"Progressive Metabolic Acidosis or Bicarbonate Measurement Error?"
Accurate bicarbonate measurement is critical for assessing acid-base status. This study characterizes the cause of an unexpected discrepancy between a common bicarbonate assay and the bicarbonate calculated from blood gasses in nine cases identified at a single medical center over a 12-month observation period. Hospitalized patients with at least a 3 mEq/L difference between the plasma bicarbonate measured by a photometric assay and a blood gas were investigated to determine the cause. All patients experienced a fall in measured bicarbonate associated in clinical scenarios in which progressive metabolic acidosis was suspected. Electrolyte, acid-base status, triglyceride, turbidity index and clinical histories were obtained in all patients. The mean bicarbonate discrepancy was >8 mEq/L (range 3.4-12 mEq/L). All patients (9/9) experienced transient hyperlipidemia that persisted as the lipid level fell below that typically detected by a turbidity index and was not matched by a fall in pH or the calculated bicarbonate level. The effect of lipid addition and removal on measured bicarbonate was investigated to replicate or minimize the detected bicarbonate discrepancy, respectively. A positive correlation between the severity of the bicarbonate discrepancy measured by a common photometric assay and hyperlipidemia occurred. This discrepancy persisted below the lipid level detected by a visual turbidity index, was not matched by a fall in pH or the calculated bicarbonate level. Lipid interference is distinct from the dilutional mechanism of pseudohyponatremia and is independent of the specific autoanalyzer, operator, and institution. Pseudohypobicarbonatemia increased resource utilization in the absence of clinical deterioration or supporting laboratory data to suggest progressive metabolic acidosis. At high levels, the addition of exogenous lipid replicated the bicarbonate discrepancy. We show that pseudohypobicarbonatemia is associated with transient hyperlipidemia. Lipid removal from blood samples prior to biochemical assay combined with increased clinical awareness of this phenomenon minimizes the untoward impact of this phenomenon resource utilization and clinical practice.
Introduction
In the proper clinical setting, a fall in serum bicarbonate concentration, linked with a rise in the anion gap, suggests progressive metabolic acidosis. Metabolic acidosis consumes bicarbonate and often decreases systemic pH. A fall in systemic pH perturbs tertiary protein structure, reduces enzyme activity, and interferes with protein-protein interactions [1]. A reduction in bicarbonate also compromises buffering capacity, causing the systemic milieu to be poorly defended against additional acid-base perturbations [2]. As a result of these biologic consequences, hypobicarbonatemia profoundly affects clinical decision-making. Specifically, hypobicarbonatemia in the setting of progressive acidemia mandates urgent investigation to identify and reverse its cause, usually prompts intravenous fluid therapy, often in an intensive care setting [2].
Discrepancy between the measured and calculated plasma bicarbonate concentration confounds clinical decision-making and jeopardizes appropriate medical care. This is especially true when a deteriorating acid- base status is discordant with patients’ clinical state. Although such discrepancies have been sporadically reported, we collected nine cases over a 12-month time period that highlight an important and potentially avoidable cause of pseudohypobicarbonatemia. We suggest an effective, practical approach for minimizing the discrepancy between measured and calculated bicarbonate levels that directly address this unexpected phenomenon.
Methods
Case Selection: The index case was discovered as an unexplained discrepancy between the measured and calculated plasma bicarbonate levels. The subsequent cases were identified by the presence of increased plasma turbidity (lipemia index 4+) detected by the auto-analyzer (suggesting hyperlipidemia) and a discrepancy of at least
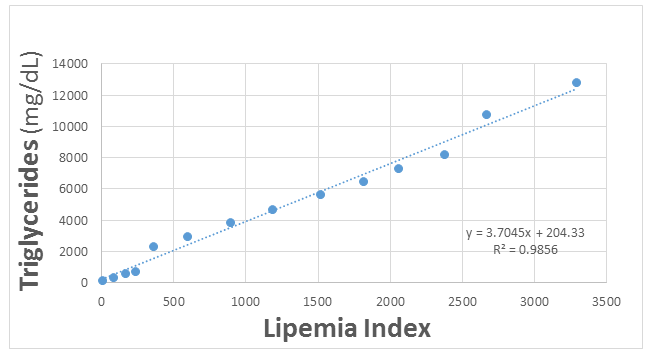
3 mmol/l between the measured and calculated bicarbonate values. Bicarbonate Determinations: An auto-analyzer (manufactured by Abbott, Abbott Park, IL or Roche, Indianapolis, IN) was used to measure total CO2 (bicarbonate + dissolved CO2 in solution) values in plasma obtained in heparinized tubes from hospitalized patients during routine care for acute illnesses. This technique uses a standard photometric reaction to determine the total carbon dioxide content in serum or plasma blood samples, using an enzymatic assay that is reportedly linear between 5 and 50mmol/l [3]. For ease of comparison and given their near equivalence, total plasma CO2 is hereafter referred to as bicarbonate concentration [4]. Bicarbonate was also calculated from the Henderson-Hasselbalch equation [5, 6] in venous blood gas samples in which pH and pCO2 were directly measured (Radiometer; Brea, CA). Intralipid Assay: A solution containing 20% homogenous fat particle in emulsion; (IntralipidTM Baxter, Deerfield, IL) was added to human plasma samples to achieve a final triglyceride concentration of 136-12,800 mg/dL. The effect of triglyceride addition on plasma bicarbonate measured by the photometric technique was determined in serial human blood samples.
Results
A 54-year-old man with well-controlled diabetes mellitus (A1C 6.4 two months prior to admission) presented to his primary care clinic with acute respiratory symptoms consistent with an asthma exacerbation. Routine testing of venous serum at an outpatient facility using an auto-analyzer (Beckman Coulter, Brea, CA) revealed a plasma glucose of 446 mg/dLl, sodium of 138 mmol/L, chloride of 96 mmol/L, bicarbonate 15 mmol/L with a calculated anion gap of 27 mmol/L. Urinalysis revealed 3+ urine ketones and 3+ glucosuria, suggesting diabetic ketoacidosis (DKA) as the presumptive diagnosis [7]. The patient was referred to the Emergency Department (ED) at Boston University Medical Center for further management of metabolic acidosis and hyperglycemia.
In the ED, the point of care finger-stick glucose measured 362 mg/dL. A venous blood gas (VBG) revealed a pH of 7.28, partial pressure of carbon dioxide (PCO2) of 39.4 mmHg, and bicarbonate of 17.7 mmol/L, supporting the clinical suspicion of DKA with mild respiratory acidosis likely caused by carbon dioxide retention in the setting of reactive airways disease. The patient received 10 units of intravenous Lispro insulin, isotonic saline, potassium chloride replacement and bronchodilator therapy. A repeat VBG showed worsening mixed acidemia with a pH of 7.17, PCO2 52.6 mmHg, and bicarbonate 18.6 mmol/L. The patient received an additional 5 units of Lispro insulin before an arterial blood gas (ABG) revealed a pH of 7.27, PCO2 35 mmol/L, and plasma bicarbonate of 14.7 mmol/L. Point of care finger-stick glucose fell to 188 mg/dL and the patient was admitted to a medical-surgical floor for further management of his acidemia.
On the medical-surgical floor, basal and bolus insulin was initiated with NPH and Lispro insulin, respectively. Despite the absence of symptoms, his morning laboratory data performed for the first time on an Abbott auto- analyzer revealed a plasma venous bicarbonate of only 7.0 mmol/L and an anion gap of 21 mmol/L. Repeat venous plasma testing confirmed these findings (Table 1). The falling bicarbonate and increasing anion gap ostensibly suggested uncontrolled DKA, prompting urgent transfer to the medical intensive care unit (MICU) for intravenous insulin therapy.
| 1/13 | 1/13 | 1/14 | 1/14 | 1/14 | 1/14 | 1/14 | 1/14 | 1/15 | 1/15 | 1/15 | 1/16 | |||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1700 | 2100 | 0300 | 1000 | 1300 | 1400 | 1600 | 2000 | 000 | 0400 | 1600 | 0400 | |||||||||||||||||||||||||
| Venous plasma bicarbonate (mmol/l) | 7 | 5 | <5.0 | <5.0 | 6 | 17 | 18 | 22 | ||||||||||||||||||||||||||||
| Venous blood gas bicarbonate (mmol/l) | 17.2 | 18.6 | 14.9 | 14.5 | 15.5 | 20.1 | 23.7 | 23.2 | ||||||||||||||||||||||||||||
| Triglycerides (mg/dL) | 2179 | 1358 | 1134 | 860 |
Table 1: (Index Patient) Serial plasma bicarbonate concentrations measured by an auto-analyzer vs. calculated blood gas bicarbona
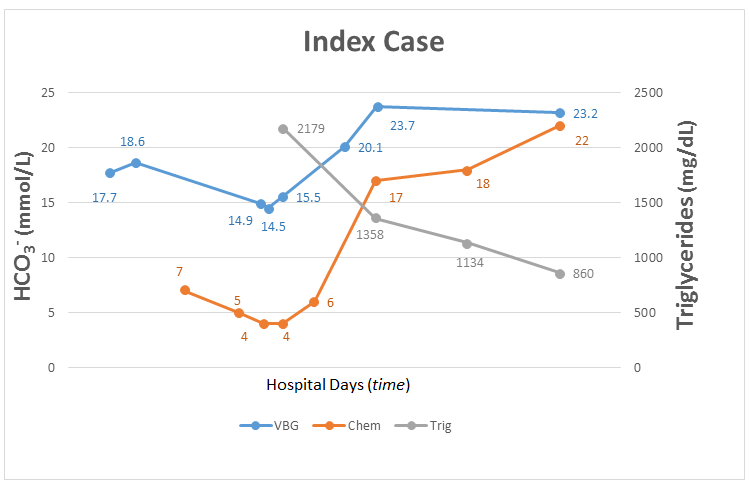
In the MICU, both intravenous insulin and isotonic bicarbonate infusions were initiated. The patient appeared well, exhibited normal vital signs, and had no specific medical complaints. Before the insulin and bicarb infusion were initiated, a venous blood gas (VBG) revealed a pH 7.30, PCO2 35 mmHg, and calculated bicarbonate of 15 mmol/L, suggesting a much less profound acidemia than measured by the venous chemistries. In fact, the calculated bicarbonate was 7 mmol/l higher than the measured bicarbonate value that prompted the urgent MICU transfer. In the intensive care unit, the patient remained clinically well, the blood lactate level was normal and blood cultures were negative for bacteria. Repeat venous blood gases (Table 1) consistently revealed calculated bicarbonate levels that were approximately 8-10 mmol/L higher than the bicarbonate levels measured in serial plasma samples by the auto-analyzer. Routine lipid screening showed profound hypertriglyceridemia of 2,179 mg/dL. During insulin treatment for the hyperglycemia, the patient’s triglycerides level fell to <1000 mg/dL at which time the discrepancy between the calculated VBG and measured plasma bicarbonate (as well as the accompanying anion gap) disappeared (Figure 1). The time course of the Day 1 Day 1 Day 2 Day 2 Day 2 discrepancy between measured and calculated bicarbonate levels vs. serum triglycerides is detailed (Table 1). The patient was transitioned to basal/bolus insulin therapy and received fenofibrate, an anti- hyperlipemic agent.
Recognition of the discrepancy between the bicarbonate values from two different methodologies, as well as the dissociation between the deteriorating acid- base and improving clinical status of the index case, prompted identification of eight additional cases over the subsequent six months. In each case, the bicarbonate discrepancy was associated with marked hypertriglyceridemia, usually associated with visible serum turbidity. Plasma sodium concentrations measured by an automated indirect potentiometric assay that incorporates sample dilution also differed from the values measured by a direct potentiometric in samples submitted for blood gas analysis (Table 2). The discrepancy is sodium measurement by these two assays averaged about 5 mmol/L during the period of peak hyperlipidemia and fell to 1 mmol/L as the triglyceride levels fell below 1,000 mg/dL.
Day 2
Day 2
Day 2
Day 3
Day 3
Day 3
Day 3
0400 Venous plasma sodium
Venous blood gas sodium (mmol/l) 137 137 136 138 137 139 138
These in vitro experiments suggested that marked hyperlipidemia caused by a homogenous lipid increases turbidity, thereby decreasing the bicarbonate concentration photometrically measured by the auto- analyzer. Furthermore, these experiments match the manufacturer’s recommendation that CO2 measurements are accurate only with triglyceride levels below 2,000 mg/dL. However, the marked in vivo “bicarbonate discrepancy” that persisted with blood triglycerides in the 1,000-2,000 mg/dL range was unexplained, potentially confounding clinical care at lesser but more commonly encountered degrees of hyperlipidemia.
To address this clinical challenge and minimize subsequent reporting of falsely low plasma measured bicarbonate levels, a procedural change was piloted by our clinical chemistry laboratory. Specifically, turbid venous samples detected by a markedly elevated lipemia index (i.e., an index of 4+ on a 0-4+ scale that reflects a serum triglyceride level above 200 mg/dL), were subjected to mechanical removal of the upper turbid lipid layer from the venous blood sample by a technician prior to sample processing by the auto-analyzer. In the twelve months after this procedural change was instituted, only three additional cases of bicarbonate discrepancy were detected. However, when this procedure change was combined with an automated warning regarding the potential for hypobicarbonatemia for plasma bicarbonate measurements < 15 mmol/l, no clinically important bicarbonate discrepancies were reported over the following 6 months of this study (Table 3).
| Venous tota | l | Venous blood | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age & | T | riglycerid | e | ( | HCO3 | ) | |||||||||||||||
| HCO 3 | gas HCO 3 | Active medical issues(s) | Key co-morbidities | ||||||||||||||||||
| Gender | (mg/dL) | mmol/l | |||||||||||||||||||
| (mmol/l) | (mmol/l) | ||||||||||||||||||||
| Index patient | 54 yo M | 2179 | <5.0 | 15.5 | >10.5 | DKA | DM | ||||||||||||||
| Patient 2 | 38 yo M | 3840 | 15 | 21.1 | 6.1 | Pancreatitis | DM | ||||||||||||||
| Patient 3 | 57 yo F | 2094 | 24 | 33 | 11 | None (routine blood work) | Pre-DM, HTN, alpha thalassemia minor | ||||||||||||||
| Patient 4 | 39 yo M | >4,000 | 19 | 24.5 | 5.5 | Pancreatitis | DM, alcohol use disorder | ||||||||||||||
| Patient 5 | 51 yo M | 3224 | 8 | 20 | 12 | Pre-B cell ALL on PEG- asparignase | HTN | ||||||||||||||
| Patient 6 | 41 yo M | 2174 | 14.4 | 24.6 | 10.2 | HHS, Pancreatitis STEMI | DM, CAD | ||||||||||||||
| Patient 7 | 63 yo M | 3018 | 15.6 | 21.4 | 5.8 | None (routine blood work) | DM | ||||||||||||||
| Patient 8 | 61 yo F | 2325 | 11 | 14.4 | 3.4 | DKA, influenza B | HIV, ILD | ||||||||||||||
| Patient 9 | 37 yo F | >4000 | 17 | 24.7 | 7.7 | Pancreatitis | DM |
Table 2: (Additional Cases of Bicarbonate Discrepancy) Over a 7-month time period following the index case, eight additional case
Table 3: (Additional Cases of Bicarbonate Discrepancy) Over a 7-month time period following the index case, eight additional cases of a bicarbonate discrepancy were detected in patients presenting with hyperlipidemia: 8/9 cases had primary hyperlipidemia and in a single case, hypertriglyceridemia was induced by chemotherapy. In all cases, there was at least a 3 mmol/L difference between auto-analyzer measurements of the plasma bicarbonate and the calculated venous blood gas bicarbonate. In each case, the bicarbonate discrepancy completely disappeared after the serum triglyceride level fell below 1,000 mg/dL (similar to our index case).
Discussion
The medical literature contains rare, isolated reports of single patients with a discrepancy between blood bicarbonate measurements and blood gas calculations wherein the measured value was deemed to be inaccurate. Rifkin et al. report a single case of pseudohypobicarbonatemia associated with hypertriglyceridemia. These authors posited that the hyperlipidemia and its accompanying turbidity interfered with the photometric analysis used to measure bicarbonate by lipid particle-induced light scattering [8]. Navaneethan, et al. described an outpatient with a persistent bicarbonate discrepancy but were unable to detect the interfering substance responsible for the observed discrepancy [9]. A similar phenomena was reported in a single neonate with congenital hyperlipidemia caused by lipoprotein lipase deficiency [10]. Finally, Goldwasser, et al. described another case in which two distinct paraproteins acted as the endogenous interfering substance associated with pseudohypobicarbonatemia [11]. In contrast to these single patient case reports, we assembled the only series to date of bicarbonate discrepancy detected at commonly encountered levels of hypertriglyceridemia and show that this unexpected phenomena is more common than expected.
Our index patient with mild DKA exhibited a peak of 12 mmol/L /L discrepancy between the plasma bicarbonate measured on the Abbott auto-analyzer and the bicarbonate calculated from the Henderson- Hasselbach equation using pH and the PCO2 values measured by a Radiometer blood gas analyzer. When a discrepancy occurs between these two laboratory determinations, it is common practice to accept the measured value from the venous chemistry rather than the calculated blood gas estimate [11], especially in the setting of an increased anion gap and suspected acidemia. In our index case, this practice prompted an unnecessary MICU transfer and unnecessary exposure of the patient to isotonic bicarbonate and insulin. At the time of the bicarbonate discrepancy, the plasma was grossly lipemic and turbid due to triglycerides in excess of 2,000 mg/dL. At this level, hypertriglyceridemia exceeds the maximum value that the manufacturer recommends for obtaining accurate bicarbonate measurements with the auto- analyzer (Abbott Architect bicarbonate package insert). Importantly, the observed bicarbonate discrepancy is not specific to a particular chemistry analyzer manufacturer. Virtually identical (and discrepant) plasma bicarbonate results in 20 blood samples from one of our cases were serially measured by a Roche Cobas chemistry analyzer that uses an identical biochemical bicarbonate assay also susceptible to photometric interference (case #9, data not shown).
In our series, the lower than expected plasma bicarbonate value measured by the Abbott auto-analyzer is aptly termed “pseudohypobicarbonatemia”. Similarly, sodium measurements in blood are well known to be lowered by interfering substances including lipids. This phenomenon is commonly referred to as pseudohyponatremia when the plasma osmolality is in fact normal. In pseudohyponatremia caused by hyperlipidemia, the excess lipids occupy space, resulting in inaccurate sample dilution characterized by the electrolyte exclusion effect [12]. Error is amplified by indirect potentiometric techniques that rely upon accurate sample dilution and assume a fixed percentage of solids by volume and a consistent diluent amount in each sample [13, 14]. Curiously, a 5 mmol/L discrepancy between the sodium concentration measured by auto- analyzer using a direct potentiometric assay in the blood gas sample and the indirect potentiometric technique used in the autoanalyzer was also present in our index patient (Table 2). This 5 mmol/L sodium concentration discrepancy is likely due to the electrolyte exclusion effect of excess lipid that alters the indirect sodium assay [13, 15] and is identical in magnitude to a prior report [16]. In contrast, it is highly unlikely that falsely low bicarbonate level reported here is caused by an electrolyte exclusion since a dilution step is not required for the photometric auto-analyzer assay. In our index case (as well as in the subsequent eight cases), we propose that the turbidity in the blood likely caused by VLDL and chylomicrons that positively correlate with triglyceride level [17] interferes with the photometric–based bicarbonate assays commonly used by current auto-analyzers. Therefore, the phenomenon of pseudohypobicarbonatemia is distinct from the effect of solid mass occupied by VLDL and chylomicrons that result in inaccurate sample dilution in pseudohyponatremia [12]. In our index patient, a bicarbonate discrepancy existed even with initial triglyceride levels between 1,000-2,000 mg/dL. In fact, it was not until the triglyceride level fell to < 1,000 mg/dL that the discrepancy between the plasma bicarbonate and the venous blood gas bicarbonate disappeared. This observation suggests that a factor(s) other than total triglyceride level interfere(s) with photometric-based bicarbonate measurements. Rifkin, et al., suggested that the specific lipid composition, rather than the absolute level interferes with standard photometric assays [8]. These authors also suggested that visual inspection, followed by the addition of Lipo-Clear (Beckman Coulter, Brea CA), a commonly used lipid adsorbent, to lipemic samples might eliminate the problematic bicarbonate discrepancy with a photometric technique. In contrast to adding Lipo-Clear, we elected to physically remove the lipid from grossly lipemic samples, a maneuver that limits interference by lipids in excess of 200 mg/dL. This procedural change decreased but did not eliminate, bicarbonate discrepancy, supporting the current hypothesis that specific lipid particles or particle size(s) cause interference with photometric assay.
We concur with Rifkin, et al. that a lower turbidity threshold for adding a lipid adsorbent (e.g., 3+ rather than 4+ turbidity) or physically removing the “lipid layer” prior to obtaining photometric measurements in the chemistry analyzer would likely eliminate “factitious- hypobicarbonatemia” [8]. Lowering the screening criteria from 4+ to 3+ turbidity index would identify samples with lipid levels of about 100 mg/dL, a level that approximates the normal lipid range. However, such strict turbidity criteria would be less cost-effective due to the additional steps required to process a much larger number of samples. To balance accuracy and cost, we suggest lipid removal (either manually or with an absorbent) in all samples with 4+ turbidity prior to measuring bicarbonate in all auto-analyzers that rely on a photometric assay. However, if less stringent turbidity criteria are used or if the upper serum layer is not routinely removed from all samples, clinical judgment is required to identify the remaining cases of pseudohypobicarbonatemia at lipid levels that escape visual detection. In the presence of measured and calculated bicarbonate discrepancy but absent clinical deterioration (tachypnea, tachycardia, hypotension, and/or altered mental status), we suggest that unexpectedly low serum or plasma bicarbonate concentration measured by the photometric technique be confirmed by arterial or venous blood gas measurement. This recommendation is based on our repeated observation that in the presence of interfering lipids, calculated bicarbonate levels are more accurate and clinically useful than photometric measurements. In the present study, it is not possible to ascertain the identity, size, or composition of the specific lipid particle that interfere with photometric bicarbonate assays. However, it is clear that the total lipid level alone does not sufficiently predict assay interference. Comparative mass spectrometry of blood samples before and after triglyceride lowering will likely be required to identify the substance(s) responsible for interfering with photometric bicarbonate assays in specific patients.
Conclusion
We report nine cases of clinically important discrepancies between measured and calculated plasma bicarbonate concentrations. In these cases, the fall in measured serum bicarbonate was not accompanied by progressive signs or symptoms of metabolic acidemia. The bicarbonate discrepancy described in all nine cases represents a transient phenomenon associated with stress-induced hyperlipidemia [18] in contrast to single case of persistent pseudohypobicarbonatemia [19]. In our cases, metabolic stress associated with diabetes, hyperglycemia, and ketoacidosis was sufficient to trigger hypertriglyceridemia [20]. Based on our preliminary study, we suggest a multifaceted approach to address the problem of bicarbonate discrepancy. First, automated screening for turbidity in blood samples should be used to initiate removal of the interfering lipid. This can be achieved either by ultracentrifugation of the sample or the addition of a lipid adsorbent. This approach will effectively detect samples with greater than 200 mg/dL triglyceride content (4+ turbidity) but will not eliminate lipid interference in samples with 3+ or lower turbidity that reflect normal lipid levels. Second, we suggest that laboratories add the following warning to report bicarbonate results < 15 mmol/l: “Elevated triglycerides levels (>1,000 mg/dL) may cause falsely low bicarbonate results. If clinically indicated, a venous blood gas should be ordered to confirm the serum bicarbonate results.” Finally, we suggest that clinicians are aware of the potential for bicarbonate discrepancy and employ clinical judgement, especially in cases in which apparent hypobicarbonatemia occurs in the absence of clinical urgency.
References
-
Sahin E, Grillo AO, Perkins MD, Roberts CJ (2010) Comparative Effects of pH and Ionic Strength on Protein-Protein Interactions, Unfolding, and aggregation for IgG1 antibodies. J Pharm Sci 99(12): 4830-4848.
-
Adrogué HJ, Madias NE (1998) Management of Life- Threatening Acid-Base Disorders. N Engl J Med 338(1): 26-34.
-
Norris KA, Atkinson AR, Smith WG (1975) Colorimetric Enzymatic Determination of Serum Total Carbon Dioxide, as applied to the Vickers Multichannel 300 Discrete Analyzer. CLIN CHEM 21(8): 1093-1101.
-
Centor RM (1990) Serum Total Carbon Dioxide. Butterworths.
-
Henderson LJ (1908) Note on the union of the protines serum with alkali. American Journal Physiology 21(2): 169-172.
-
Henderson LJ (1908) The Theory of neutrality regulation in the animal organism. Am J Physiol 21(4): 427-448.
-
Kitabchi AE, Umpierrez GE, Miles JM, Fisher JN (2009) Hyperglycemic Crises in Adult Patients With Diabetes. Diabetes Care 32(7): 1335-1343.
-
Rifkin SI, Shaub B (2014) Factitious hypobicarbonatemia associated with profound hyperlipidemia. Ren Fail 36(7): 1155-1157.
-
Navaneethan SD, Mooney R, Sloand J (2008) Pseudo- anion gap acidosis. NDT Plus 1(2): 94-96.
-
Ashraf AP, Hurst ACE, Garg A (2017) Extreme hypertriglyceridemia, pseudohyponatremia, and pseudoacidosis in a neonate with lipoprotein lipase deficiency due to segmental uniparental disomy. J Clin Lipidol 11(3): 757-762.
-
Goldwasser P, Manjappa NG, Luhrs CA, Barth RH (2011) Pseudohypobicarbonatemia ct5ttttttttaused by an Endogenous Assay Interferent: A New Entity. Am J Kidney Dis 58(4): 617-620.
-
Aw TC, Kiechle FL (1985) Pseudohyponatremia. Am J Emerg Med 3(3): 236-239.
-
Albrink MJ, Hald PM, Man EB, Peters JP (1955) The Displacement of Serum Water by the Lipids of Hyperlipemic Serum; a New Method for the Rapid Determination of Serum Water. J Clin Invest 34(10): 1483-1488.
-
Weisberg LS (1989) Pseudohyponatremia: A reappraisal. Am J Med 86(3): 315-318.
-
Kim GH (2006) Pseudohyponatremia: Does It Matter in Current Clinical Practice?. Electrolyte Blood Press 4(2): 77-82.
-
Langhoff E, Steiness I (1982) Potentiometric analysis for sodium and potassium in biological fluids. Clin Chem 28(1): 170-172.
-
Kroll MH, McCudden CR (2013) Endogenous Interferences in Clinical Laboratory Tests : Icteric, Lipemic, and Turbid Samples. De Gruyter.
-
Nonogaki K, Moser AH, Feingold KR (1944) Grunfeld C Alpha-adrenergic Receptors Mediate the Hypertriglyceridemia Induced by Endotoxin, but not Tumor Necrosis Factor in Rats. Endocrinology 135(6): 2644-2650.
-
Cartier JL, Look DC, Dunn JP (2018) Pseudohypobicarbonatemia in a patient presenting with suspected diabetic ketoacidosis. AACE Clin Case Reports 4(2): 108-111.
-
Yuan G, Al-Shali KZ, Hegele RA (2007) Hypertriglyceridemia: its etiology, effects and treatment. CMAJ 176(8): 1113-1120.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet