ⅲ→ | Ⅳ→ | Ⅴ→ | |||||||||
| Method | Phone | 〇 | □ | □ | 〇 | □ | □ | 〇 | ||||||
| Apartment Visit | 〇 | □ | ||||||||||||
| Home-visit | □◇ | 〇□◇ | ||||||||||||
| ZOOM | □◇ | □◇ | 〇 ◇ | 〇 ◇ | ||||||||||
| LINE | ●● |
Table 1: Progress of Occupational Therapy. Phone indicates telephone contact. Apartment indicates an apartment near the universit
Table 1: Progress of Occupational Therapy. Phone indicates telephone contact. Apartment indicates an apartment near the university where he lives. Home indicates the house he shares with his mother. Zoom indicates an online conferencing system. Line indicates a mobile messaging application. White circles indicate that the OT was being conducted at the beginning of the month, white squares indicate the middle of the month, and white diamonds indicate the end of the month. Black circles indicate that the exchange was conducted every day for a week.
Period I: April to May 2020
When contacted by telephone in early April 2020, a positive statement was acknowledged: “I am getting used to living alone, and I am working hard on my school assignments.” However, he never went to school because the university was closed. Consequently, he had no friends, no opportunities to interact with others, and felt lonely. He was allowed to say, “I have been living a life of staying at home ....” In May, he responded, “I am working on my school assignments and my room is a mess, but I am doing laundry and cleaning,” The OTR encouraged him to continue to clean and do laundry.
Period II: June to September 2020
During the phone call in June, he remarked, “I am working on my school assignments without any problems...,” however, “I have a hard time with the kitchen sink...” and expressed concern about his IADL. The OTR visited Case A’s residence in mid-July to assess the current situation. At that time, the living space was clean, but the dishes and pans in the kitchen area were covered with mold because they had been left unattended for a long time after usage. In addition, three garbage bags were left at the entrance, because he had probably cleaned the apartment just before the visit. He also stated, “I cleaned the room frantically because the OTR was coming but I didn’t know how to do the sink, so please teach me how to clean it.” He asked for assistance, therefore, under the guidance of the OTR, he learned how to clean the sink. Since he was only eating two cups of ramen noodles a day, we discussed ways to improve his diet and instructed him to buy a boxed lunch or a side dish once a day. During this time, Case A was anxious about his new life and tried to avoid bringing gaming devices into his apartment. Consequently, he could obtain 90% of the credits for the courses he took despite his IADL problems.
Period III: October to November 2020
Since the second semester was also an on-demand- oriented class, Case A went home to his mother’s house and stayed there from mid-October to late November. He participated in the class from home. The OTR visited him at his mother’s house once a week to check on his assignments and discuss his situation at the university and his experience of living alone. During this period, he sometimes had to put off his on-demand classes, but with his mother’s encouragement, he was able to complete his university assignments smoothly.
Period IV: December 2020 to March 2021
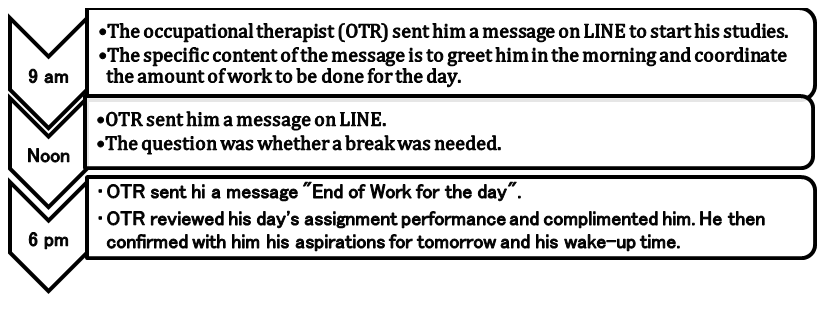
In late November, Case A resumed living alone to prepare for the examinations in the second semester. This time, he brought a video game console from his house, as playing electronic games was one of his hobbies. On-demand classes continued to be offered at the university but he began getting distracted due to the games as he could watch those classes at any time. Gradually, his daily rhythm was getting disrupted, and he seemed to be leading a life in which his days and nights were reversed. When the OTR called him, he responded positively, “My daily rhythm is not stable, but I am managing my tasks.” However, he felt a sense of crisis just before the late December deadline for submitting assignments that were due for the second semester: “I had not listened to 30 on-demand lessons for three subjects, and I was storing up assignments. How should I tackle the assignments?” he asked the OTR. We suggested using Zoom to meet with the OTR once a week, in addition to checking assignment due dates and planning assignment execution schedules. The Zoom interviews consisted of the following five items for about 40 minutes: (1) how he spent this time during the day, (2) talking about university assignments and friends, (3) talking about recent news and hobbies, (4) translating English sentences together, and (5) discussing failure stories with the OTR. In addition, communication with Case A was conducted via LINE. By communicating daily at 9:00, 12:00, and 18:00, we established Case A’s daily rhythm, motivated him to complete his tasks, checked his performance, and conducted positive feedback for two weeks (Figure 1).
Period V: April 2021 (sophomore year)
A new academic year began, and many of the courses taken consisted of face-to-face and hybrid classes. Case A has been attending the university more and more, “I have more friends in the department, and when I study for tests, I use the ICT technology I learned in distance OT to work on my assignments in my room, collaborating with my friends through the screen.” He also said, “I have more friends in the university.” The series of remote OT sessions ended with a few exchanges of LINE messages and phone calls to confirm the course subjects.
Changes in the Japanese version of the Vineland- II Adaptive Behavior Scale
The change in the adaptation level of each item at the time of admission and one year later is shown in Table 2. Household chores in daily living skills and interpersonal relationships in social skills scored as “somewhat low.” The corresponding age was unchanged at 11 years and 6 months for housework and changed from 9 years and 2 months to 12 years and 6 months for interpersonal relationships. The maladaptive behavior index was slightly high for both internalizing and externalizing problems, and there was no significant change between the start of the study and one year later.
Comments from Case a during the final evaluation
The OTR asked, “What was the hardest part of going to university during the COVID-19 infection?” His answer to this question was “Not being able to attend university was the hardest part. I had studied at school since high school because studying at home was too tempting and difficult for me. So, having to study in my own living space was very hard for me.” The OTR asked, “What do you think of this process in retrospect?” His answer to this question was “Looking back at the history of the LINE, I still think it was a critical situation. I am glad that I was able to ask for help from the OTR at that time, and that I was able to achieve my goal of doing it on schedule and meet the OTR’s expectations.”
| Adaptive behavior assessment | ||
|---|---|---|
| Area | At the time of entering university | Current Status |
| Communication | 96 | 96 |
| Daily living skills | 105 | 89 |
| Sociality | 85 | 92 |
Table 2: Changes in the Japanese Vineland-II Adaptive Behavior Scale.
The OTR asked, “How do you feel about the benefits of using ICT?” His answer to this question was “As the assignments piled up, I blamed myself for my inadequacies, and sometimes I wanted to die because I could not sublimate these feelings on my own.” However, he realized the power of ICT, which allowed him to consult with the OTR easily even when he was away from home, and he felt that listening to the OTR’s casual stories of failure helped him mentally and gave him courage. Also, because he had no one to talk to about his true feelings apart from his mother, the time he spent talking with the OTR was a good time to let out his feelings of weakness. He answered, “I am very grateful to the OTR for giving me the opportunity to talk.”
Discussion
The Effectiveness of OT using ICT
Based on the results of the evaluation, the short-term goals were set as “establishing a solitary lifestyle and building interpersonal relationships” and “being able to tackle tasks in a planned manner,” and the long-term goal was set as the “completion of remote OT.” The standardized scores of the Japanese version of the Vineland-II Adaptive Behavior Scale did not change significantly between Case A’s time of enrollment and one year later. In the daily living skills scale, the score increased from 105 before enrollment to 89 now, but the difference was due to an increase in age rather than a rough score. The corresponding age for interpersonal skills increased from 9 years and 2 months to 12 years and 6 months, despite the decrease in opportunities for interaction due to behavioral restrictions. This finding is presumably because Case A asked himself questions and took action through his involvement with the OTR.
Case A continued to live in a 1DK due to behavioral restrictions, resulting in a disruption in the daily rhythm of life. The first step in regulating the daily rhythm of life is to synchronize the body clock with the outside world [13]. Exposure to outdoor light is said to be effective for this [14, 15]. However, the declaration of a state of emergency reduced opportunities to go outside during the daytime, creating a vicious cycle in the daily rhythm of life. One of the characteristics of living with ASD is impaired executive function. Executive function is “the ability to know when, where, what, and how to do things,” and when this is impaired, impulsive behavior and irritable reactions occur [16]. These include “difficulty concentrating in one’s room” and “reduced attention span due to distractions from family, cell phones, and other things outside of class” [17]. Not only students living with ASD, but “many other university students have negative attitudes toward distance learning due to the reduced motivation and drive to use ICT, and they feel that it has a negative impact on their learning experience and motivation to learn” [17]. Case A had planned to study on the university campus after entering the university but was forced to complete his assignments in his room without commuting to school. In addition, he was plagued by loneliness and temptations (games) rather than studying in the enclosed space of his 1DK, and his motivation to study decreased significantly, leading to an accumulation of assignments at the university. These findings suggest that while it is difficult for any university student and adult to maintain motivation for learning, Case A experienced even more difficulty managing his schedule and his inability to manage himself contributed to the worsening of his situation.
An earlier report stated, “people are resisting daily temptations to achieve self-discipline and long-term goals, even though they are tempted daily by temptations that are tempting” [18, 19]. The OTR inferred they were able to help Case A to cope with the conflict and complete the task by setting him a daily schedule, providing task performance goals, and giving him an obligation to report the activity. It was also reported that “many students are anxious and unable to find clues to work on their own initiative” [20]. Case A appreciated the convenience of being able to consult easily with the OTR through the usage of ICT. We can use ICT to keep in touch on a daily basis. In Case A, it was inferred that the OT intervention using ICT improved the students’ motivation and led to their independent efforts. This was also made possible by the fact that the OTR was a person other than his mother to whom he could talk about his true feelings.
These results suggest that remote OT using ICT can be useful as a means of encouraging independent activity and the participation of those subjects living with ASD. In addition, tele-OT can be a means of providing continuous support when regular OTR visits are difficult.
Remote OT in the Future
We have shown that the usage of ICT to work in the study of Case A (1) does not depend on physical distance, (2) can work when needed, (3) can work as many times as needed in a day, and (4) can provide continuous support in place of face- to-face contact. The combination of multiple methods was also found to enable an accurate understanding of the target person and the provision of necessary support. In addition, what we realized in our involvement with Case A was the need for an on-site OT to assess the current situation. In this case, the authors were able to provide both remote OT and on-site OT. This allowed OTR to assess Case A’s living situation and suggest available services. These were important events in the detailed study of Case A’s new life. However, it is not possible to adapt the present measures to all children and adults. Therefore, it is important to collaborate with the home-visit service at the subject’s locality.
In the future, more and more children in remote areas living with ASD whom the authors support will go to high schools and universities. It is easy to assume that even if the children have acquired a stable daily rhythm and social participation, changes in their living environment will make it difficult for them to cope, and they may fall into a chaotic situation. Remote OT is a necessary means to avoid such situations.
The challenges ahead are (1) hardware and software for ICT, (2) expenses for remote OT, and (3) the service system for remote OT.
The information that could not be obtained by telephone was obtained using Zoom and LINE. However, the changing facial expressions of Case A, as well as the situation inside the apartment, were sometimes unclear due to the poor picture resolution of the camera hardware and software of both parties. In addition, the communication technology also affected the results. This point is expected to improve with the initiation of 5G and the accompanying improvement of hardware and software. In addition, knowledge of security measures in the usage of ICT will become increasingly important for OTRs. The cost of remote OT was billed by insurance only for Case A’s apartment and home visits after returning home. However, the transportation costs for the apartment visit and the interview with the help of ICT usage were borne by the individual or office of the OTR. Due to the spread of COVID-19 infection, the Ministry of Health, Labour, and Welfare of Japan has suddenly relaxed the previous requirements and approved telephone and online medical services. We hope that the Japanese Association of Occupational Therapists and other related OT organizations will gather evidence of remote OT and that this evidence will be included in the reimbursement system. In remote OT, one OTR was involved mainly because of the importance of the connection with Case A. However, a need arose to be involved outside of normal working hours, and the company struggled to put in place a system to accommodate this need.
Therefore, to promote remote OT, it is necessary to establish an overall service system, including a primary and a second person in charge, and also implement a day shift and a night shift. It is also necessary to clarify what remote OT can and cannot do and to take measures to compensate for the disadvantages of remote OT. For example, it is necessary to consider collaborating with offices that provide on-site OT in the area and also with the student affairs office of the university concerned.
As mentioned above, many issues need to be addressed to actively introduce remote OT. However, in other countries, its effectiveness and necessity have been verified in a wide variety of ways [21, 22]. The present findings suggest that tele-OT not only supports ADL and IADL, including daily life rhythms, according to the disability characteristics of the target children and adults but also contributes positively to their mental health.
Conclusion
A client living with ASD went to university and started living alone; however, given the coronavirus situation, he took on-demand classes in his apartment from the beginning of his enrollment.
Therefore, we implemented remote OT using ICT. We implemented an OT program that encouraged the client to re-establish his daily rhythms. The program improved the client’s daytime routine and allowed him to work on assignments for on-demand classes at the university.
These findings suggest that regular remote OT may help students living with ASD to continue with their university life.
Conflicts of Interest
The authors declare that they have no conflict of interest.
Acknowledgements
The authors thank the parent of the participant and the staff of Kanon Co. Ltd., for their excellent assistance. Part of this paper was presented at the 55th Japanese Occupational Therapy Conference & Expo in Sendai, Japan.
Funding
Not applicable
References
-
Mishra L, Gupta T, Shree A (2020) Online teaching- learning in higher education during lockdown period of COVID-19 pandemic. Int J Educ Res Open 1: 100012.
-
Sharma A, Alvi I (2021) Evaluating pre and post COVID 19 learning: an empirical study of learners’ perception in higher education. Educ Inf Technol (Dordr) 26(6): 7015-7032.
-
Almendingen K, Morseth MS, Gjølstad E, Brevik A, Tørris C (2021) Student’s experiences with online teaching following COVID-19 lockdown: a mixed methods explorative study. PLOS ONE 16(8): e0250378.
-
Ministry of Education, Culture, Sports, Science and Technology: survey on support for students affected by new strains of coronavirus infection in Japanese.
-
Kyushu University Public Relations Office: Results of the Student Questionnaire on Student Life at Kyushu University (Spring Semester) in Japanese.
-
Ishizawa K, Hosokawa M (2018) A study of the relationship between traits of autism spectrum disorder and anxiety in college students. Bulletin of the Faculty of Education, Ibaraki University. Education Sci 67: 409- 422.
-
(2013) Japanese Telemedicine and Telecare Association: Illustration: Telemedicine in Japan.
-
(2021) Occupational Therapy and Telehealth. World Federation of Occupational Therapists.
-
Hung G, Fong K (2019) Effects of telerehabilitation in occupational therapy practice: a systematic review. Hong Kong J Occup Ther 32(1): 3-21.
-
Horita H, Shimizu E (2020) A case study of remote cognitive behavior therapy for parents with internet addiction’s minors. Japanese Society of Occupational Therapy Abstracts 54: 887.
-
Shiozu H, Okutsu M, Kurasawa S (2021) Cognitive orientation to daily occupational performance (CO- OP)-based tele-occupational therapy for children with reading and handwriting difficulties. Japanese Occupational Therapy Research 40(1): 72-78.
-
Hagiwara T (2016) Japanese Vineland-II adaptive behavior scale overview in Japanese. Japanese Journal of Child and Adolescent Psychiatry 57(1):26-29.
-
Okawa M (1995) Development of sleep-wake rhythm and it’s disorder. Japanese Journal of Clinical Ecology 4: 56-62.
-
Yamanaka Y (2016) Living environment and circadian clock in humans. Japanese Journal of Biometeorology 53(2): 69-81.
-
Hashimoto S, Honma S, Honma K (2007) Sleep and biological rhythms. Folia Pharmacologica Japonica 129(6): 400-403.
-
Takase C, Matsuhisa M, Imamura S (2020) Individual support classes for college students with developmental disabilities: the effect of individual support and self- recording on behavioral improvement for the students with difficulties with schedule management. St. Andrew’s University of Education Bulletin of the Research Institute 2: 27-41.
-
Serhan D (2020) Transitioning from face-to-face to remote learning: students’ attitudes and perceptions of using zoom during COVID-19 pandemic. International Journal of Technology in Education and Science (IJTES) 4(4): 335-345.
-
Fujita K (2011) On conceptualizing self-control as more than the effortful inhibition of impulses. Pers Soc Psychol Rev 15(4): 352-366.
-
Tang L, Toyama M, Miwa S, Nagamine M, Kainuma R, et al. (2021) The effects of temptation coping strategies on self-control in academic contexts: The moderating role of goal importance and difficulty. The Japanese Journal of Psychology 92(3): 204-210.
-
Kida Y, Takagi S (2001) Mental Health and Psycho– Education of students from a viewpoint of Student Counseling. –Based on UPI for the 10 years of Toyama University of International Studies–. Journal of the Faculty of Humanities and Social Sciences, Toyama University of International Studies 1: 155-166.
-
Cason J (2009) A pilot telerehabilitation program: delivering early intervention services to rural families. Int J Telerehabil 1(1): 29-38.
-
Nix J, Comans T (2017) Home quick: occupational therapy home visits using mHealth, to facilitate discharge from acute admission back to the community. Int J Telerehabil 9(1): 47-54.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial