Comparison of P Cadherin (Myoepithelial Cell Marker) Expression in Benign and Primary Malignant Breast Tumors
Introduction: Breast cancer is the second most common cancer in the world and, by far, now the most common cancer in women in India. It becomes important to recognize benign lesions, both to distinguish them from in situ and invasive breast cancer and to assess a patient’s risk of developing breast cancer, so that the most appropriate treatment can be given. Material and methods: The present study was a cross sectional observational study, conducted on breast tissue specimens received in the department of Pathology, P.G.I.M.E.R & Dr. R.M.L Hospital, New Delhi, in collaboration with the Department of Surgery, from the period of 1st November 2013 to 31st March 2015. The sample size for this study was 80. Histological assessment was done and Immunohistochemistry was applied on all the cases using P-caherin antibody. Results: Out of a total of 40 benign cases, 100% cases showed positive staining with P Cadherin. Whereas for 40 malignant cases studied, 24 cases (60%) showed no staining. The staining index for them was zero. 7 cases (17.5%) showed staining index between1-3. A comparison of P cadherin positivity was done between all benign and malignant cases. The association between the type of lesion of the breast and result of IHC staining is considered to be statistically significant. Conclusion: P-cadherin is a highly sensitive marker for myoepithelial cells. Its expression strongly correlates with the type of breast lesion, which can help in differentiation between benign and malignant lesions whenever there is confusion in diagnosis with routine methods.
Introduction
Cadherins are cell-cell adhesion glycoproteins that form calcium-dependent intercellular junctions and play an essential role in morphogenesis, development and maintenance of adult tissues and organs [1]. The cadherin family is subdivided into various subfamilies including classical E-, P-, and N-cadherin. E Cadherin is the predominant cadherin family member, expressed in all epithelial tissues and is extremely important in maintenance of cell shape and polarity. Its gene CDH1 acts as a tumor supressor gene, negatively regulating the invasion and metastasis of tumor cells in several malignancies [2]. In contrast, N Cadherin is upregulated in several cancers and contributes to an invasive phenotype by interlacing with fibroblast growth factor (FGFR) and its downstream signalling [3]. The expression of P-cadherin is only restricted to basal or lower layers of stratified epithelia, including prostate and skin and also to breast myoepithelial cells (MECs) [4].
In normal breast, the epithelium throughout the ducts and lobules is bilayered, consisiting of an inner epithelial layer and an outer myoepithelial layer. Outer MECs are spindle-shaped contractile, smooth muscle like cells [5]. The importance of this double cell layer cannot be ignored because it is one of the main guides to the distinction between benign and malignant lesions. This myoepithelial layer is present around normal ducts and lobules, benign lesions, including sclerosing adenosis and radial scars, and ductal carcinoma in situ (DCIS), but not around invasive carcinoma. As loss of this layer is hallmark of infiltrating carcinomas in breast, it can be targeted by different myoepithelial markers in aiding diagnosis in difficult cases.
There are various benign and malignant breast lesions that can be difficult to differentiate histologically and which, therefore, can cause diagnostic problems. The frequency of this occurring has increased with the introduction of mammographic screening—for example, differentiating between tubular carcinoma and radial scar. Another problem area is the determination of the presence or absence of invasion in cases of ductal carcinoma in situ.
The presence of myoepithelial cells has been recognised to be of value in the assessment of these diagnostic problems. The markers used for their identification include smooth muscle actin (SMA), S100, and cytokeratin 14, but some problems have been reported with these—for example, SMA is also present in myofibroblasts and S100 can be present in normal hyperplastic and neoplastic epithelium, in addition to myoepithelial cells [6].
In this study we will assess the ability of immunohistochemical (IHC) marker, P-cadherin, to distinguish between benign and malignant breast lesions, through evaluating the P-cadherin expression in different benign and malignant lesions of breast by scoring grades.
Material and Methods
The present study was conducted on all breast tissue specimens including trucut biopsies, lumpectomy and mastectomy specimens received in the department of Pathology, P.G.I.M.E.R & Dr. R.M.L Hospital, New Delhi, in collaboration with the Department of Surgery, from the period of 1st November 2013 to 31st March 2015. This study was a cross sectional observational study. The sample size for this study was 80 cases (40 benign and 40 malignant).
The specimens included in the study were all benign lesions of breast and primary breast cancers. While inflammatory lesions, traumatic lesions, metastatic lesions of breasts, lymphoma, lesions in male breast and patients who received preoperative chemotherapy and radiotherapy were excluded from the study.
Trucut biopsy specimens were whole processed and on lumpectomy and mastectomy specimens all margins (i.e. deep resected margin, lateral margins, superior and inferior margin) were inked and cuts were made to identify the tumor and fixed in 10% neutral buffered formalin for appropriate time till the tissue was well fixed. Sections from tumor and other necessary areas were taken.
The sections were processed in automatic tissue processor (Shandon Citadel 2000). Paraffin embedded tissue were cut at 4µm thickness using rotary microtome (Shandon) and sections were stained with Hematoxylin and Eosin. Histological assessment was done and histopathological diagnosis was documented. Immunohistochemistry was applied on all the cases using P-caherin antibody.
The P -cadherin reactivity was graded by determining the percentage of P cadherin immunoreactive cells, i.e. brown membranous and/or cytoplasmic reactivity and intensity of staining.
Intensity score (IS) of IHC reaction, as viewed under light microscope, are as follows: 0 – Negative 1 – Weak 2 – Medium 3 – High Proportional score (PS) cells showing staining:
- No staining
- 1-10%
- 11-50%
- >50% Total score (TS) = IS x PS (0-
Results
Eighty cases of breast lesions were included in this study. Out of these, forty were histologically proven benign lesions and forty were diagnosed as breast malignancies.
Out of the forty benign cases studied, fibroadenomas constituted the largest group with 70% (28/40) of cases. Usual ductal hyperplasia comprised 10% (4/40) and intraductal papillomas 10% (4/40). Fibrocystic disease and sclerosing adenosis each constituted 5% (2/40) of cases. Whereas amongst forty malignant cases, majority of the cases were of invasive ductal carcinoma, not otherwise specified (NOS) constituting 82.5% (33/40) of the cases. 10% (4/40) of the cases were of invasive papillary carcinoma and invasive lobular carcinoma comprised of 7.5% (3/40) of all cases. Out of the 40 malignant cases, 10 were further classified as grade 3 carcinoma (poorly differentiated), 12 as grade 2 (moderately differentiated) and 18 cases as grade 1 carcinomas (well differentiated) on the basis of modified Bloom Richardson system.
The mean age for the benign group was 37.23 years (age range 25-60 yrs) and for the malignant group was 60.53 years (age range 35-80 yrs). All 80 cases taken in this study are of female sex (100%).
Immunohistochemistry was applied on all the eighty cases using P Cadherin antibody and its expression was evaluated. Pattern of staining was predominantly brown membranous staining with few areas showing both membranous and cytoplasmic positivity. Its differential expression in benign and primary malignant tumors was also analysed using scoring.
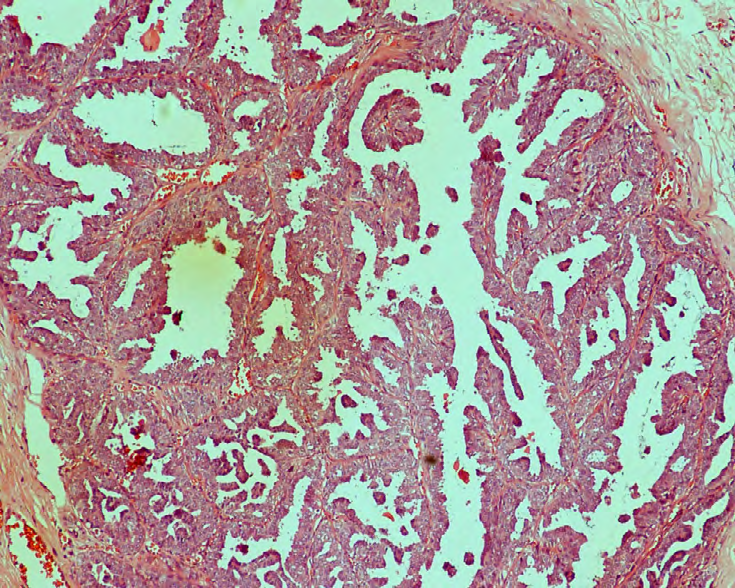
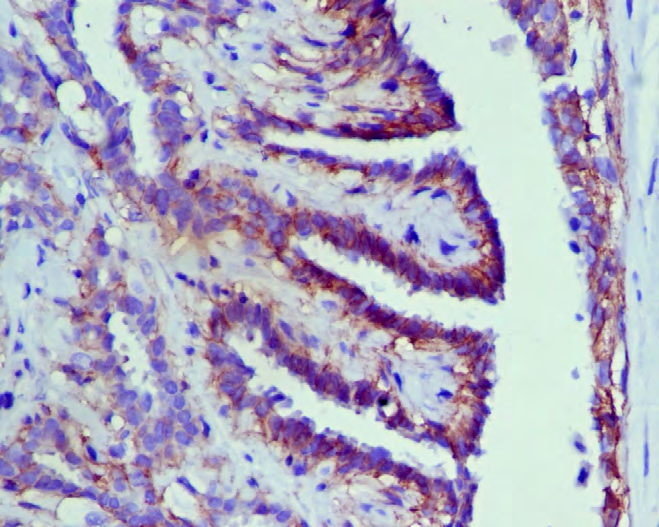
Out of the 40 benign cases studied all showed positive staining with P Cadherin (100%). Of 28 fibroadenoma cases, 57.1% (16/28) had a total score ranging between 4-6 and 42.8% (12/28) had a total score between 7-9 (Figures 1 & 2).
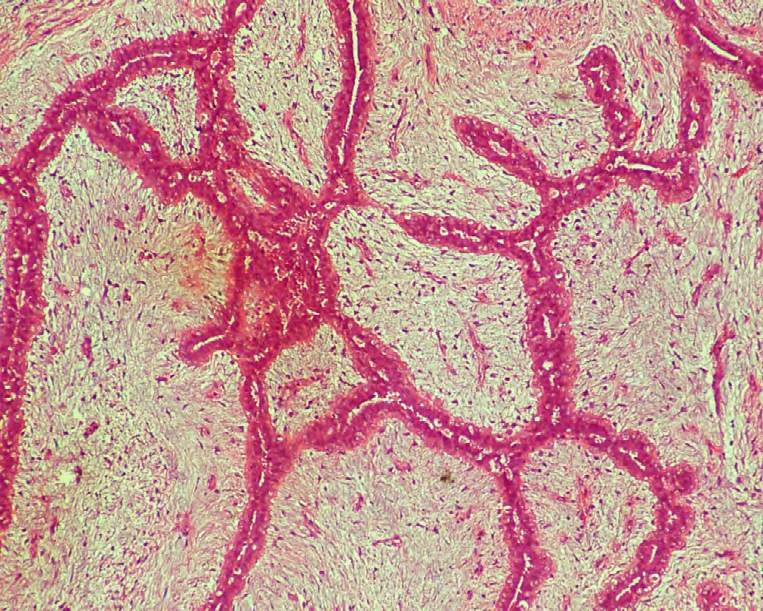
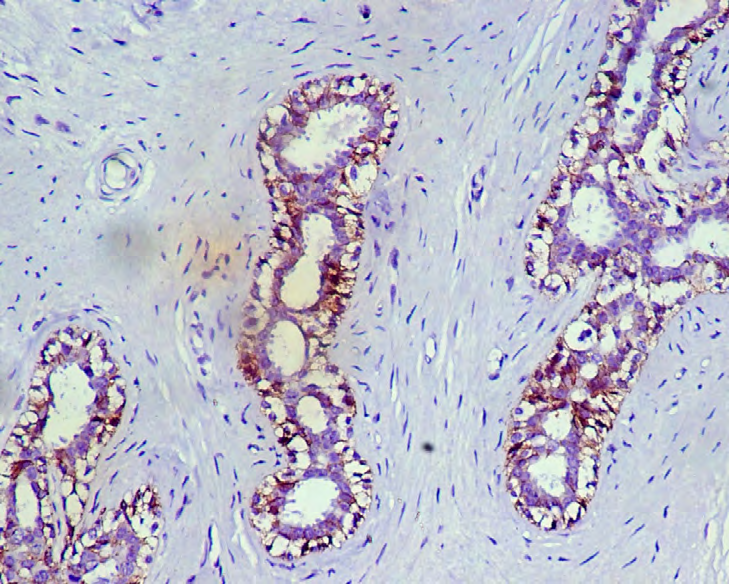
Out of 4 cases of intaductal papilloma, 100% (4/4) showed a total score between 4-6 (Figures 3 & 4).
Of 4 cases of usual ductal hyperplasia, 75% (3/4) showed a total score between 4-6 and 25% (1/4) cases had a total score between 7-9. All the cases of sclerosing adenosis (2/2) had a total score between 4-6 (Figures 5 & 6).
In fibrocystic disease 50% (1/1) had score between 4-6 and 50% (1/1) had score between 7-9 (Table 1).
| LESION | NO | TS 0 | TS 1-3 | TS 4-6 | TS 7-9 |
|---|---|---|---|---|---|
| Fibroadenoma | 28 | 0 | 0 | 16 | 12 |
| Intraductal Papilloma | 4 | 0 | 0 | 4 | 0 |
| Usual Ductal Hyperplasia | 4 | 0 | 0 | 3 | 1 |
| Fibrocystic Disease | 2 | 0 | 0 | 1 | 1 |
| Sclerosing Adenosis | 2 | 0 | 0 | 2 | 0 |
| Total | 40 | 0 | 0 | 26 | 14 |
| Percentage (%) | 100 | 0 | 0 | 65 | 35 |
Table 1: P Cadherin Staining In Benign Breast Lesions.
Out of a total of 40 benign cases, 100% cases showed positive staining with P Cadherin. No case showed negative result. The staining index of majority of the cases (65%) was between 4 and 6. The group with staining index between 7 and 9 comprised 35% of the cases.
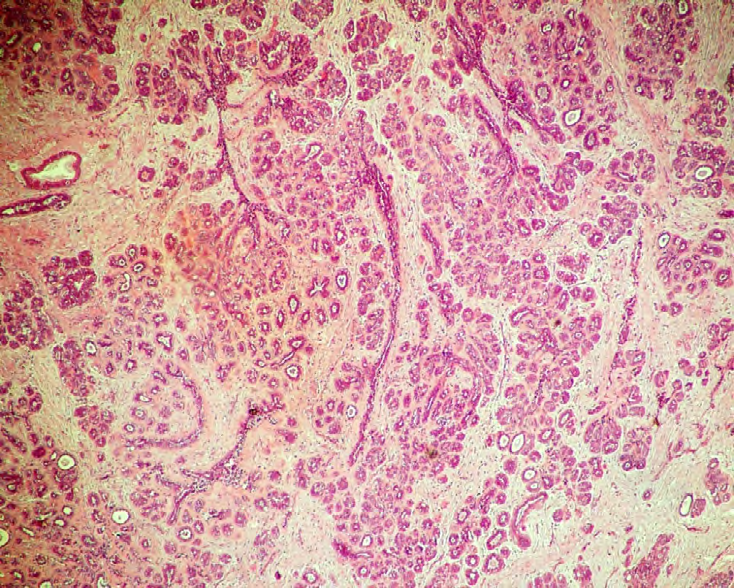
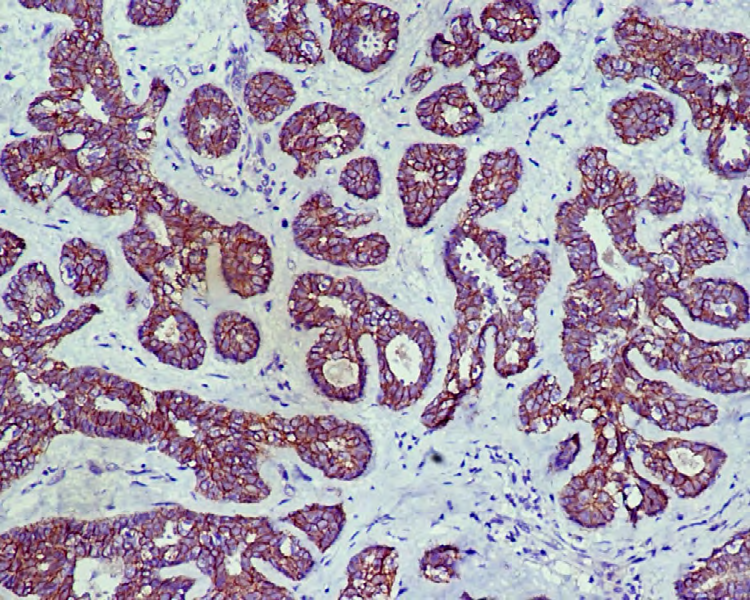
Whereas for 40 malignant cases studied, 24 cases (60%) showed no staining. The staining index for them was zero. 7 cases (17.5%) showed staining index between1-3 (Figures 7-9).
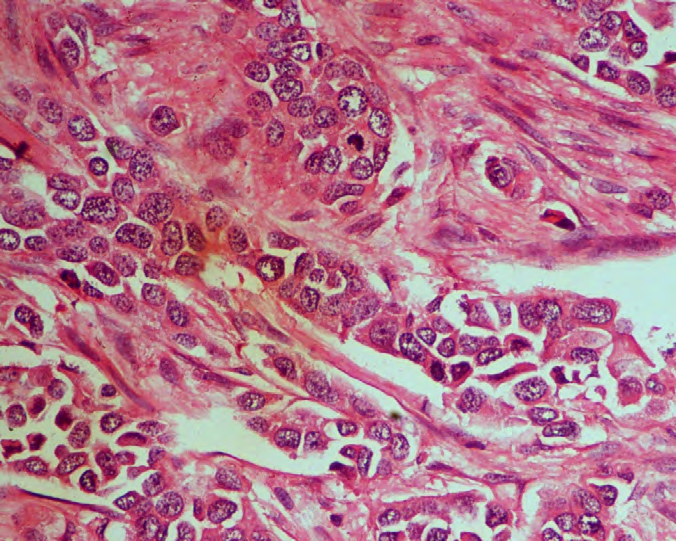
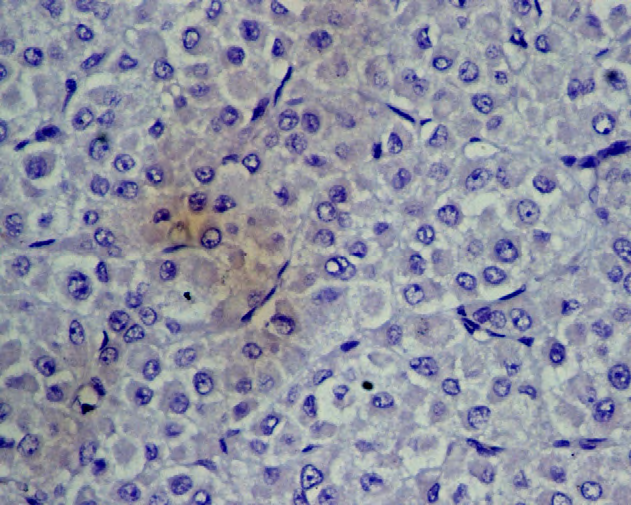
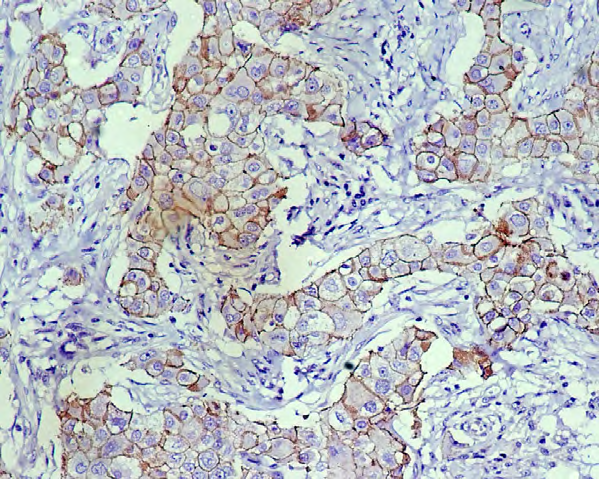
These cases included 6 cases of invasive ductal carcinoma and 1 case of invasive lobular carcinoma. 22.5% (9/40) of the total cases showed a positive staining with a staining index between 4-6. All these cases were of invasive ductal carcinoma NOS. Staining index between 7-9 was not seen in any of the case. Thus, 67.5% of the malignant cases were negative for P Cadherin and 22.5% of the cases were positive (Table 2).
| Lesion | NO | TS 0 | TS 1-3 | TS 4-6 | TS 7-9 |
|---|---|---|---|---|---|
| Invasive Ductal Carcinoma,Nos | 33 | 18 | 6 | 9 | 0 |
| Invasive Papillary Carcinoma | 4 | 4 | 0 | 0 | 0 |
| Invasive Lobular Carcinoma | 3 | 2 | 1 | 0 | 0 |
| Total | 40 | 24 | 7 | 9 | 0 |
| Percentage (%) | 100 | 60 | 17.5 | 22.5 | 0 |
Table 2: P Cadherin Staining In Malignant Breast Lesions. Out of the 9 malignant cases which were positive for P-cadherin, 6 were
A comparison of P cadherin positivity (evaluated by total scores) was done between all benign and malignant cases (Table 3).
| Lesion | Positive Staining | Negative Staining | Total | P Value |
|---|---|---|---|---|
| Benign (No.) | 40 | 0 | 40 | <0.0001 |
| Percentage (%) | 100 | 0 | ||
| Malignant (No.) | 9 | 31 | 40 | |
| Percentage (%) | 22.5 | 77.5 | ||
| Total | 49 | 31 | 80 |
Table 3: Comparison between Results of P Cadherin Immunostaining in Benign and Malignant Lesions.
Chi square test was applied to the results of P-cadherin expression to perform statistical analysis. The p value was found to be < 0.0001. Thus the association between the type of lesion of the breast and result of IHC staining is considered to be statistically significant.
The results show that P-cadherin can be used as a reliable marker for the identification of myoepithelial cells in breast tissue and can thus help in differentiating benign lesions of the breast from invasive carcinomas.
Discussion
According to GLOBOCON 2018, breast cancer is the second most common cancer in the world and, by far, now the most common cancer in women in India. Both, the incidence, as well as deaths, due to breast cancer is more than cervical cancer [7].
Although breast cancer has characteristic histological features, but it is often difficult to distinguish it from some of the benign lesions like fat necrosis, radial scar, complex sclerosing lesion, granular cell tumor, fibromatosis, myofibroblastoma, pseudo-angiomatous stromal hyperplasia and other stromal cell lesions. Therefore, it becomes imperative to recognize benign lesions, both to distinguish them from in situ and invasive breast cancer and to assess a patient’s risk of developing breast cancer, so that the most appropriate treatment modality for each case can be established [8]. It is postulated and generally accepted that primary breast carcinomas show a dramatic increase in the ratio of luminal-to-myoepithelial cells, and that many invasive breast carcinomas essentially lack myoepithelial cells entirely [9].
The majority of breast cancer studies have focused on luminal cells, because these are known to be the source of most carcinomas of the breast. However, progression to carcinoma involves alteration of the entire organized structure of the breast; depending on tumor grade, the changes can include the loss of apicobasal polarity, collapse of the glandular structure, disappearance of normal myoepithelial cells and disruption of the Basement Membrane (BM) at the epithelial– stromal junction [10].
The mechanisms responsible for the loss of the myoepithelial layer and BM in invasive cancer are unknown. Man and Sang proposed that loss of myoepithelial cells in cancer is due to localized death of these cells; however, this is not proven, and the potential factors responsible for selective cell death are not known [11]. Barsky and coworkers were the first to use functional assays to show that myoepithelial cells exhibit many antitumorigenic properties, such as the ability to inhibit tumor cell invasion and angiogenesis. Subsequent studies revealed that myoepithelial conditioned media inhibited the growth of breast cancer cell lines and induced a G2/M cell cycle arrest [12].
P-cadherin is a highly sensitive marker for myoepithelial cells, with exceptions in few cases of benign and malignant proliferations. The distinct staining of myoepithelial cells for P-cadherin and the lack of staining for myofibroblasts, when differentiating between a radial scar and a tubular carcinoma, show its advantage over smooth muscle actin. Thus, P-cadherin should be considered as a helpful tool in the differential diagnosis of breast lesions and borderline malignant tumors [13].
For the tubular carcinomas there is a clear discrimination between normal glands and neoplastic tubular structures for P-cadherin, with staining of myoepithelial cells in the normal glands, but no staining around the neoplastic structures. When differentiating between a radial scar and a tubular carcinoma, the distinct staining of myoepithelial cells for P-cadherin and the lack of myofibroblast reactivity make it preferable to smooth muscle actin.
Jones and coworkers showed that myoepithelial cells inhibit invasion through downregulation of MMP expression by tumor cells and fibroblasts. These data suggest that normal myoepithelial cells inhibit tumor cell function through a combined suppression of tumor cell growth, invasion, and angiogenesis [13].
In this study, P-cadherin expression was analyzed in all benign and malignant cases separately and then its differential expression was compared in between the two groups. The difference in the expression of P-cadherin was found to be statistically significant between the benign and malignant cases (p value < 0.0001). Also the malignant cases were divided into different histological grades according to their morphological features and differential expression of P-cadherin was observed in different grades.
In our study the mean age at presentation for the benign group was 37.23 years (age range 25-60 yrs) and for breast carcinoma was 60.53 years (age range 35-80 yrs). Our results were in concordance with the literature. Out of the forty benign cases, fibroadenoma was the most common benign breast lesion encountered. It constituted the maximum number of cases making upto 70% of the total. Our finding was in agreement with most of the available literature on benign breast lumps, where the frequency of fibroadenoma ranged from 46.6%-65.6%. Out of the forty malignant cases, invasive ductal carcinoma not otherwise specified was the most common malignancy encountered comprising of 82.5% of all the cases. These results were in accordance with the literature [14, 15, 16].
We observed, all the forty benign cases showed positive staining with P cadherin that is P Cadherin was identified in all the myoepithelial cells of all the breast tissues studied, with no difference between ducts and lobules and with overall strong staining. In these forty cases, 65% of them had a total score between 4-6 and in the remaining 35% it was between 7-9. Most of cases showed membranous staining in more than 50% of tissue section (3+). In few cases both membranous and cytoplasmic staining was seen. Our results were in concordance with a similar study by Yachika Bhatia [17], in which, P Cadherin expression was studied in 25 benign cases. All the 25 cases were positive for immunostaining with P Cadherin. Similar findings were reported by Palacios, et al. in 2002 [18]. The absence of E-cadherin membranous staining is characteristic of invasive lobular carcinoma. Pleomorphic lobular carcinoma were frequently ER- and PR- positive, E-cadherin-negative [19].
A study conducted in 2003 by Kovacs and Walker also assessed the value of P cadherin as myoepithelial marker in differential diagnosis of benign and malignant lesions of breast [19]. All MECs in normal breast ducts, ductules and lobules and sclerotic lesions showed strong staining for P cadherin. P cadherin was detected in the MECs of ducts and lobules of all ten samples from reduction mammoplasties. There was difference in reactivity between large and small ducts or lobules.
Gama et al studied expression of P cadherin in mammary tissue to analyze the possible role of P cadherin in mammary tissue. Its expression was examined in 13 samples of normal (n=2) and hyperplastic (n=11) mammary tissues. In normal and hyperplastic mammary gland, P cadherin was restricted to MECs, usually at the sites of cell to cell contact [20].
None of the benign cases in our study had a score less than or equal to 3. These results were also in concordance with the work by Yachika Bhatia in 2013. Thus our study shows that P cadherin is a reliable marker for staining MECs as reflected by its 100% positivity in all the benign lesions in which an intact myoepithelial layer was present. Moreover it does not stain myofibroblasts, thus showing an advantage over other myoepithelial markers like SMA.
We analysed P cadherin expression on 40 cases of breast malignancies. 33 cases were contributed by IDC- NOS occupying the major share of 83%. Out of these 33
cases, 10 were classified as grade 3 (poorly differentiated) malignancies based on the modified Bloom and Richardson system. Rest 17% was contributed by invasive papillary carcinoma (4/40) and invasive lobular carcinoma (3/40) forming 10% and 7% respectively. In the present study, out of the total cases, 60% (24/40) cases showed no staining with P cadherin. Their total score was zero. 17.5% (7/40) cases showed total score between 1 and 3 (taken as negative). The remaining 22.5% (9/40) cases showed positive staining (total score between 4 and 6). None of the case had a score between 7 and 9.
Thus in our study, 77.5% (31/40) cases had negative results and 22.5% (9/40) cases were immunopositive for P cadherin. All the positive 9 cases belonged to IDC-NOS. All 4 cases of invasive papillary carcinoma showed zero staining. Out of 3 cases of invasive lobular carcinoma, all showed negative results for P cadherin with one case having score between 1 and 3 and two cases with zero score. The results of this study were in concordance with the work by Yashika Bhatia, et al. Similar findings have been reported by Palacios et al in 2002 [18].
Pleomorphic lobular carcinomas (PLC) of the breast display histological features associated with classic invasive lobular carcinoma (ILC), yet they also exhibit more conspicuous nuclear atypia and pleomorphism, and an aggressive clinical behaviour. From a breast cancer progression perspective, it is unclear whether PLC is a variant of ILC or is a high-grade invasive ductal carcinoma (IDC) that has lost E-cadherin. The molecular features of 26 PLC were studied using immunohistochemistry [oestrogen receptor (ER), progesterone receptor (PR), HER2, p53 and E-cadherin], 0.9 Mb resolution, microarray-based comparative genomic hybridization (aCGH), fluorescent (FISH) and chromogenic (CISH) in situ hybridization and loss of heterozygosity. Comparative analysis was performed with aCGH data from PLC with classic ILC (16 cases) and high grade IDC (35 cases). PLCs were frequently ER- and PR-positive, E-cadherin-negative and occasionally HER2- and p53- positive. Recurrent copy number changes identified by aCGH included gains on 1q, 8q, 11q, 12q, 16p and 17q and losses on 8p, 11q, 13q, 16q and Xq. Highly recurrent 1q+ (100% of cases), 16p+ (93%), 11q- (53%) and 16q- (93%) and evidence of the der(1;16)/der(16)t(1;16) rearrangement, as detected by FISH, suggested that PLC had a ‘lobular genotype’. Focal amplifications were evident at 8p12-p11, 8q24, 11q13.1-q14.1, 12q14, 17q12 and 20q13. Loss of BRCA2 was detected in 40% of PLC by LOH. Comparative analysis of aCGH data suggested the molecular features of PLC (ER/ PR-positive, E-cadherin-negative, 1q+, 11q (-), 16p+ and 16q (-)) were more closely related to those of ILC than IDC, implicating an overlapping developmental pathway for these lobular tumour types. Molecular alterations found in PLC that are more typical of high-grade IDC than ILC (p53 and HER2 positivity, 8q+, 17q24-q25+, 13q(-) and amplification of 8q24, 12q14, 17q12 and 20q13) are likely to drive the high-grade and more aggressive biology of PLC [20].
In a work by G Turashvili et al in 2011, a tissue microarray was constructed from 3992 cases of invasive breast carcinoma, and P-cadherin expression was evaluated using immunohistochemistry [21]. Out of 3710 interpretable cases on the tissue microarrays, P-cadherin was positive (50% cut point) in 1290 patients (34.8%). They also found that P-cadherin expression differed according to the histological type of breast cancer. Invasive ductal carcinoma cases showed P-cadherin-positive rates equal to the overall P-cadherin-positive rate [35.5% (1195/3364) in the whole series]; invasive lobular carcinoma showed lower P-cadherin-positive rates [16.2% (45/ 278) in the whole series]. The positivity of P cadherin in breast malignancies in this study was higher than seen in our study. There are some other studies that have analysed the expression of P cadherin in breast carcinoma. In an early study by Rasbridge, et al in 1993, P-cadherin was not detected in patients with ductal carcinoma [22]. In contrast, a later study found P-cadherin in some cases of infiltrating ductal carcinoma (20%), where it was associated with reduced E cadherin and advanced histological grade [18]. These results are in concordance with the results of our study.
In the present study it was observed that out of the 10 cases grade 3 invasive carcinomas, 6 cases (60%) were immunopositive for P cadherin and had total score between 4 and 6. Remaining 4 cases (40%) were negative and showed score between 1 and 3. However, no statistical analysis was done between the grade of tumor and P cadherin positivity in our study.
Similar observations were also seen by G Turshavili, et al (2011). They found that both the percentage of P cadherin-positive cells and P cadherin staining intensity were positively associated with histological grade, and negatively associated with age at diagnosis [21]. They also showed that P cadherin positivity is associated with high- grade tumor subtypes (HER2+ and basal carcinomas), and well-established markers of poor prognosis (ER, PR, Bcl-2).
In 2005, Arnes et al undertook a detailed evaluation of the relationship between P-cadherin, prognostic markers in breast cancer, and outcome [23, 24, 25]. P cadherin was present in 31% of breast cancers cases and was more frequent in tumors with a basal epithelial phenotype (p < 0.001).
Conclusion
In this study it was shown that all the benign cases (100%) were immunopositive for P-cadherin. The myoepithelial cells were highlighted in all these cases by P-cadherin. There was no reactivity of P-cadherin with myofibroblasts giving an advantage over few other myoepithelial markers like SMA. In the malignant group, 77.5% cases were immunonegative with P-cadherin. Only 22.5% cases showed positivity. The difference between the results in these two groups was statistically significant with p value < 0.0001. Thus, this study shows that P-cadherin is a highly sensitive marker for myoepithelial cells. Its expression strongly correlates with the type of breast lesion, which can help in differentiation between benign and malignant lesions whenever there is confusion in diagnosis with routine methods.
References
-
Paredes J, Correia AL, Ribeiro AS, Albergaria A, Milanezi F, et al. (2007) P-cadherin expression in breast cancer: A review. Breast Cancer Res 9(5): 214.
-
Yilmaz M, Christofori G (2010) Mechanisms of motility in metastasizing cells. Mol Cancer Res 8(5): 629-642.
-
Suyama K, Shapiro I, Guttman M, Hazan RB (2002) A signaling pathway leading to metastasis is controlled by N-cadherin and the FGF receptor. Cancer Cell 2(4): 301- 314.
-
Lo Muzio L, Campisi G, Farina A, Rubini C, Pannone G, et al. (2005) P-cadherin expression and survival rate in oral squamous cell carcinoma: An immunohistochemical study. BMC Cancer 5: 63.
-
Adriance MC, Inman JL, Petersen OW, Bissell MJ (2005) Myoepithelial cells: Good fences make good neighbors. Breast Cancer Res 7(5): 190-197.
-
Choi H, Puvenna V, Brennan C, Mahmoud S, Wang XF, et al. (2016) S100B and S100B auto-antibody as biomarkers for early detection of brain metastases in lung cancer. Transl Lung Cancer Res 5(4): 413-419.
-
(2018) Cancer Statistics: India versus The World, Globocan.
-
Guray Merih, Sahin AA (2006) Benign breast dieases: Classification, Diagnosis and Management. The Oncologist 11(5): 435-449.
-
Rudland PS (1987) Stem cells and the development of mammary cancers in experimental rats and in humans. Cancer Metastasis Rev 6(1): 55-83.
-
Ronnov-Jessen L, Petersen OW, Bissell MJ (1996) Cellular changes involved in conversion of normal to malignant breast: importance of the stromal reaction. Physiol Rev 76(1): 69-125.
-
Man YG, Sang QX (2004) The significance of focal myoepithelial cell layer disruptions in human breast tumor invasion: a paradigm shift from the ‘protease- centered’ hypothesis. Exp Cell Res 301(2): 103-118.
-
Sternlicht MD, Safarians S, Rivera SP, Barsky SH (1996) Characterizations of the extracellular matrix and proteinase inhibitor content of human myoepithelial tumors. Lab Invest 74(4): 781-796.
-
Jones JL, Shaw JA, Pringle JH, Walker R (2003) Primary breast myoepithelial cells exert an invasion-suppressor effect on breast cancer cells via paracrine down- regulation of MMP expression in fibroblasts and tumour cells. J Pathol 201(4): 562-572.
-
Carey LA, Perou CM, Livasy CA, Dressler LG, Cowan D, et al. (2006) Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. JAMA 295(21): 2492- 502.
-
Kim MJ, Ro JY, Ahn SH, Kim HH, Kim SB, et al. (2006) Clinicopathologic significance of the basal-like subtype of breast cancer: a comparison with hormone receptor and Her2/neu-overexpressing phenotypes. Hum Pathol 37(9): 1217-1226.
-
Rakha EA, Putti TC, Abd El-Rehim DM, Paish C, Green AR, et al. (2006) Morphological and immunophenotypic analysis of breast carcinomas with basal and myoepithelial differentiation. J Pathol 208(4): 495-506.
-
Bhatia Y (2013) P-cadherin as myoepithelial cell marker for differential diagnosis of benign and malignant breast lesions. Indian J Pathol Microbiol 56(1): 6-9.
-
Palacios J, Benito N, Pizzaro A, Suavez A, Espada J, et al. (1995) Anomalous expression of P Cadherin in breast carcinoma. Am J Pathol 146(3): 605-612.
-
Jagtap SV, Beniwal A, Chougule PG, Shah HP, Jagtapet SS (2016) Invasive lobular carcinoma of breast histopathological subtypes: clinicopathological study. Int J Health Sci Res 6(7):105-111.
-
Simpson PT, Reis-Filho JS, Lambros MB, Jones C, Steele D, et al. (2008) Molecular profiling pleomorphic lobular carcinomas of the breast: evidence for a common molecular genetic pathway with classic lobular carcinomas. J Pathol 215(3): 231-244.
-
Kovacs A, Walker RA (2003) P Cadherin as a marker in the differential diagnosis of breast lesions. J Clin Pathol 56(2): 139-141.
-
Gama A, Paredes J, Albergaria A, Gartner F, Schmitt F (2004) P-cadherin expression in canine mammary tissues. J Comp Pathol 130(1): 13-20.
-
G Turashvili, McKinney SC, Goktepe O, Leung SC, Huntsman DG, et al. (2011) P cadherin expression as aprognostic biomarker in a 3992 case tissue microarray series of breast cancer. Mod Pathology 24(1): 64-81.
-
Rasbridge SA, Gillett CE, Sampson SA, Walsh FS, Millis RR (1993) Epithelial (E-) and placental (P-) cadherin cell adhesion molecule expression in breast carcinoma. JPathol 169(2): 245-250.
-
Arnes JB, Brunet JS, Stefansson I, Bégin LR, Wong N, et al. (2005) Placental cadherin and the basal epithelial phenotype of BRCA1-related breast cancer. Clin Cancer Res 11(11): 4003-4011.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet