Ameloblastic Fibrosarcoma an Uncommon Odontogenic Tumor of Right Maxilla
Ameloblastic Fibrosarcoma (AFS) is an uncommon mixed odontogenic tumor composed of a benign epithelial and a malignant ectomesenchymal component. We report a case of a 15 year old female presented with a history of painful swelling over right maxilla of 6 months duration. On examination showed an irregular greyish white solid mass measuring 4.5 x 3.4 cm. On radiograph CT Neck (plain and contrast) showed mass lesion in right maxillary sinus with erosion of its floor and extending into right gingivo-buccal space. Features suggestive of neoplastic pathology. The right subtotal maxillary resection was done. On histopathological evaluation showed an irregular greyish white solid mass measuring 4.1 x 3.4 x 3.3 cm. On cut section showed grey white fleshy tumor. On histopathology reported as ameloblastic fibrosarcoma. We are presenting this extremely rare case for its clinical, radiological and histopathological features.
Sunil V Jagtap1*, Shubham S Jagtap2, Nupura Vibhute3, Digvijay Patil4 and Shefali Mishra5
Keywords: Malignant Tumors of Maxilla; Mixed Odontogenic Tumor; Ameloblastoma; Jaw Tumors
Introduction
Odontogenic tumors are derived from epithelial ectomesenchymal and mesenchymal elements of the tooth forming apparatus. AFS is extremely uncommon tumor to the best of our knowledge, less the 100 cases have been reported in English literature [1]. AFS was first reported by Heath in 1887 [2]. AFS is a rare mixed odontogenic tumor that consists of a benign epithelial component and a malignant ectomesenchymal stroma. It is thought to be malignant counterpart to ameloblastic fibroma. The other term used variant like ameloblastic fibrodentinosarcoma are used when dentin is present in the malignant stroma while ameloblatic fibroodontosarcoma is used when enamel is present in the malignant stroma. In our case no such finding were observed on multiple tissue sections studied.
A case of a 15 year old female presented with a history of painful swelling over right maxilla of 6 months duration. Swelling was extending in right upper gingivo-buccal sulcus. It was incidious in onset gradually increasing in size without any noticed aggravating or relieving factors. There was no history of smoking or tobacco use. Patient had history of a swelling in right buccal vestibule extending from 13 to 18th region and over crest of alveolus. The biopsy report at that time was features suggestive of ameloblastoma. Now on radiograph CT Neck (Plain & Contrast) showed mass lesion in right maxillary sinus with erosion of its floor and extending into right gingivo-buccal space. Feature suggestive of neoplastic pathology. There is no evidence of any lymphadenpathy. The patient underwent a right subtotal maxillary resection. On gross examination a swelling in right buccal vestibule extending from 13 to 18th region and over crest of alveolus, also extending over right side of cheek was noted. On examination showed an irregular greyish white solid mass measuring 4.1 x 3.4 x 3.3 cm. On cut section showed grey white fleshy tumor (Figure 1).
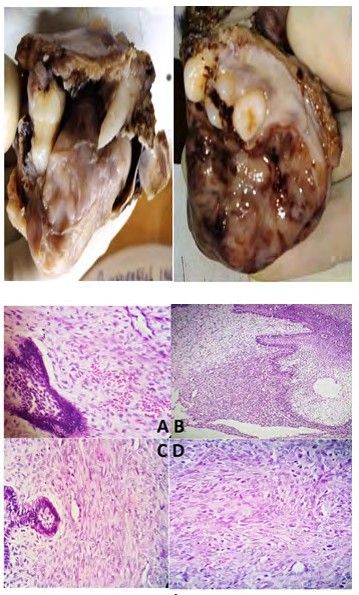
On microscopy showed biphasic tumor of benign epithelium and malignant stroma (Figures 2A-2D). The benign odontogenic epithelium with ameloblastic appearance having peripheral palisidation. Tumor arranged in islands, strands, cords and nest, reverse marginization with large tumor islands was noted. Malignant stroma of spindle cells and mild to severe pleomorphism, atypia, hyperchromasia and increased mitosis was noted. The surface epithelium shows ulceration, hyperplasia and dysplasia. On histopathological evaluation reported as Ameloblastic Fibrosarcoma.
Figures 2A-2D: Ameloblastic fibrosarcoma: A) Biphasic tumor of benign epithelium and malignant stroma (Low power view H&E stain) B) Tumor cells usually arranged in islands, strands, cords and nest C) Biphasic tumor of benign epithelium and malignant stroma High power view (H&E stain) D) Malignant stroma of spindle cells and mild to moderate pleomorphism, atypia, hyperchromasia and increased mitosis were noted. Areas of tumor cells in herrington or storiform pattern (High power view H&E stain).
Discussion
AFS is an uncommon odontogenic tumor [3]. Clinically these patients present with facial swelling, pain or paraesthesia. It is reported that half of the cases arises from Ameloblastic Fibroma [4, 5]. AFS can arise de novo. The mandible is the most commonly affected site. The maxilla is rarely affected. The maxillary tumors tend to show antral involvement with apparent erosion of the sinus walls and invades adjacent soft tissues. The common age affected is younger with mean 28 years of age, having Male: Female ratio of 16:1 [4]. In our case it was presented at the age of 15 years and recurred after 6 months of previous surgical excision. On radiological imaging these lesions present as a radiolucent masses with ill-defined borders. The unilocular or multilocular cystic cavities having expansile mass with cortical perforations are evident. It is observed that erosion and destruction of bony tissue may appear. In our case mass lesion with cystic cavity and massive intra oral extension was noted.
On histologic examination typically biphasic tumor of benign epithelium and malignant stroma is noted. The benign odontogenic epithelium with ameloblastic appearance having peripheral palisidation is observed. Tumor cells usually arranged in islands, strands, cords and nest, reverse marginization with large tumor islands are noted. Malignant stroma of spindle cells and mild to severe pleomorphism, atypia, hyperchromasia and increased mitosis were noted. Areas of tumor cells in herrington or storiform pattern are also noted. The diagnosis is dependent on clinical, radiological and pathological findings. It is important to differentiate AFS from ameloblastic fibroma and ameloblastoma. Ameloblastic fibroma (AF) and AFS have a biphasic nature; however, AF has no malignant component. AFS can arise de novo or from a previous ameloblastic fibroma. On histopathology features of malignancy like pleomorphism, nuclear hyperchromasia, increased mitosis, occasional tumor giant/bizarre cells, areas of haemorrhage and necrosis vascular and neuronal invasion are helpful to differentiate from above.
The conditions having myxoid and malignant stromal spindle cell component including myxofibrosarcoma, myofibrosarcoma, and fibroblastoma should be properly look out as a differential diagnosis [6]. Several IHC studies with Vimentin, Ki-67, Bcl-2, PCNA, c-Kit, p53, AE1/AE3, pancytokeratin have been described but histological diagnosis has an important role [7]. AFS shows locally aggressive tumor with high recurrence rate (40-50%) [8, 9]. However local or distant metastasis are not so common, A case of pulmonary and hepatic metastases of mandibular ameloblastoma was reported [10]. The treatment modality is wide surgical resection which is optimal. The neck dissection is not usually indicated, as regional lymph node metastases are very rare. The use of adjuvant chemotherapy and radiotherapy will be helpful for good prognosis. The cases require long term follow up.
Conclusion
AFS is an uncommon malignant odontogenic tumor with high rate of local recurrence. In our case it showed aggressive clinical behaviour with early recurrence.
References
-
Hu YY, Deng MH, Yuan LL, Niu YM (2014) Ameloblastic fibrosarcoma of the mandible: a case report and mini review. Experimental and Therapeutic Medicine 8(5): 1463-1466.
-
Heath C (1887) Lectures on certain diseases of the jaws. Br Med J 2: 5.
-
Huguet P, Castellvi J, Avila M, Alejo M, Autonell F, et al. (2001) Ameloblastic fibrosarcoma: report of a case. Immunohistochemical study and review of the literature. Med Oral 6(3): 173-179.
-
Lai J, Blanas N, Higgins K, Klieb H (2011) Ameloblastic fibrosarcoma: report of a case, study of immunophenotype, and comprehensive review of the literature. J Oral and Maxillofacial Surgery 70(8): 2007- 2012.
-
Noordhoek R, Pizer ME, Laskin DM (2012) Ameloblastic fibrosarcoma of the mandible: treatment, long-term follow-up, and subsequent reconstruction of a case. J Oral and Maxillofacial Surgery 70(12): 2930-2935.
-
Jagtap SV, Jain A, Jagtap SS, Kshirsagar AY (2015) High- grade myxofibrosarcoma-presented as a large mass of right upper arm. Indian J Pathol Microbiol 58(1): 105- 107.
-
Pontes HA, Pontes FS, Silva BS, Cury SE, Fonseca FP, et al. (2010) Immunoexpression of Ki67, proliferative cell nuclear antigen, and Bcl-2 proteins in a case of ameloblastic fibrosarcoma. Ann Diagn Pathol 14(6): 447-452.
-
Marx RE, Stern D (2012) Oral and Maxillofacial Pathology: A Rationale for Diagnosis and Treatment. 2nd (Edn.), Quintessence Publishing Co.
-
Kobayashi K, Murakami R, Fujii T, Hirano A (2005) Malignant transformation of ameloblastic fibroma to ameloblastic fibrosarcoma: Case report and review of the literature. J Cranio-maxillo-facial Surg 33(5): 352- 355.
-
Kilara N, Subramanian M, Koushik K (2007) Unusual case of pulmonary and hepatic metastases of mandibular ameloblastoma. Indian J Medical & Paediatric Onco 28(3): 31-33.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet