Evaluation of Q Angle in Down syndrome
Background: Down Syndrome is a genetic disorder and the most common chromosomal abnormality. It is predominantly characterized by muscle hypotonia and joint hypermobility. Qangle is the angle formed between two imaginary lines one from ASIS to Center of Patella, another from Tibial tuberosity to the Center of Patella. Objectives: Aim of the study is to evaluate the Q-angle in male children with Down syndrome of 7-16 years of age and compare the values between children with internal and external tibial torsion. Methodology: It is an observational study done with convenient sampling carried out in 12 male children with Down syndrome. The tibial torsion was measured. Based on internal and external tibial torsion they were categorized into Group A and B respectively. Group A consisting of 7 children with internal tibial torsion and Group B consisting of 5 children with external tibial torsion. Q-angle was measured using standard goniometer. Results: There is no significant difference in P-value (P>0.05) between the right and left leg of children in Group A and in Group B. On comparison between Group A and Group B, there was a statistical significance in P-Value of 0.005 and 0.050 when compared mean of Q angle for right leg and left leg respectively. Conclusion: The study concluded that assessing Q-angle helps to evaluate the biomechanical changes in knee. In this study done for the male children with Down syndrome, the Q-angle lies within the normal range of 13.1±3.5. However children with internal tibial torsion has comparatively decreased angle and children with ex
Introduction
Down syndrome is a genetic disorder and the most common chromosomal abnormality. Incidence in India is 1 per 1150 live birth [1]. Cause of Down syndrome can be attributed to the non-disjunction in which there is a failure of the genetic material to separate during the formation. Hence there occurs an alteration in the genetic mechanism resulting in an extra chromosome in chromosome 21. Hence also called as Trisomy 21 [1]. The risk factors for Down syndrome include advanced maternal age, consanguineous marriage, exposure of the parents to chemicals, radiation during pregnancy and socioeconomic factors [2]. Down syndrome individuals are chiefly characterized by muscle hypotonia and joint hypermobility. The other features include flattened face, unusual shaped or small ears, short neck, wide gap between 1st and 2nd toes [3].
Q-angle defines the vector pull by the quadriceps muscle on patella. It is defined as the angle formed between two imaginary lines, one starting from ASIS to CP (center of patella) and another starting from Tibial tuberosity (TT) to CP [4, 5]. It was first defined by Brattstrom [6]. It is an important factor in assessing the function of knee joint [7]. It is the lateral force exerted by the quadriceps muscle activation on the patellofemoral joint [8]. It is usually taken for the evaluation of patellar alignment for the clinical measurements of knee alignment in relation to hip, femur and tibia. The normal range of Q-angle for male children between 7-12 years of age is 13.1±3.5 and for female children is 13.7±4.9. Although Q-angle varies in a wide range in children [5], however when the values exceeds the range, the child is more prone to biomechanical alterations and gait pattern deviation thereby increased risk of injuries. Tibial torsion- the angle between transmalleolar axis and transverse axis of knee. Tibial torsion-internal or external depending upon the inward or outward rotation of tibia respectively. There are previous studies available related to Q-angle in spastic cerebral palsy and in typically normal population but no study has been conducted for the evaluation of Q-angle in Down syndrome. Identifying Q-angle changes can result in disabling individuals by abnormal exertion of quadriceps force on knee joint. Hence the disability potential can be addressed as a risk factor. Hence the aim of the study is evaluation of Q-angle in male children with Down syndrome of 7-16 years of age and comparison of the values between Demographic Variables children with internal and external tibial torsion.
Methodology
It is an observational study done with convenient sampling. Based on the selection criteria 12 children were selected. Inclusion criteria included boys of age group between 7-12 years and those who were able to stand and walk independently. The exclusion criteria included those who had any recent orthopedic surgery at lower extremities, children with congenital deformity of lower limb and those with recent musculoskeletal injuries in lower limb were excluded. The children were categorized into- Group A consisting of 7 children with internal tibial torsion and Group B consisting of 5 children with external tibial torsion. Later standard goniometer was used to measure Q-angle. Q-angle measurement- The child was made to lie in supine position. Two imaginary lines were drawn. One starting from ASIS to CP (Center of patella); another starting from tibial tuberosity to CP. Angle formed by these two line were measured. Measurement of Tibial torsion- The child was made to lie in prone and TFA was measured with the knee in 90 degrees flexion and ankle in neutral position. Angle between two axes were measured. One is the axis of thigh and another is the axis of foot.
Statistical Analysis
The collected data was tabulated and was analyzed using SPSS software
| N | Mean | Sd | T - Value | P - Value | ||
|---|---|---|---|---|---|---|
| Age | Group A | 7 | 11.71 | 3.638 | -2.337 | 0.042 S |
| Age | Group B | 5 | 15.6 | 0.548 | -2.337 | 0.042 S |
| BMI | Group A | 7 | 18.457 | 3.7973 | -2.914 | 0.015 S |
| BMI | Group B | 5 | 25.2 | 4.1713 | -2.914 | 0.015 S |
Table 1: shows that the mean age of group A is 11.71; group B is 15.60 and mean BMI of group A is 18.45; group B is 25.20.
Comparison between Right and Left Leg Q-Angle within the Same Group
| N | Mean | SD | T - Value | P - Value | ||
|---|---|---|---|---|---|---|
| Group A | Right | 7 | 10.43 | 2.637 | -0.624 | 0.544 NS |
| Group A | Left | 7 | 11.29 | 2.498 | -0.624 | 0.544 NS |
| Group B | Right | 5 | 14.8 | 0.447 | 1.372 | 0.207 NS |
| Group B | Left | 5 | 14 | 1.225 | 1.372 | 0.207 NS |
| N | Mean | Std. Deviation | T - Value | P - Value | ||
| Right | Group A | 7 | 10.429 | 2.6367 | -3.621 | 0.005 S |
| Right | Group B | 5 | 14.8 | 0.4472 | -3.621 | 0.005 S |
| Left | Group A | 7 | 11.29 | 2.498 | -2.224 | 0.05 |
| Left | Group B | 5 | 14 | 1.225 | -2.224 | S |
Table 2: shows the comparison between the right and left leg Q-angle within the same group with P>0.05 in both group A and B. Com
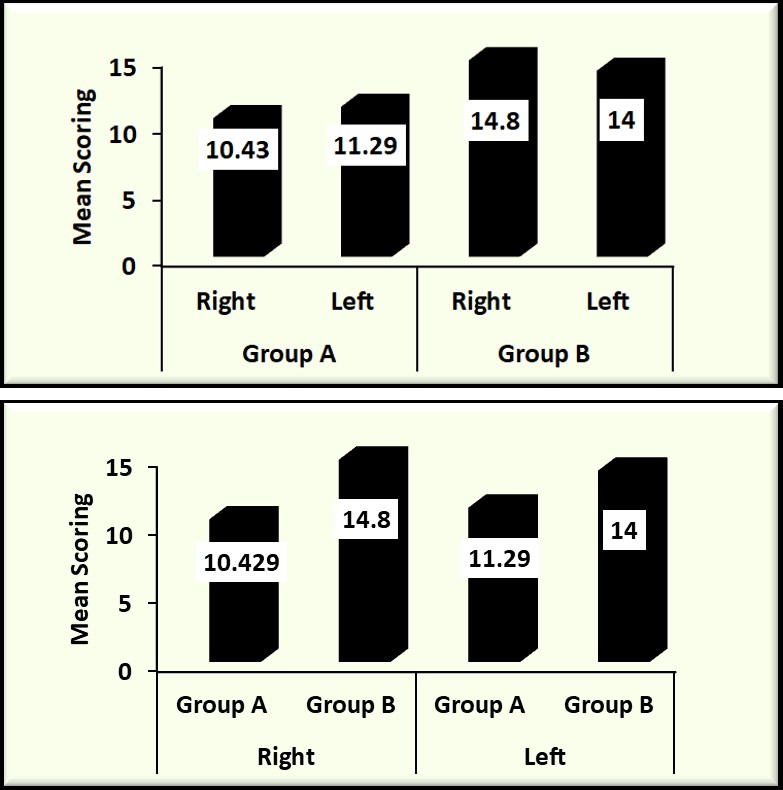
Graph 1: Bar Graph Showing the Comparison between Right and Left Leg Q-Angle within the Same Groups.
Graph 2: Bar Graph Showing a Comparison of the Mean Q-Angle of Each Leg between Group A and B.
Results
Table 1 shows the demographic variables. The mean age of group A is 11.71; group B is 15.60 and mean BMI of group A is 18.45 and group B is 25.20 Table 2 shows the comparison between Q-angle of right and left leg of children within the same group. In Children with internal tibial torsion, mean of Q-angle of right leg- 10.43 and left leg- 11.29. There is no significant difference in P-value (0.544) between right and left leg of children in Group A. In children with external tibial torsion, mean of Q-angle of right leg- 14.80 and left leg- 14.00. Similar to Group A, there is no significant difference in P-value (0.207) between right and left leg of children in Group B.
Table 3 shows a comparison of mean Q-angle of each leg between group A and B. There is statistically a significant difference of P-value 0.005 between the right leg of children with internal tibial torsion- Mean 10.429 and external tibial torsion- Mean 14.800). Also there is a significant statistical difference of P-value 0.050 between the left leg of children with internal torsion- Mean 11.29 and external torsion- Mean 14.00.
Discussion
The purpose of the current study is evaluation of Q-angle in male children with Down syndrome between 7-12 years of age and to compare the values between children with internal and external tibial torsion. Q-angle is an important factor in assessing the biomechanical changes in knee joint thereby contributing to the changes in the alignment of hip, knee and ankle and hence to plan for the treatment protocol in cases of any deviations so as to prevent the further injuries of deformities. The subjects included in the study were above 7 years of age as children below 7 years undergo continuous physiological changes occurring in lower extremity alignment. Also due to limited literature support as not many studies involving Q-angle in paediatric population especially in Down syndrome children is available, the statements in the study can be hypothetical. In the current study, mean values of Q angle between the right and left leg of group with internal torsion did not show any statistical difference (p>0.05). Similarly mean values of Q angle between the right and left leg of group with external torsion did not show any statistical difference (p>0.05). Elizabeth Ardolino et al., (2017) stated that Dynamic walking program helps in strengthening the muscle [9]. While Jehoon Lee et al., (2014) in his study stated that on increasing the dynamic strength by weight bearing there will be a significant effect on Q-angle [10]. Ajlan Sac et al., (2018) stated in his study that, greater Q angle is associated with reduced isokinetic knee strength. Hence we can conclude that, owing to the strengthening exercises received for hypotonia the normal range of Q angle is observed in the participants [11]. Also the children included in the study were able to walk independently. Hence this might be because the participants in the study would have received early weight-bearing interventions and hence deviations from the normal range of Q-angle is noted.
Conclusion
The study concluded that assessing Q-angle helps to evaluate the biomechanical changes in knee. Also the Q-angle of male children with Down syndrome between the age group 7-16 lies within the normal range of 13.1±3.5. However children with internal tibial torsion has comparatively decreased angle and children with external tibial torsion has comparatively increased angle even though there is no deviation from the normal range for the age.
Limitation and Recommendations
Limitations
- The sample size is small
- The study included only male children with Down syndrome
- Children below 7 years were excluded
- Q angle in various positions were not taken into account
- Muscle strength of quadriceps and gait pattern was not assessed
Recommendations
- Future studies can be done in girl children with Down syndrome of the same age group
- Studies involving individuals with no prior interventions can be done
- Studies including muscle strength of quadriceps and gait pattern can be done for further correlation with the Q-angle
- Also studies can be done by assessing any other biomechanical deviations in Down syndrome children.
References
-
Ram lakhan, Madhavaram Thomas Kishore (2016) Down syndrome in tribal population in India: A field observation, Journal of Neurosciences in rural practice 7(1): 40-43.
-
Malini SS, Ramachandra NB (2007) Possible risk factors for Down syndrome and sex chromosomal aneuploidy in Mysore, South India. Indian journal of human genetics 13(3): 102.
-
Carmeli E, Kessel S, Coleman R, Ayalon M (2002) Effects of a treadmill walking program on muscle strength and balance in elderly people with Down syndrome. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences 57(2): M106-10.
-
Jimshad TU, Sanam Mainali, Swethankh KS, Anil T John (2016) Does Q angle change in spastic diplegia children ?, Indian journal of cerebral palsy 2(2): 85-89.
-
Raveendranath R, Nachiket S, Sujatha N, Priya R, Rema D (2011) Bilateral variability of the quadriceps angle (Q angle) in an adult indian population. Iranian journal of basic medical sciences. 14(5): 465.
-
Akta Bhalara, Dhaval Talsaniya, Nikita, Nidhi Gandhi (2013) Q angle in children population aged between 7 to 12 years, International journal of health sciences & research 3(4): 57-64.
-
Khasawneh RR, Allouh MZ, Abu-El Rub E (2019) Measurement of the quadriceps (Q) angle with respect to various body parameters in young Arab population. PloS one 14(6).
-
Chhabra PK, Setiya M, Godwin R (2016) “Quadriceps angle”: An important indicator of biomechanical function of lower extremity and its relation with anterior knee pain. International journal of scientific study 4(7): 173- 176.
-
Ardolino E, Flores M, Manella K (2017) Gross Motor Outcomes After Dynamic Weight-Bearing in 2 Children With Trunk Hypotonia: A Case Series. Pediatric Physical Therapy 29(4): 360-364.
-
Lee J, Lee H, Lee W (2014) Effect of weight-bearing therapeutic exercise on the q-angle and muscle activity onset times of elite athletes with patellofemoral pain syndrome: a randomized controlled trial. Journal of physical therapy science 26(7): 989-992.
-
Ajlan Sac, Mehmet Yalcin Tasmektepligil (2018) Correlation between the Q angle and the isokinetic knee strength and muscle activity, Turk J Phys Med Rehab 64(4): 308-313.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial