Coexistent Carcinoma with Tuberculosis of the Lip - A Rare Cytologic Association
Granulomatous inflammation is considered to be an immune mechanism against infections or certain non-neoplastic conditions. Rarely granuloma formation may be noted in neoplastic disorders also. However a granulomatous response in the lymph nodes draining cancers is unusual. Such granulomas may sometimes show tumour cells in their centre. The exact cause of this phenomenon is not known but an immunologic reaction to tumour antigens has been suggested. A close scrutiny of such granuloma is necessary to avoid under diagnosis of a metastatic disease. A subtle morphological feature which may be helpful in differentiating a co-existing infection or tumour induced granuloma needs to be addressed. Granulomatous reactions occurring with carcinomas are a well known but uncommon occurrence. We report a case of 44 year old male with lip ulcer diagnosed as coexistent carcinoma of the lip with tuberculosis. FNAC of the lesions was characterized by the presence of scattered caseating epithelioid cell granulomas along with malignant squamous cells which was confirmed on histopathological examination.
Introduction
Granulomatous inflammation is considered to be an immune mechanism against infections or certain non- neoplastic conditions [1]. Rarely granuloma formation may be noted in neoplastic disorders also. Such granulomas may sometimes show tumour cells in their centre. The exact cause of this phenomenon is not known but an immunologic reaction to tumour antigens has been suggested. A close scrutiny of such granuloma is necessary to avoid under diagnosis [2]. Subtle morphological features which may be helpful in differentiating a co-existing infection or tumour induced granuloma need to be addressed.
Necrotizing granulomas have been described in patients with many types of malignancy (eg, lymphoma, testicular cancer, head and neck cancer, gastric cancer, renal cancer, and breast cancer) [3, 4]. Granulomas have been found surrounding the primary tumor or in the draining lymph nodes and probably reflect an immune response to tumor antigens [3]. The diagnosis requires a compatible clinicoradiologic picture and the demonstration of necrotizing granulomas. The granulomas are typically found adjacent to the tumor or lymphatic drainage route. One should not be persuaded away from a diagnosis of malignancy when caseating granulomas are present. Granulomatous reactions occurring within lymph nodes draining carcinomas are a well known but uncommon occurrence [1].
Case Summary
A 44-year-old male presented to the oral surgery clinic with complaints of a non-healing ulcer on the lower lip since the last 3 months despite of administration of antibiotics and topical medicated mouthwashes. He also complained of decrease in appetite and weight loss for the last 2 months. There was history of low grade fever with expectorating cough. He gave no history of haemoptysis. The patient was from a low socioeconomic status and a chronic tobacco smoke with Gutka chewing for the last 20 years.
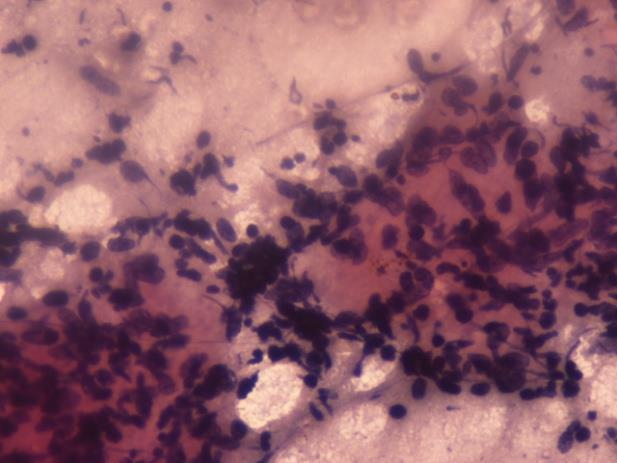
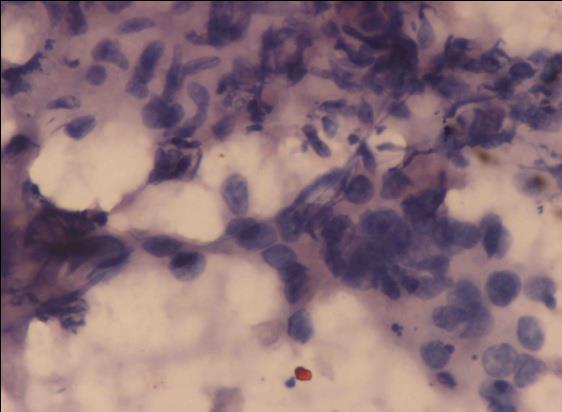
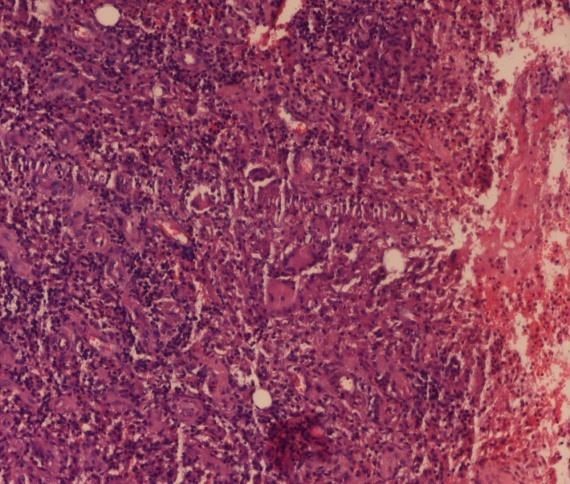
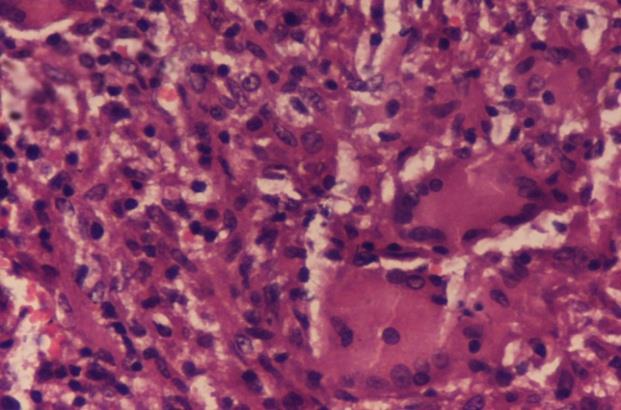
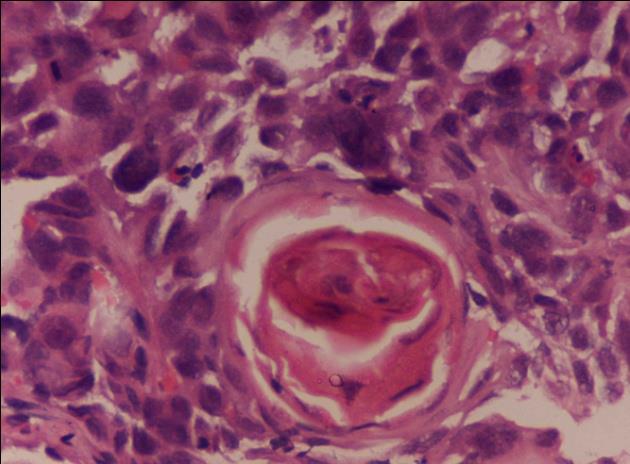
On examination, the patient was thin built, appeared pale and unwell. He had an ulcerated lesion on the lower lip, 3 cm x 1 cm in size with a shallow ulcerated base and rolled margins with poor oral hygiene. There was no evidence of any lymphadenopathy. A strong clinical suspicion of malignancy was elicited. FNAC of the lesion was performed which was characterized by the presence of scattered caseating epithelioid cell granulomas along with malignant squamous cells (Figures 1 & 2). An urgent incision biopsy was performed under local anaesthesia. Microscopic examination revealed an inflamed ulcerated lesion with several epithelioid cell granulomas with langhan’s giant cells (Figures 3 & 4) and irregular sheets of highly atypical squamous cells with keratin pearl formation (Figure 5). However several acid-fast bacilli were identified with Ziehl-Neelson stain leading to a diagnosis of ulcerated lip tuberculosis with squamous cell carcinoma.
Blood tests were within normal limits except for a raised white cell count with lymphocytosis, a raised erythrocyte sedimentation rate (96 mm in 1st hour) and a raised C-reactive protein (77.6 mg/L). Chest x-ray showed a minor degree of consolidation and cavitations in the right upper lobe, consistent with tuberculosis. He was prescribed 4 drugs anti-tubercular treatment of Rifampicin, Isoniazid, Ethambutol and Pyrazinamide for 9 months with Co-60 radiation therapy x 25 fractions and adjuvant cispatinum chemotherapy (50 mg/m2 x 6 cycles). After 6 months of follow up period, the condition of the patient has improved with complete resolution of the lip lesion.
Discussion
Diagnosis of granulomatous inflammation is a common practice in pathology. The common causes of granulomatous inflammation are infective agents like mycobacterium, fungi, parasites and non-infective aetiologies like breast carcinoma, gastric, colonic and laryngeal cancer, sarcoidosis, foreign bodies, Wegener’s granulomatosis, Hodgkin’s and Crohn’s disease [4, 5]. Few instances of granulomatous non-Hodgkin T cell lymphomas, seminoma of the testis, renal cell carcinoma, nasopharyngeal carcinoma and ovarian dysgerminoma have been reported [5, 6]. This interesting observation of granulomas in the tumour parenchyma can be attributed to the cytokine milieu of the main tumour cells [2].
FNAC of the lesions was characterized by the presence of scattered epithelioid histiocytes and multinucleated langhan’s-type giant cells along with lymphocytes and plasma cells. Granuloma is a focus of chronic inflammation consisting of microscopic aggregation of macrophages that are transformed into epithelial like cells, surrounded by a collar of lymphocytes and occasionally plasma cells [1, 2].
Our study demonstrated a case of squamous cell carcinoma of the lip with associated tubercular inflammation. Cases of granulomatous inflammation in the lymph nodes draining the primary tumour either with or without metastatic cancer have been reported [3]. It has been observed in many malignancies arising from breast, stomach, colon and larynx can be associated with a granulomatous response in the draining lymph nodes and should be included in the list of differential diagnosis of causes of granulomatous inflammation. Whenever a granuloma is seen in the draining lymph node in a known case of cancer it should be carefully scrutinized for the presence of malignant cells [7, 8].
The granulomatous reaction may be a response to the presence of necrotic material or stromal granulomatous response adjacent to the foci of carcinoma. Granuloma containing centrally located malignant cells is a foreign body inflammatory response or an immunological reaction, whereas the granulomatous response within draining lymph nodes represents a response to soluble tumour related antigens and the stromal reaction represents a T cell mediated immunological response to cell surface antigens [2, 3] The synchronous presence of granulomatous reaction and carcinoma in our patient, supports the contention that this is a very early immunological response to surface antigens.
Conclusion
Granulomatous inflammation is very common, with tuberculosis being the most common cause of granulomas. Cooperation between the clinician and the pathologist is important, if the patient is to derive the greatest benefit from the biopsy. This percentage can be further consolidated, if microbial culture, serological investigations and PCR are done.
References
-
Oberman H (1987) Invasive carcinoma of the breast with granulomatous response. Am J Clin Pathol 88(6): 719-721.
-
Watterson J (2012) Epithelioid granulomas associated with hepatocellular carcinoma. Arch Pathol Lab Med 106: 538-539.
-
Blackshaw A (2010) Metastatic tumour in lymph nodes. In: Stansfield AG, [Eds.], Lymph node biopsy interpretation. London: Churchill-Livingstone pp: 380-397.
-
Williams GT, Williams WJ (2013) Granulomatous inflammation - a review. J Clin Pathol 36(7): 723-733.
-
Adams DO (1976) The granulomatous inflammatory response. Am J Pathol 84(1): 164-187.
-
Alka B, Yashwant K, Anjali SK (2009) Granulomatous inflammation in lymph nodes draining cancer: A coincidence or a significant association. Int J Med Med Sci 1(2): 13-16.
-
Marcus PK, Carlos AJ, Ashwini DM, Rodolfo CM, Georgie AE (2010) Clinical implications of granulomatous inflammation detected by endobronchial ultrasound transbronchial needle aspiration in patients with suspected cancer recurrence in the mediastinum. J Cardioth Surg 3: 8- 12.
-
Paari M, Robert E, Bihong J (2010) Nonspecific granulomatous prostatitis with prostatic adenocarcinoma. Ind J Pathol Microbiol 53(1): 152- 154.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet