Combined Tumor-A Tumor with Features of Malignant Melanoma and Squamous Cell Carcinoma-A Case Report and Review of Literature
Squamo-melanocytic tumors are very rare. The most common sites are head and neck followed by extremities. It consists of two distinct malignant tumors with epithelial and melanocytic components, hence classified as combined tumor. These tumors represent a diagnostic challenge and histopathological examination plays an important role in early diagnosis as well as treatment. We present a case of combined tumor that is malignant melanoma with squamous cell carcinoma in a 65 year old female patient to highlight its rarity as well as clinical and histomorphological features.
Introduction
Cutaneous tumors having two different cell types can be seen within the same lesion. These are very rare and the most common sites are head and neck followed by extremities [1]. Amongst these, are squamo-melanocytic tumors which consist of two distinct malignant cellular components that is epithelial and melanocytic components. Till date, only 37 cases of squamo- melanocytic tumors have been described [2].
We present a case of combined tumor that is acral lentiginous malignant melanoma and squamous cell carcinoma in a 65 year old female patient. The tumor was arising from medial aspect of right foot.
Case Report
A 65 year old female patient presented with wound on right foot which was followed by trauma 2 years back. The lesion was blackish in colour and later resulted in ulcer.

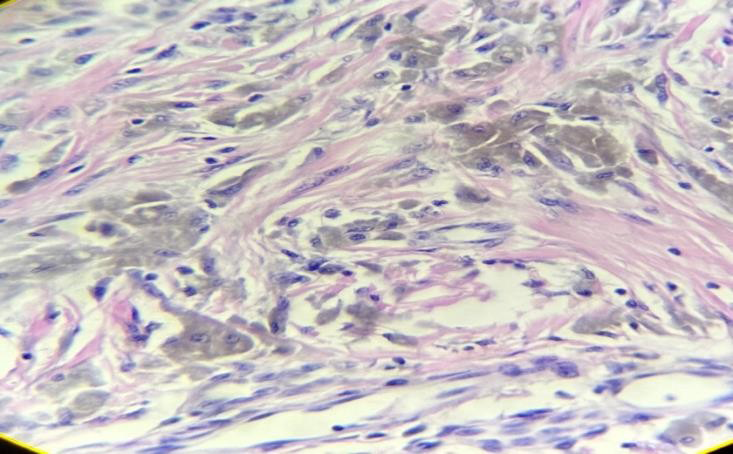
The wound was initially of size of peanut which gradually increased to current size of 3 x 3 cm. There was no history of pus discharge. Inguinal lymph nodes wre not palpable. On USG there was no evidence of metastasis. Incisional biopsy was performed and sent for histopathological examination. Histopathological examination revealed a combined tumor with features of malignant melanoma and squamous cell carcinoma. Tumor cells were arranged in sheets and nests showing highly atypical pleomorphic nuclei and ample amount of cytoplasm loaded with melanin pigment. These cells were spindle to epitheloid and were distributed in the superficial dermis, dermoepithelial junction as well as showing transepidermal invasion in a Pagetoid fashion. Arising from epidermis was seen a squamous cell carcinoma , the tumor cells were arranged in cords and trabeculae showing round to polygonal shape with enlarged hyperchromatic and pleomorphic nuclei, prominent nucleoli and keratin pearls. The stroma showed dense lymphoplasmocytic reaction.
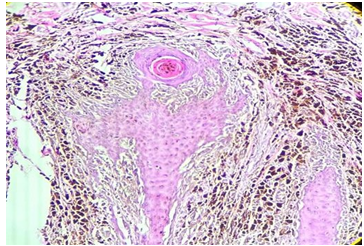
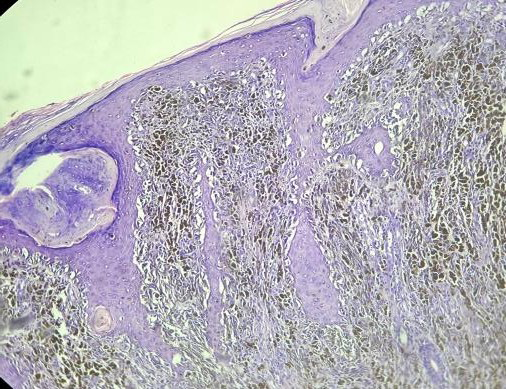
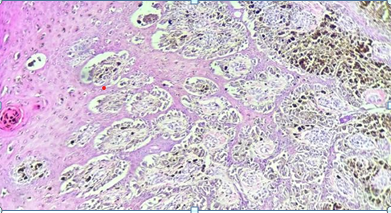
Considering these features , the tumor was diagnosed as a combined tumor that is malignant melanoma and squamous cell carcinoma. Malignant Melanoma was acral lentiginous melanoma with Breslows thicknes of 4 mm. Immunohistochemistry was adviced.
Discussion
The term squamous melanocytic tumor was first coined by Rosen [3] to describe a neoplasm composed of squamous cell carcinoma admixed with malignant melanoma.
Squamo-melanocytic tumors are classified into 4 subtypes : I. Collision tumors are two independent neoplasms which are close to each other but neoplastic cells do not mix. II. Combined tumors are composed of two distinct neoplasms of malignant cells that fuse imperceptibly. III. Biphenotypic tumors which coexpress immunohistochemistry markers and have the same molecular properties in both cell components. They arise from a common stem cell precursor that undergoes divergent differentiation IV. Colonized tumors are where tumor cell population permeates and colonizes another pre- existing tumor [4].
The presence of melanoma component in combined tumors is very rare [5]. The rarity of squamo- melanocytic tumor limits what is known about its incidence and prognosis and hence referred as tumor having uncertain biological potential [6]. Acral melanoma as known as acral lentiginous melanoma is seen over hands and feet involving palms and soles as well as fingers and toes which is the least common of all melanomas. Clinically, it begins as a black coloured macule which progresses to nodule, finally showing ulceration and bleeding [7]. Similar observation was seen in our case. The average age is 68.5 years with male predominance [8].
Microscopic examination of these tumors reveal sheets and irregular nests of malignant squamous cells intermingling with large atypical pigmented dendritic cells.
Immunohistochemistry shows melanocytic cells with positivity for Melan A, HMB 45, SOX 10, while squamous cells express positivity for CKAE1/AE3, CK-5/6, Epithelial membrane antigen [9]. The treatment guidelines for acral melanoma is excision with clinical margins depending upon Breslows thickness. Radiation therapy and chemotherapy are required for metastasis.
Conclusion
Squamo-melanocytic tumors are very rare and require a high degree of suspicion as they are highly invasive having increased risk of distant metastasis and hence require aggressive treatment. Histopathological examination with immunohistochemistry are indispensible towards making a diagnosis.
References
-
Satter EK, Metcalf J, Lountzis N, Elston DM (2009) Tumors composed of malignant epithelial and melanocytic populations: a case series and review of the literature. J Cutan Pathol 36(2): 211-219.
-
Cornejo KM, Deng AC (2013) Malignant Melanoma Within Squamous Cell Carcinoma and Basal Cell Carcinoma: Is It a Combined or Collision Tumor?--a Case Report and Review of the Literature. The American Journal of Dermatopathology 32(2): 226-234.
-
Jour G, Paniz-Mondolfi A, Reidy J, Cressey BD, Rosenthal S (2014) Squamomelanocytic tumor: a case report and further insights into its possible histogenesis. Am J Dermatopathol 36(6): 517-521.
-
López-Llunell C, Garbayo-Salmons P, Cañada MG, Artacho ES, Fernández-Sartorio C (2023) Squamomelanocytic Tumors: A Singular Case Report and Comprehensive Review. Indian J Dermatol 68(1): 122.
-
Kochoumian E, Kazlouskaya V, Mangold A, Lal K, Maia-Cohen S, et al. (2015) Tumor with the features of both squamous cell carcinoma and melanoma (melanocarcinoma). Indian Dermatol Online J 6(3): 217- 219.
-
Miteva M, Herschthal D, Ricotti C, Kerl H, Romanelli P (2009) A rare case of a cutaneous squamomelanocytic tumor: revisiting the histogenesis of combined neoplasms. Am J Dermatopathol 31(6): 599-603.
-
Niamh L, Wilson N, Calonje JE (2009) Squamomelanocytic Tumor: An Unusual and Distinctive Entity of Uncertain Biological Potential. The American Journal of Dermatopathology 31(5): 495-498.
-
Plaza AJ, Suster D, Perez-Montiel D (2007) Expression of Immunohistochemical Markers in Primary and Metastatic Malignant Melanoma: A Comparative Study in 70 Patients Using a Tissue Microarray Technique. Applied Immunohistochemistry & Molecular Morphology 15(4): 421-425.
-
Bristow IR, Berker DAD, Acland KM, Turner RJ, Bowling J (2010) Clinical guidelines for the recognition of melanoma of the foot and nail unit. J Foot Ankle Res 13: 25.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet