Determining the True Incidence of Transfusion Reactions in Transfusion Recepients by Active Hemovigilance by Transfusion Medicine Personnel: An Indian Study
Purpose: Hemovigilance is the systematic surveillance of transfusion reactions (TRs). The aim of this study is to evaluate the effectiveness of active, bed side surveillance OR active HV done by transfusion medicine (TM) personnel over reporting directed by clinicians, calculate true incidence of TRs. Methods: This study consisted of prospective cross sectional and retrospective analysis arms. The study was conducted in a tertiary care hospital, Northern India. In the retrospective analysis arm, the data was archived for the period spanning from 01-07-15 to 30-06-19, which provided historical pertinent data. The prospective analysis was done for the duration of six months from July 2019 to December 2019. In prospective analysis group was divided into two a.) TRs reported by clinicians (passively) and b.) TRs diagnosed by active HV in which the recipients were assessed and followed bed side for 24 hours vide a post transfusion questionnaire by TM residents. All the recipients of allogenic transfusions were included. Results and Conclusions: The incidence of the TRs in prospective analysis was 0.54%., out of which only 0.24% were reported by clinicians and rest 0.30% were reported by active HV. While in retrospective arm, the incidence of TRs was 0.20% only. On comparison of prospective and retrospective data, TRs reported during prospective analysis were statistically significantly higher, (p <0.05). On comparison of various studies, it is concluded that Active HV for assessment of TRs can make significant differences in the reporting. Febrile Non- Haemolytic Transfusion Reaction was the most commonly reported TR.
Introduction
Hemovigilance (HV) is defined as the systematic surveillance of transfusion-related adverse events (AE) and adverse reactions (AR). HV system is an integral part of quality management in transfusion medicine (TM). HV is essential for the improvement of the quality and safety of blood and blood products, it encompasses all the activities of the blood transfusion chain, i.e., from blood donation till the blood/ component is transfused and extends in post transfusion phase [1]. HV was initiated in France in 1993 with obligatory reporting and in United Kingdom (UK) voluntary reporting system in 1996. However, HV programme (HvP) in India was incepted in December 2012 as part of pharmacovigilance programme [2, 3].
It is estimated that up to 10% of the transfusions are associated with the AE [4, 5]. One of the main goals of developing HvP is to improve Blood Transfusion practices by appropriate and timely reporting of TRs. The HvP relies on the reporting of TRs by the clinicians to the Department of TM which is ultimately updated to national HV networks [2, 5]. However, the published national and international studies state that TRs like Transfusion Associated Circulatory Overload (TACO), Transfusion Associated Lung Injury (TRALI) and Delayed Haemolytic Transfusion Reaction (DHTR) are often and missed under reported [5, 6, 7, 8]. In the light of international and national studies, we conducted a study to determine the true incidence of TRs by active bed side surveillance by transfusion medicine personnel and compare it with the retrospective data of clinician directed cases.
Material and Methods
This is a cross sectional study conducted in the department of TM at a tertiary care centre in Jodhpur, Rajasthan, India for which the ethical clearance was obtained.
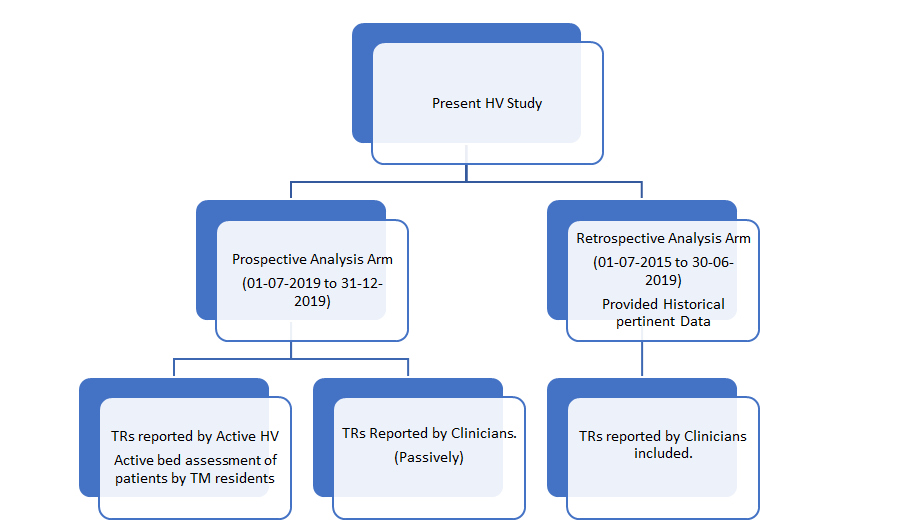
The study was divided into prospective and retrospective arms. The retrospective arm included TRs reported only by clinicians, whereas in the prospective arm TRs were reported both by clinicians and by active follow up of the transfusion episodes by TM residents within 24 hrs post transfusion. The incidence of TRs in retrospective analysis arm was determined for the period of four years from mid of 2015 to 2019. The prospective analysis was carried out for six months duration from July 2019 to December 2019.
- Inclusion Criteria: All the allogenic transfusions were included.
- Exclusion Criteria: The transfusions during plasma exchange were excluded because it can introduce procedure related reactions which can confound the interpretation.
- Prospective analysis group: included proactive evaluation by TM residents followed by final adjudication of TR by TM specialists to ascertain the incidence of TRs by active surveillance over and above the routine reporting of TRs by clinicians.
Hence, the prospective study was divided into two groups namely
- TRs reported by clinicians (Passively).
- TRs reported by Active HV (by TM residents).
The prospective analysis was observational study hence patient consent was not taken, but hospital transfusion policy and nursing protocols were followed as laid down. During the study period, the transfused patients were assessed bed side with regards to post transfusion clinical parameters to rule out OR establish TR vide post transfusion questionnaire to be used by TM residents, enclosed as Appendix 1.
The active bed side evaluation of the transfused patient by TM residents included collecting data related to patient demographics, diagnosis, indications of transfusion, drug history, h/o previous and multiple transfusions, component- related data (type and number of components,), pre- transfusion and post-transfusion vitals (blood pressure, heart rate, respiratory rate, oxygen saturation) laboratory parameters (blood grouping, direct Coomb’s test, indirect Coomb’s test, pre and post complete blood count, pre and post renal function test, pre and post liver function test), radiology reports (pre and post Chest X-ray) and clinical records were recorded. The immediate care givers were interviewed and clinicians too if required.
Namely, the following evaluation tools were used (Figure 1)
- Post transfusion questionnaire enclosed in the Appendix no. 1 of the study to be used by TM residents.
- Transfusion monitoring forms filled by clinical residents and paramedical staff available in-patient records.
- Compatibility cum reaction forms returned back to blood bank within 24 hours by clinicians.
The final adjudication of TR was performed by TM specialist as per institutional protocols and International Society of Blood Transfusion (ISBT) definitions. The review period was 24 hours but in cases suspicious of DHTR like inadequate increase in post transfusion haemoglobin, increase in LDH etc. These patients were followed up for seven days post transfusion.
TRs were defined and classified for Imputability & severity (association of TR with BT) according to the guidelines provided by the International Society of Blood Transfusion working party on HV (ISBT) as detailed below [9]:
Severity
- Grade 1 (Non-Severe): The recipient may have required medical intervention (e.g. symptomatic treatment) but lack of such would not result in permanent damage or impairment of a body function.
- Grade 2 (Severe): The recipient required in-patient hospitalization or prolongation of hospitalization directly attributable to the event; and/or the adverse event resulted in persistent or significant disability or incapacity, or the adverse event necessitated medical or surgical intervention to preclude permanent damage or impairment of a body function.
- Grade 3 (Life-threatening): The recipient required major intervention following the transfusion (vasopressors, intubation, transfer to intensive care) to prevent death.
- Grade 4 (Death): The recipient died following an adverse transfusion reaction.
Imputability
This is, once the investigation of the TR is completed, the assessment of the strength of relation to the transfusion of the ATE.
- Definite (certain): When there is conclusive evidence beyond reasonable doubt that the AE can be attributed to the transfusion.
- Probable (likely): When the evidence is clearly in favor of attributing the AE to the transfusion. Possible: when the evidence is indeterminate for attributing the AE to the Transfusion/an alternate cause.
- Unlikely (doubtful): When the evidence is clearly in favor of attributing the AE to causes other than the transfusion.
- Excluded: When there is conclusive evidence beyond reasonable doubt that the AE can be attributed to causes other than the transfusion.
The prospective analysis- divided into two groups. • TRs reported by the clinicians (passively): This group included consultation by clinicians regarding TRs wherein final adjudication and imputability assessment was done by TM specialist.
• TRs by Active HV (by TM residents): This group included comprehensive review of the transfused patients within 24 hours post transfusion to detect cases suspicious of TRs by TM residents as mentioned earlier.
Retrospective analysis
Review of available records of patients to ascertain the incidence of TRs reported by clinicians i.e., passive reporting. The retrospective analysis of our electronic clinical records, HvP data, hard copy of blood transfusion reaction register, monthly statistics available was conducted to determine our institution’s historical rate of TRs based on passive reporting by clinicians over the period of July 2015 to June 2019.
Statistics
The prospective analysis data was entered into Microsoft Excel spread sheet. The data was analysed and expressed as either descriptive statistical parameters like mean with standard deviation, median and range or as absolute numbers and percentages for categorical variables. The incidence was calculated as the percentage of total number of TRs divided by the total number of blood components transfused and also incidence was calculated for each category of components. Transfusion Episodes were not taken to calculate the incidence as done in few studies as it over estimates the incidence. Statistical comparison was made with the incidence reported in the past four years using Chi-square test as the retrospective data of TRs was available in the institution. This study was also compared with the past studies published in the indexed medical journals form India to avoid population bias.
Results
Retrospective Analysis
(Table 1) The total of 32 TR episodes were reported from July 2015 to June 2019, with the age range of the affected patients between 5 months to 75 years, with mean age of 36.31 years. Out of 32 TR episodes, 18(56.25%) were in males and 14 (43.75%) were in females. On deeper analysis of TR episodes, 21 cases (65.62%) were due to Packed red blood cell concentrates (PRBC) transfusion with the incidence of 0.31%, 4 cases (12.50%) were due to Fresh frozen plasma (FFP) transfusion with incidence of 0.08%, 4 cases (12.50%) were due to Random donor platelet concentrates (RDPC) transfusion with incidence of 0.14%, 3 cases (9.37%) were due to Single Donor platelet concentrate (SDPC) transfusion with incidence of 1.85%.
| Type of blood component | PRBC (Packed red blood cell concentrates) | FFP (Fresh frozen plasma) | RDPC (Random donor platelet concentrate) | SDPC (Single Donor platelet concentrate) | CRYO (Cryoprecipitate) | CPP (Cryo poor Plasma) | Total |
|---|---|---|---|---|---|---|---|
| Number of TRs due to component | 21(65.62%) | 4(12.5%) | 4(12.5%) | 3(9.375%) | 0 | 0 | 32 |
| Incidence of TRs with each component | 0.31% | 0.08% | 0.14% | 1.85% | 0 | 0 | 0.20% |
| Number of Components Issued | 6,787 | 5,207 | 2920 | 162 | 162 | 162 | 15,600 |
Table 1: TR Data in Retrospective Analysis.
TR Data in Prospective Analysis
Prospective analysis: The prospective analysis group was divided into two groups namely • Reported by clinicians (passively).
• Reported by Active HV.
A total of 18 TR episodes were reported in 18 different patients, out of which 8 (44.4%) were reported passively, while 10 (55.5%) were reported by active HV. The age range of the affected patients was between 8 months to 79 years, with the mean of 36.8 years. The sex wise distribution is 6 patients (6/18, 33.33%) were males, 12 (12/18,66.67%) were females. Out of 18 TRs reported 15 cases (83.3%) were non severe in nature, rest 3 (16.66%) were severe in nature. Non-severe TRs were most common. Life threatening reactions or death were not reported in this study.
The overall incidence of TRs was 0.54%, out of which only 0.20% was reported by clinicians and 0.34% was reported by active HV (Table 2). In this prospective analysis, total of 3,277 blood components were transfused, of which 58.2% (1,907 units) were leucodepleted packed red blood cells (LD-PRBC), followed by RDPCs with 20.14% (660 units) of transfusions and others (as mentioned vide Table 2).
| TR Data in Prospective Analysis | |||||||
|---|---|---|---|---|---|---|---|
| Type of blood components | PRBC (Packed red blood cell concentrates) | FFP (Fresh frozen plasma) | RDPC (Random donor platelet concentrate) | SDPC (Single Donor platelet concentrate) | CRYO (Cryopreci pitate) | CPP (Cryo poor Plasma) | Total |
| Number of TRs due to component | 15(83.3%) | 1(5.5%) | 1(5.5%) | 1(5.5%) | 0 | 0 | 18 |
| Number of Components Issued | 1,907(58.2%) | 541(16.5%) | 660(20.14%) | 2(0.88%)9 | 130(3.97%) | 10(0.31%) | 3,277 |
| Incidence of TRs with each component | 0.78% | 0.18% | 0.15% | 0.88% | 0 | 0 | 0.54% (Passive Reporting /00.24% + active HV 00.30%) |
Table 2: TR Data in Prospective Analysis.
In this prospective analysis two cases of Delayed Hemolytic transfusion reaction (DHTR) were diagnosed out of total episodes of 18 TRs.
| DHTR cases | Age/Sex | Clinical diagnosis | Presentation of TR | Laboratory Investigations | Specialized Laboratory Investigations | Further Management |
|---|---|---|---|---|---|---|
| Ist case | 55Y/F | Myelodysplastic Syndrome with suspected Autoimmune Haemolytic Anaemia,H/o previous transfusions. | Inadequate increase in post transfusion Hb. 3.1 gm% to 2.9gm% (24-hour post transfusion Hb) | LDH:660U/ L,Reticulocyte Count:5.52%,Total/ Direct/Indirect Bilirubin: 2.2/0.59/1.62 mg/dl. | DCT:2+,ICT: 3+,Antibody screening: Positive.Antibody Identification: Kell, Kidd (JKa), N. | Transfusion withphenotypically selected ABO compatible units negative for anti- Jka (Kidd), N & Kell antigens. |
| 2nd Case | 43Y/F | People Living with Human Immunodeficiency VirusWith fever, pancytopenia, with Gram positive bacilli positive.H/o previous transfusions. | Hemoglobinuria, Hematuria,Inade quate increase in post transfusion Hb after two PRBC transfusions. 2.8gm/dl to 3.8gm/dl | LDH: 440 U/ LReticulocyte Count: 4.0%,Nucleated Red Blood Cell count:Total/ Direct/Indirect Bilirubin:1.9/0.40/1.50 mg/dl.Peripheral Smear: evidence of spherocytosis. | DCT 2+ with mixed field reaction.Antibody ScreeningPositive. Antibody identification: Anti Kell Antibody,RBC phenotyping:Kell antigen negative. | Transfusion with phenotypically selected ABO compatible units negative for Kell antigen. |
| S. No. | Age/Sex | Product | Type of Reaction | Type of Hemovigilance | Remarks | |
| 1 | 8Y/M | Cryoprecipitate | Allergic | P | • Multiply transfused Haemophilic patient. | |
| 2 | 8 month/F | PRBC | FNHTR | A | - | |
| 3 | 5Y/M | PRBC | FNHTR | P | - | |
| 4 | 20Y/F | PRBC | FNHTR | P | - | |
| 5 | 6Y/F | PRBC (LD) | Allergic | P | • Multiply transfused thalassaemic patient. | |
| 6 | 60Y/F | PRBC | FNHTR | P | - | |
| 7 | 79Y/F | PRBC | FNHTR | P | - | |
| 8 | 50Y/F | PRBC | FNHTR | A | - | |
| 9 | 30Y/F | PRBC (Irradiated) | FNHTR | A | • Multiply transfused patient of Aplastic Anemia, later treated with Anti thymocyte Globulin. | |
| 10 | 66Y/M | PRBC | Hypotensive Reaction | P | • On adjudication, the transfusion was classified as unlikely as patient was under General Anesthesia as anesthetic agents can have hypotensive effect. | |
| 11 | 74Y/M | PRBC | TACO | A | • Patient had co-morbidities like diffuse alveolar hemorrhage, coronary artery disease. | |
| • showed symptoms of hypoxemia, tachypnea, worsening dyspnea. | ||||||
| • B Lines in USG thorax | ||||||
| • ECG changes: Not significant. | ||||||
| • Fluid overload that responded to administration of diuretics. | ||||||
| • Mode of Oxygen therapy: Noninvasive ventilation. | ||||||
| 12 | 51Y/M | PRBC | Allergic | A | - | |
| 13 | 30Y/F | PRBC | FNHTR | A | • Multiply transfused patient of Aplastic Anemia, later treated with Anti thymocyte Globulin | |
| 14 | 25Y/F | PRBC | TAD (Transfusion Associated dyspnoea) | A | • Post neuro surgery patient who developed new onset dyspnea, tachypnoea within 12 hours of transfusion. | |
| • Patient had no other cause of dyspnea as evaluated by Chest X-ray and Blood Culture sensitivity to rule out sepsis. | ||||||
| 15 | 11Y/F | RDPC (irradiated) | Allergic | A | • Multiply transfused patient of Aplastic Anaemia. | |
| 16 | 23Y/M | FFP | Allergic | P | • Post-operative patient. | |
| • No significant H/o multiple transfusions. |
Table 3: The table describing the relevant clinical details of t DHTR cases followed up for seven days (Reported by Active HV).
The clinical details of the patients, characteristics of TRs (except DHTR), incriminating blood components etc. are mentioned comprehensively in (Table 4).
Table 4: Patient details in Prospective analysis except DHTR cases. Note: P stands for Passively reported/ reported by clinician, A stands for TRs reported by Active HV. A total of 18 TR episodes occurred during the study period, out of which PRBCs were responsible for the majority i.e., 15 cases; 83.3% of TRs identified (Table 2). On statistical analysis of incidence of TRs in Prospective and Retrospective analysis, p value was 000493, p<0.05, hence it is statistically significant. It is inferred that incidence of TRs in prospective analysis was significantly higher due to active HV. In this study, most common TR in active HV group was FNHTR (40%). Analysis of temporal association Or Imputability.
| Imputability | TRs (%) in overall prospective study group |
|---|---|
| Definite | 3/18 (16.67%) |
| Probable | 9/18(50.00%) |
| Possible | 5/18(27.78%) |
| Unlikely | 1(5.55%) |
| Excluded | 0 |
Table 4: Strength of Association of BT to TR.
The (Table 5) details the temporal association of the TRs in overall prospective study group. Out of four FNHTRs, three showed a temporal association with transfusion, where as in Agnihotri, et. al (Jan 2011- Dec2013) (6) Current Study (June 2019 to Dec 2019) Units transfused RBC used Leucoreduced using buffy coat method 4 log leuco Depleted leuco depleted Non- leucodepleted Non leuco depleted to leucodepleted Allo antibody screening done Yes Yes Yes No No HV Active feedback & bed side evaluation Active feedback Active feedback & bed side evaluation Passive reporting Passive reporting Number of TRs 18 (8 passive reporting+10 HV) 61 9 (2 passive reporting+7active HV) 105 196 TRs within 24 hours of transfusion (% of total reactions)
00.54% (Passive reporting00.24% active HV 00.30%); Retrospective arm: 0.2% p value was.000493, p<0.05 Incidence of TRs/unit transfused
0.32 one case it was a possible TR. The comparative study of HV based studies done in India is described in detail in (Table 6).
Bhattacharya P, et al. Chandigarh Study (July 2002-July 2003) (12)
Kumar P, et al. Delhi Study (Dec2007- April2012) (13)
Sahu, et al. (June 2018 to September 2018) (5)
3,277 in prospective arm, 15,660 in retrospective arm 18,914 500 56,503 3,80,658
16(88.89%) 61(100%) 9(100%) 102(97.1%) 195(99.5%)
1.8%(0.4% passive reporting+1.4%active HV)Note: TR incidence calculated with number of Transfusion Episodes.
0.19 P=0.0005 0.05 P<0.0001
Table No 6: Comparison of Transfusion Reactions Reported in Studies from India.
Discussion
On comparative analysis of TRs reported in studies from India, the study undertaken by Kumar P et al & Bhattacharya P et al found incidence of TRs to be 0.05% (196 out of 380,658) & 0.19% (105 out of 56,503). This can be explained as underestimation of the true incidence because of under reporting by routine clinician directed HV [12, 13] (Table 6).
HV is a standard tool to advance the quality of the BTS, primarily focusing on safety [3]. Sahu, et al. observed that the incidence of actual TRs was under reported due to several reasons as follows:
- Lack of awareness and proper knowledge among clinicians and paramedical staff.
- Temporal association with transfusion is often overlooked and particularly in cases of delayed TRs.
- Similarity between clinical presentation of TRs with other common clinical conditions is a possible reason for missed diagnosis.
- It is difficult to diagnose TRs in comatose or unconscious patients [5, 10].
The knowledge gaps related to transfusion among paramedical staff has been established in independent studies by Shivgunde, et al. and Sapkota A, et al. Hence, active involvement and training of paramedical staff in reporting of TRs will go a long way in improving the reporting rates, as they are in proximity with the patients [10, 11].
Somagari DR, et al. observed that the incidence of TRs was proportional to the number of the transfusion events [3]. As studied, earlier HvPs relied on passive reporting, national and international studies have shown that active reporting systems report higher rates of TRs than passive ones [2, 5, 6, 7, 8]. Most studies that have carried out active surveillance did it either by review of patients’ records, auditing of electronic hospital medical records, review of TR reporting forms or by active feedback forms developed during study [3, 6].
In the present study and the study done by Sahu A, et al. [5] and various international studies done by Gosmann F, et al. & Bernard RS, et al. prospectively followed all allogenic transfusions by using various methods like active bed side evaluation of the transfused patient by TM resident which included clinical, laboratory, radiological correlation. Narick C et al performed a prospective study with similar design of active HV to evaluate incidence of TACO after plasma transfusion within 24 hours [8]. Raval JS et al focused-on TACO after platelet transfusions with the similar study design [7].
In our study, FNHTRs constituted the most frequently reported TR in all three groups,
- Incidence of 53.12% in Retrospective analysis group.
- Incidence of 44.44 % in overall Prospective analysis group.
- Incidence of 40 % in group: Reported by active HV subgroup of Prospective analysis.
- This is comparable to the latest HvPI data, wherein FNHTRs constituted the most frequently reported TRs with the percentage of 40.84% [2].
(Table 6) The overall incidence of TRs in Prospective arm is 0.54%, out of which 0.34% reported by active HV and only 0.20% were passively reported/ reported by clinicians. On statistical analysis of incidence of TRs in Prospective & Retrospective data, p value was.000493, p<0.05, hence it is statistically significant. It proves the hypothesis that active HV is superior in diagnosis of TRs in comparison with passive reporting.
Hence, it can be concluded that adopting Active HV methodologies for assessment of TRs can make significant differences in the reporting. Therefore, standardisation of HV practices, training of all the para medical, medical staff to ensure uniformity and quality in reporting of TRs.
As per data available, it is observed that Non-severe TRs frequently remain un reported [16]. In the active HV group of the prospective analysis, FNHTRs, TACO, DHTR, TAD, allergic reactions were diagnosed by active surveillance, out of which DHTR, TACO can be severe, can have serious consequences for the patient. During the study, no anaphylactic, anaphylactoid or AHTRs, deaths were observed and the incidence of these entities was nil in both the arms. Delayed Haemolytic Transfusion Reactions (DHTRs). DHTRs is a potentially life- threatening complication of transfusion in multi transfused patients like, Sickle cell disease (SCD) patients. SCD patients are more likely to be alloimmunized than the general population due to discrepancies between the recipient’s and donors RBCs phenotype [17]. DHTRs are the outcome of immunological responses mounted by the recipient to the epitopes/ antigens present on the transfused blood cells. This response is delayed and manifested as accelerated destruction of transfused red blood cells (RBCs) [17].
Haemolytic Transfusion Reaction (HTR) is clinically defined by one of the following symptoms that include fever, pain, passage of dark urine, decrease in post transfusion haemoglobin concentration, increase in LDH levels [18].
Clinical Significance of DHTR
The DHTR related data has been presented by French HV system and described in SCD patients & patients presenting with previous allo- immunization/ previous DHTR. As per French HV system, DHTRs are the most common diagnosis to be misclassified as “idiopathic”, “other diagnosis” or “causes not related to transfusion” [18].
The frequency of DHTR in SCD patients is underestimated because its symptoms mimic those of vaso-occlusive crisis and antibodies are often not detectable [18]. The mortality attributable to DHTR is in the range of 5%-10%, which is quite significant and can be a limiting factor for good patient outcome [18, 19]. Early diagnosis of DHTR is pivotal, as further transfusions may exacerbate the patient’s clinical condition. [18].
In present study, incidence of DHTR in prospective arm was 0.061% (2/3,277), whereas in retrospective arm it was 0%, (0/15,660), this is statistically significant, p<0.05, (p=0). In our study it was realised that DHTR is an important diagnosis in patients with haematological malignancies and patients with history of random transfusions in resource poor set ups. Also, it is a significant contributor to patient morbidity if left untreated.
It is imperative for the department of Transfusion medicine to undertake regular audits to study different component requirements so as to improve component separation to avoid wastage and shortage. Regular clinical meetings on transfusion medicine for indications of different components are necessary to achieve judicious use of components [19].
Conclusion
Active surveillance of TRs has provided a true picture of the incidence of TRs. Two un reported DHTR cases were reported. DHTRs are under reported TRs due to lack of knowledge and vigilance. More studies are needed to evaluate the true incidence of DHTRs. No severe or life-threatening TRs were found during the present study.
In our study, FNHTRs constituted the most frequently reported TR in both prospective & retrospective analysis which is in line with other peer group studies. This study shows statistically significant difference in incidence of TRs reported by passive reporting and Active HV by TM personnel. It can be concluded that adopting Active HV for assessment of incidence of TRs can make statistically significant differences in the reporting; this area needs more comprehensive studies.
References
-
WHO (2012) Global Consultation on Haemovigilance. Jointly organized by WHO HQ/Geneva, Sharjah Blood Transfusion and Research Center and the Government of the United Arab Emirates, in collaboration with the International Haemovigilance Network and the International Society of Blood Transfusion, pp: 1-51.
-
Bisht A, Marwaha N, Kaur R, Gupta D, Singh S (2018) Haemovigilance Programme of India: Analysis of transfusion reactions reported from 2013 to April 2016 and key recommendations for blood safety. Asian J Transfus Sci 12(1): 1-7.
-
Somagari DR, Sriram CS, Rachamalla CKV, Dutta UC, Chaliha T, et al. (2015) Haemovigilance study at a tertiary care hospital in the north‐east of India. ISBT Science Series 10(2): 61-64.
-
Rabeya Y, Kahar AHA, Leong CF (2011) An audit of reported acute transfusion reactions in Universiti Kebangsaan Malaysia Medical Centre. Malays J Pathol 33(1): 25-29.
-
Sahu A, Bajpai M (2019) Determining the true incidence of acute transfusion reactions: A surveillance at a specialized liver center. Hematol Transfus Cell Ther 42(4): 326-332.
-
Agnihotri N, Agnihotri A (2016) Active Hemovigilance significantly improves reporting of acute non-infectious adverse reactions to blood transfusion. Indian J Hematol Blood Transfus 32(3): 335- 342.
-
Raval JS, Mazepa MA, Russell SL, Immel CC, Whinna HC, et al. (2015) Passive reporting greatly underestimates the rate of transfusion-associated circulatory overload after platelet transfusion. Vox Sang 108(4): 387-392.
-
Narick C, Triulzi DJ, Yazer MH (2012) Transfusion- associated circulatory overload after plasma transfusion. Transfusion 52(1): 160-165.
-
Popovsky M, Robillard P, Schipperus M, Stainsby D, Tissot JD, et al. (2011) Working Party On Haemovigilance. International Society of Blood Transfusion, pp: 1-12.
-
Shivgunde PP, Besekar SM, Bhojwani KM, Bhojwani DG (2018) Knowledge, attitude and practice of haemovigilance amongst healthcare professionals in Nashik, Maharashtra, India. International Journal of Basic & Clinical Pharmacology 7(5).
-
Sapkota A, Poudel S, Sedhain A, Khatiwada N (2018) Blood Transfusion Practice among Healthcare Personnel in Nepal: An Observational Study, Journal of Blood Transfusion 2018: 6190859.
-
Bhattacharya P, Marwaha N, Dhawan HK, Roy P, Sharma RR (2011) Transfusion related adverse events at the tertiary care center in North India: an institutional hemovigilance effort. Asian J Transfus Sci 5(2): 164-170.
-
Kumar P, Thapliyal R, Coshic P, Chatterjee K (2013) Retrospective evaluation of adverse transfusion reactions following blood product transfusion from a tertiary care hospital: a preliminary step towards hemovigilance. Asian J Transfus Sci 7(2): 109-115.
-
Narvios AB, Lichtiger B, Neumann JL (2004) Underreporting of minor transfusion reactions in cancer patients. Med Gen Med 6(2): 17.
-
Vamvakas EC, Pineda AA, Reisner R, Santrach PJ, Moore SB (1995) The differentiation of delayed hemolytic and delayed serologic transfusion reactions: incidence and predictors of hemolysis. Transfusion 35(1): 26-32.
-
Rieux C, Brittenham G, Bachir D, Meyer ED, Boudjedir K (2019) Delayed hemolytic transfusion reaction in the French hemovigilance system. Transfus Clin Biol 26(2): 109-111.
-
Narbey D, Habibi A, Chadebech P, Dessap AM, Khellaf M, et al. (2017) Incidence and predictive score for delayed hemolytic transfusion reaction in adult patients with sickle cell disease. Am J Hematol 92(12): 1340-1348.
-
CDC (2021) National healthcare Safety Network Biovigilance Component Hemovigilance Module Surveillance protocol, pp: 1-31.
-
Hulwan AB, Kanetkar SR, Jagtap SV, Kale PP (2019) Pattern of utilization of blood and blood components in a teaching hospital. J Datta Meghe Inst Med Sci Univ 14(2): 61-66.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet