The Sezary Syndrome: A Rare case of Cutaneous T cell Lymphoma
Sezary syndrome is uncommon variant of cutaneous T-cell lymphoma (CTCL) characterized by erythroderma, pruritus and atypical lymphocytes with cerebriform nuclei. Hereby, the authors present a rare case of 60 years male with multiple hyperpigmented scaly plaques over face, bilateral upper, lower limbs, abdomen and trunk since 6 months. On Peripheral smear examination revealed Sezary cells of intermediate to large size with cerebriform nuclei with scant blue cytoplasm. Skin biopsy of the patient revealed atypical lymphoid infiltrate in the superficial dermis characterized by small cells with irregular nuclear contour and hyperchromatic chromatin (Sezary Cells). Hence there is a need for skin biopsies in patients with erythrodermic lesion with suspicion for Cutaneous T cell Lymphoma.
Introduction
Primary cutaneous lymphomas are a heterogeneous group of extra nodal non-Hodgkin lymphomas which are confined to the skin. In contrast to nodal non-Hodgkin lymphoma which is B-cell derived. Two-thirds of primary cutaneous lymphomas are T-cell derived and are classified as Mycosis fungoides.
Sezary cases can either have T or B cells origin and are called cutaneous T-cell lymphomas or cutaneous B-cell lymphomas (CBCL) respectively. The indolent forms of cutaneous lymphomas include mycosis fungoides (MF), lymphomatous papulosis and anaplastic large T-cell primary lymphoma. The most aggressive form includes Sezary syndrome (SS) which is characterized by complete effacement of the nodal architecture by infiltrating Sezary cells and have an adult onset condition [1, 2, 3].
Cutaneous T cell Lymphomas have increased risk of secondary cancers such as melanoma, lung cancer, and bladder cancer and other non-Hodgkin lymphomas. When neoplastic cells of Mycosis fungoides are found in the blood, the condition is called Sézary syndrome [4]. Both mycosis fungoides and SS have as cell of origin the skin resident CD45RO+ effector memory T cell.
Cutaneous B-cell lymphomas (CBCLs) have clinically indolent behaviour with Prominent dermal B cell infiltrates present and B cell collections are typically not found in normal skin and are rarely observed in reactive conditions or other types of cutaneous lymphomas [5].
Case Report
A 60-year-old male presented with multiple hypopigmented scaly plaques-like lesions and itching all over the body for the past 6 months. He was a known case of type 2 diabetes mellitus and had a history of accelerated hypertension, for which he was on medication. On physical examination, the patient had multiple hyperpigmented scaly plaques present over the face, bilateral upper limbs, bilateral lower limbs, abdomen, and trunk. Erythroderma is the key feature for diagnosis and is defined by involvement of >80% of the body surface.
The patient also had generalized odema and lymphadenopathy. LN and Bone marrow Biopsy was not done as patient expired soon after admission. Complete hemogram revealed mild anemia with Hb of 10.0 g/dl, adequate platelet count and elevated leucocyte count (TLC – 33,200). Peripheral smear examination revealed Atypical Lymphocytes of (Sezary cells) intermediate to large size

with cerebriform nuclei and scant blue cytoplasm. By manual calculation on peripheral smear 30 % were of atypical lymphoid cells (Sezary cells). Owing to the presence of multiple scaly plaques over trunk, limbs, face and skin biopsy was taken in 10% neutral buffer formalin and sent for Histopathological examination.
Grossly: The Skin with subcutaneous tissue totally measuring 1 x 0.3 x 0.2 cm. Routine processing of the biopsy was done and the section were taken.
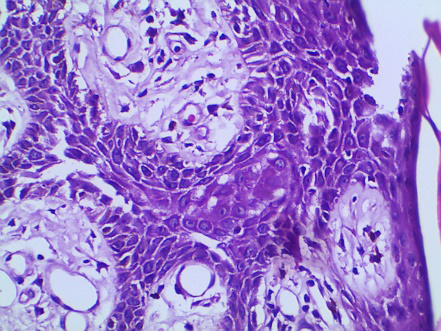
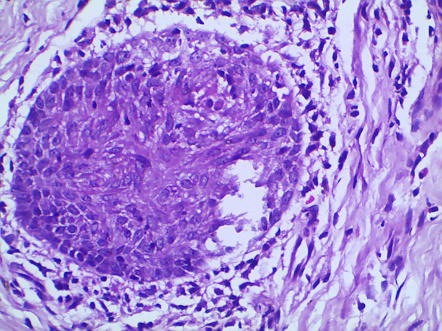
Microscopy: Atypical lymphoid infiltrate in the superficial dermis characterized by small Cells with irregular nuclear contour and hyperchromatic chromatin with epidermotropism.
On IHC Revealed Positivity for T Cell Markers: CD3 and CD4.
Figures (1-3): Showing Exfoliative Scaly Lesions and Marked Erythroderma Over the Face, Trunk and Lower Limbs.
Discussion
Primary cutaneous lymphomas are a heterogeneous group of extranodal non-Hodgkin lymphomas which, by definition, are confined to the skin at the time of diagnosis but have the potential for secondary involvement in lymph nodes, blood, and viscera. Skin lesions include patches or plaques with erythroderma that may be localized or disseminated. In some patients, the disease remains limited to the skin for many years, while in others, it may progress more quickly to extracutaneous involvement and has a worse prognosis. Sezary Syndrome is an erythrodermic and pruritic form of CTCL, characterized by peripheral lymphadenopathy and the presence of neoplastic T-cells with cerebriform nuclei (Sézary cells). Peripheral blood smears show flower or cloverleaf cells, and similar morphology is also seen in extracutaneous sites. In Sezary, most of the tumor cells are concentrated in the dermis only, but the epidermal component may also be involved. For diagnosis, it definitely requires clinical evidence of patch- and plaque-stage disease, which can be confused with different types of lymphoma. In patients with primary cutaneous lymphoma, along with disseminated skin disease or lymphadenopathy, flow cytometry and bone marrow biopsy are recommended. The recommended flow cytometric panel includes CD3, CD4, CD5, CD7, CD8, CD25, and CD30 [6].
In pathogenesis of cutaneous lymphomas there is chronic activation of T-cells by antigen-presenting cells resulting in accumulation of mutations that results in development of neoplastic cells. There is also a hypothesis that large plaque parapsoriasis and pityriasis lichenoides chronica would represent lymphocytic dyscrasias that could correspond to the link between polyclonal processes and MF [7, 8].
The diagnosis of MF, especially for patch/plaque stage disease, is difficult, as many of its clinical and pathologic features are non-specific and overlap with reactive processes. Many patients will have symptoms attributed to eczema, psoriasis or parapsoriasis for years prior to obtaining a definitive diagnosis. The median time from symptom onset to diagnosis in a retrospective series is 3 to 4 years, but may exceed upto fouth decade [9, 10, 11].
The histopathologic findings in the skin often resemble those observed in MF, with less prominent epidermotropism, though findings in skin biopsies maybe paradoxically subtle and non-specific. As in MF, immunohistochemical studies shows predominance of CD4 marker and loss of pan T-cell markers. Lymph node involvement is characterized by complete effacement of the nodal architecture by infiltrating Sezary cells. In Sezary Syndrome, clonal T cells are generally CD3+CD4+and CD8. In MF, the aberrant loss of pan-T-cell antigens, including CD2, CD3, CD4, CD5, CD7 and/or CD26 is observed. Of these, the aberrant loss of CD7 or CD26 expression is most common, being observed in most cases. CD7and CD26 is highly sensitive and specific for SS [12, 13, 14, 15].
In MF, the cytological aspects and the architectural pattern of the cellular infiltrate correspond to the clinical stage of the disease along with epidermotropism of atypical lymphocytes. Atypical lymphocytes have a large and hyperchromatic nucleus with cerebriform contours . In the early patch stages and in erythrodermic phase, the number of atypical lymphocytes infiltrating the epidermis is scarce, and its infiltration is markedly increased in plaque and tumor stage. In some cases epidermotropism may be absent in plaques and tumors, making the diagnosis difficult. Other typical pathological findings are Pautrier’s microabscesses and presence of lymphocytes in the basal layer may also be observed in MF . The absence of spongiosis favors the diagnosis for MF however, it has low specificitiy. CD4+ T cell population with CD4:CD8 ≥ 10 [16, 17, 18].
Conclusion
Cutaneous lymphomas are rare extranodal non-Hodgkin lymphomas.Sezary syndrome is a rare aggressive leukemic T cell lymphoma that presents with peripheral blood involvement, erythroderma and lymphadenopathy. Inspite of having good prognosis, with high survival rates in most cases, MF patients suffer from skin lesions that significantly decrease the quality of life. Thus, clinical recognition and correct management are essential for early diagnosis and appropriate care of these patients.
Conflict of Interest
The authors have no conflict of interest.
References
-
Johnson LDS, Banerjee S, Kruglov O, Viller NN, Horwitz SM, et al. (2019) Targeting CD47 in Sézary syndrome with SIRPαFc. Blood Adv 3(7): 1145-1153.
-
Van-de-Velde V, Zhou Y (2019) Existing and Emerging Therapies for Cutaneous T-Cell Lymphoma. J Cutan Med Surg 23(3): 319-327.
-
(2022) PDQ Cancer Information Summaries. National Cancer Institute, US.
-
Larocca C, Kupper T (2019) Mycosis Fungoides and Sézary Syndrome: An Update. Hematol Oncol Clin North Am 33(1): 103-120.
-
Oschlies I, Wehkamp U (2022) Cutaneous B cell lymphomas: standards in diagnostic and clinical work- up. Hints, pitfalls and recent advances. Histopathology 80(1): 184-195.
-
Sanches JA , Cury-Martins J, Abreu RM, Miyashiro D, Pereirac J (2021) Mycosis fungoides and Sézary syndrome: focus on the current treatment scenario. Anais Brasileiros de Dermatologia 96(4): 458-471.
-
Sibbald C, Pope E (2016) Systematic review of cases of cutaneous T-cell lymphoma transformation in pityriasis lichenoides and small plaque parapsoriasis. Br J Dermatol 175(4): 807-809.
-
Cerroni L (2017) Past, present and future of cutaneous lymphomas. Semin Diagn Pathol 34(1): 3-14.
-
Kim YH, Liu HL, Mraz-Gernhard S, Varghese A, Hoppe RT (2003) Long-term outcome of 525 patients with mycosis fungoides and Sezary syndrome: clinical prognostic factors and risk for disease progression. Arch Dermatol 139(7): 857-866.
-
Doorn RV, Haselen CMV, Vader PCVV, Geerts ML, Heule F, et al. (2000) Mycosisfungoides: disease evolution and prognosis of 309 Dutch patients. Arch Dermatol 136(4): 504-510.
-
Arulogun SO, Prince HM, Lade S, Ryan GF, Blewitt O, et al. (2008) Long-term outcomes ofpatients with advanced- stage cutaneous T-cell lymphoma and largecell transformation. Blood 112(8): 3082-3087.
-
willemze R, van Vloten WA, Hermans J, Damsteeg MJ, Meijer CJ (1983) Diagnostic criteria in Sezary’s syndrome: a multiparameter study ofperipheral blood lymphocytes in 32 patients with erythroderma.J Invest Dermatol 81(5): 392-397.
-
Boumsell L, Bernard A, Reinherz EL, Nadler LM, Ritz J, et al. (1981) Surface antigens on malig-nant Sezary and T-CLL cells correspond to those of mature T cells. Blood 57(3): 526-530.
-
Vonderheid EC, Bernengo MG, Burg G, Duvic M, Heald P, et al. (2002) Update onerythrodermic cutaneous T-cell lymphoma: report of the Interna-tional Society for Cutaneous Lymphomas. J Am Acad Dermatol 46(1): 95- 106.
-
Hristov AC, Vonderheid EC, Borowitz MJ (2011) Simplified flow cytometricassessment in mycosis fungoides and Sezary syndrome. Am J ClinPathol 136(6): 944-953.
-
Kim EJ, Hess S, Richardson SK, Newton S, Showe LC, et al. (2005) Immunopathogenesis and therapy of cutaneous T cell lymphoma. J Clin Invest 115(4): 798-812.
-
Jawed SI, Myskowski PL, Horwitz S, Moskowitz A, Querfeld C (2014) Primary cutaneous T-cell lymphoma (mycosis fungoides and sezary syndrome): part i diagnosis: clinical and histopathologic features and new molecular and biologic markers. J Am Acad Dermatol 70(2): 205.
-
Cerroni L (2018) Mycosis fungoides-clinical and histopathologic features, differential diagnosis, and treatment. Semin Cutan Med Surg 37(1): 2-10.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet